Article Text

Summary
Papillary fibroelastomas (PFEs) are rare cardiac tumors. Despite their benign nature, they are associated with a high risk of embolic complications including stroke. Endovascular treatment has been reported as a safe procedure in patients with myxoma, the most common type of primary cardiac tumor. A case of ischemic stroke due to embolization of a PFE successfully treated with a single pass of a retrievable stent is described. A 64-year-old patient with a right middle cerebral artery syndrome was treated with an intravenous and endovascular protocol as a revascularization procedure. Mechanical thrombectomy resulted in total recanalization with clinical improvement. Histological examination of the clot showed pathological features of a typical PFE. The endovascular treatment was safe and effective. With mechanical embolectomy it is possible to obtain and analyze pathological specimens, enabling the diagnosis of uncommon strokes.
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Background
Papillary fibroelastoma (PFE) tumors are classified as benign endocardial tissue composed of fibrous elastic fibers and smooth muscle cells. They are the most common benign cardiac tumors after auricular myxoma. The histogenesis of PFE is still unclear. Several hypotheses about the etiology have been proposed. Among them, the most recognized is that they are hamartomas, organized thrombi or inflammatory foci developed as a result of an unusual response to different endocardial tissue aggressions (infections, surgery, radiotherapy) or hemodynamic stress. However, other authors argue for a purely neoplastic origin. Its characteristic morphology consists of a short papillary pedicle and multiple branch-like projections similar to a ‘sea anemone’. In 85% of cases PFEs are located in the endocardium valves, the tricuspid and aortic valves being most frequently affected.1 ,2 Smaller lesions near the lines of valvular closure are termed Lambl’s excrescences.2 ,3 Despite the benign nature of this tumor, it is associated with a high risk of embolic complications including neurological deficit.1–5 Endovascular therapy is increasingly used for arterial occlusion in acute stroke. In addition, the development of mechanical embolectomy devices has permitted analysis of pathologically retrieved specimens.6 The use of endovascular therapy in myxoma-related ischemic stroke has been reported.7 ,8 We describe a case of acute ischemic stroke treated with mechanical thrombectomy in which the histopathological study of the retrieved thrombus showed a tumorous embolus of a PFE.
Case presentation
A 64-year-old right-handed woman with dyslipidemia and no other previous medical and surgical history of interest presented with a right middle cerebral artery syndrome of 70 min evolution. The NIH Stroke Scale (NIHSS) score was 16. Conventional non-contrast CT ruled out intracranial hemorrhage and showed a right proximal middle cerebral artery (MCA) hyperdense artery sign. Intravenous recombinant tissue plasminogen activator (rtPA) was administered 90 min after clinical onset without significant clinical improvement. Brain CT angiography revealed right M1 segment occlusion (figure 1A) and a wide penumbra area was apparent in the perfusion protocol CT scan (figure 1B). The endovascular procedure began 4 h after clinical presentation. Mechanical thrombectomy with only one pass of the Solitaire FR 4×20 mm (EV3) retrievable stent was successful, achieving total recanalization (Thrombolysis In Cerebral Infarction (TICI) 3) without a heparin bolus (figure 2). Although the patient developed hemorrhagic transformation of the stroke (PH1 score, <30% of the ischemic area with mild edema), clinical improvement was seen with an NIHSS score of 3 at discharge. Histology of the 1×0.8 cm clot collected showed a fragment of white granular surface of soft consistency and papilliform appearance. After H&E staining, the sections showed branching papillary lesions consistent with PFE (figure 3). Ancillary tests including cardiac imaging with echocardiography evaluation (transthoracic/transesophageal) and cardiac MR performed twice during the 1-year follow-up period did not show any further relevant findings.

