Article Text

Abstract
Syphilis is a resurgent sexually transmitted infection in the UK that is disproportionately diagnosed in patients living with HIV, particularly in men who have sex with men. Syphilis appears to present differently in patients with HIV, particularly in those with severe immunosuppression. Progression to neurosyphilis is more common in HIV coinfection and can be asymptomatic, often for several years. The presentations of neurosyphilis vary but can include meningitis, meningovascular disease, general paresis and tabes dorsalis. There is debate about the circumstances in which to perform a lumbar puncture, and the current gold standard diagnostics have inadequate sensitivity. We recommend a pragmatic approach to lumbar punctures, interpreting investigations and deciding when to consider treatment with a neuropenetrative antibiotic regimen.
- neurosyphilis
- syphilis
- HIV
Statistics from Altmetric.com
The changing face of syphilis
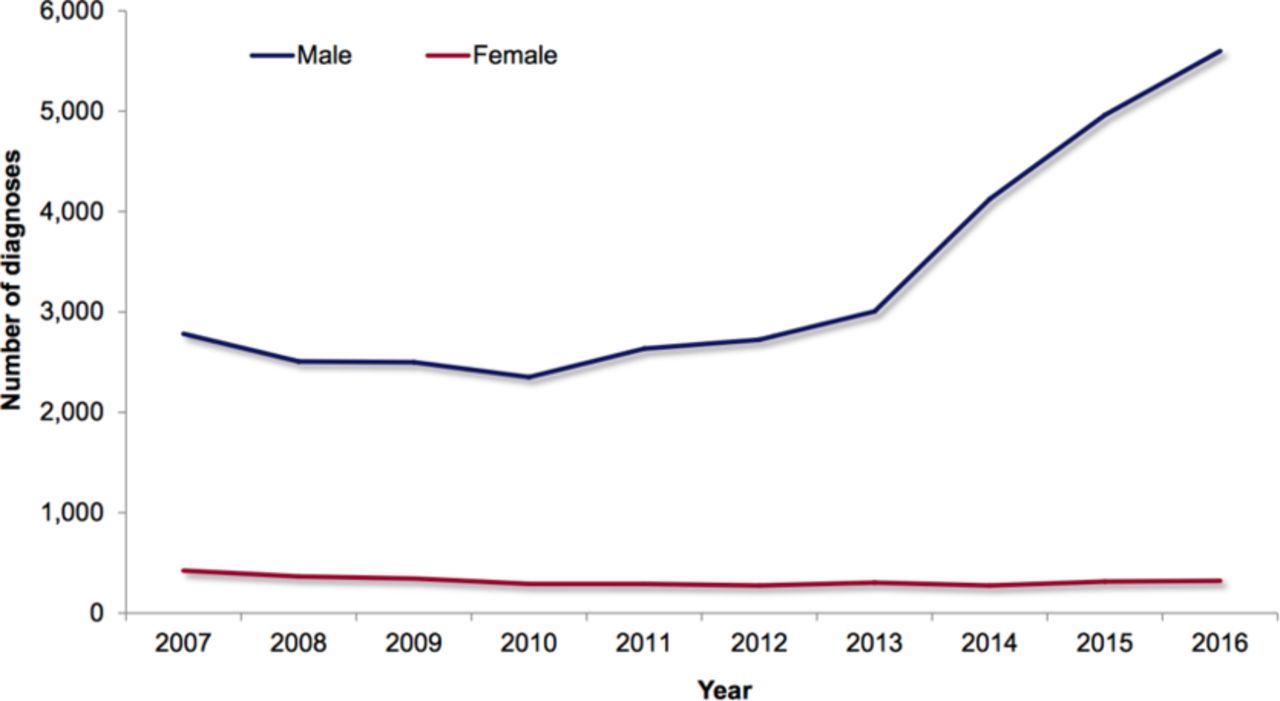
Syphilis, caused by the spirochaete bacterium Treponema pallidum, has seen a resurgence in high-income countries in recent years, particularly among men who have sex with men.1 The widespread availability of penicillin in the USA and other industrialised countries following World War II resulted in the incidence of syphilis falling from 76 per 100 000 population in 1945 to 4 per 100 000 in 1955–1957. After this period, syphilis rates became concentrated within men who have sex with men, and its incidence surged during the 1980s HIV/AIDS epidemic.1 In response to the fear induced by the epidemic, changes in sexual behaviour caused another decline, until recently where rates have again risen rapidly.1 2 In the USA, during 2014–2015, syphilis occurred in 7.5 cases per 100 000, the highest rate since 1994.3 There were similar trends in England where in 2016 there were 5920 cases (figure 1),4 12% higher than the previous year and the highest number of new diagnoses since 1949, with 80.9% of cases occurring in men who have sex with men.2