(A) Brain CT angiography showing M1 right middle cerebral artery occlusion. (B) Perfusion protocol CT showing prolonged mean transit time with corresponding decreased cerebral blood flow and cerebral blood volume consistent with hypoperfusion.
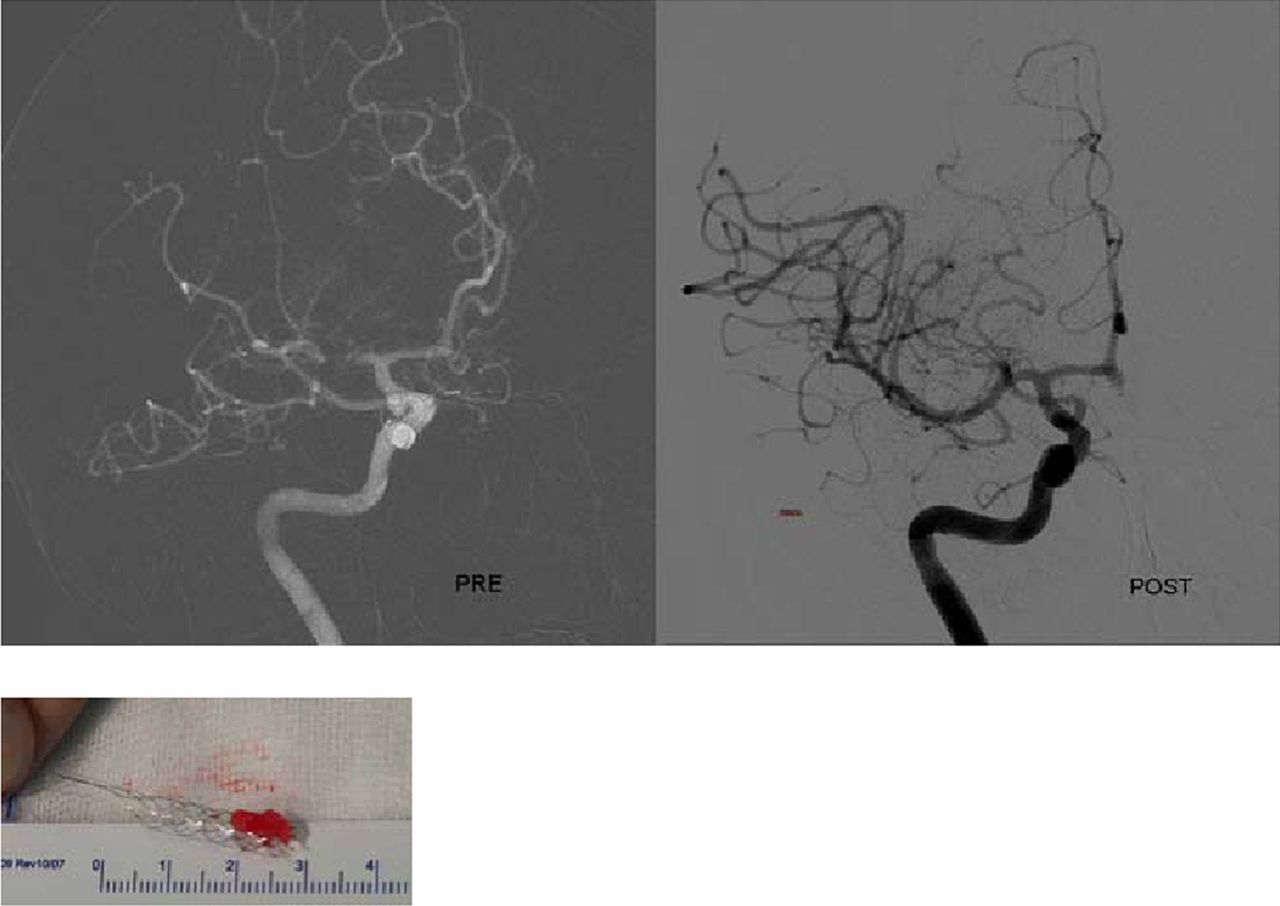
Angiography of right M1 middle cerebral artery occlusion before stent insertion (pre) and complete recanalization after one pass of the Solitaire FR self-expandable stent (post).

{kind=link}
{kind=link}
{kind=link}
Pathological features of the clot. (A) Lesion with branch-like papillary morphology (stain: H&E, magnification: 20×). (B) Connective tissue composed of elastic fibers and collagen surrounded by a single layer of hyperplastic endocardial cells (stain: H&E, magnification: 100×).
Discussion
The clinical presentation of PFE is highly variable, ranging from asymptomatic to severe thromboembolic complications, myocardial ischemia and stroke. Two mechanisms can explain the formation of emboli in PFE: dislodgement of the tumor leaves or fibrin-platelet aggregation on the endocardial surface of these leaves. The fragile nature and frond-like papillary tissues of the tumor are factors favoring thromboembolism. The diagnosis of PFE is usually echocardiographic, but tumors of small size may be undetectable.1 ,2 In the case described here, the histological features of the clot and the absence of signs in the cardiology examinations indicate that total detachment of the tumor could be the cause of the brain embolism.
Successful thrombolytic therapy with intravenous rtPA in acute ischemic stroke patients with cardiac myxoma has been performed,7 and intra-arterial thrombolysis with urokinase has been demonstrated to be capable of causing partial recanalization.8 The mechanical thrombectomy procedure can be considered the most effective endovascular technique currently used in ischemic stroke, and is also a reliable and valuable diagnostic tool.6 Endovascular treatment has been previously reported as an effective procedure in patients with myxoma.9 In theses cases, mechanical thrombectomy with the use of intracranial retrieval stent systems enabled histological examination of the clot and therefore the etiology of the stroke was known. The case described here confirms the validity of these procedures for the treatment of stroke secondary to embolization of primary cardiac tumors. Another advantage of these techniques is that they provide a histological diagnosis of the stroke that can be useful in planning complementary studies.
Learning points
-
Mechanical thrombectomy can be safe and effective in the treatment of stroke secondary to cardiac papillary fibroelastoma.
-
Mechanical thrombectomy allows histological examination of the clot for diagnosis.
-
In small cardiac papillary fibroelastomas, total detachment of the tumor may be the cause of the brain embolism.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.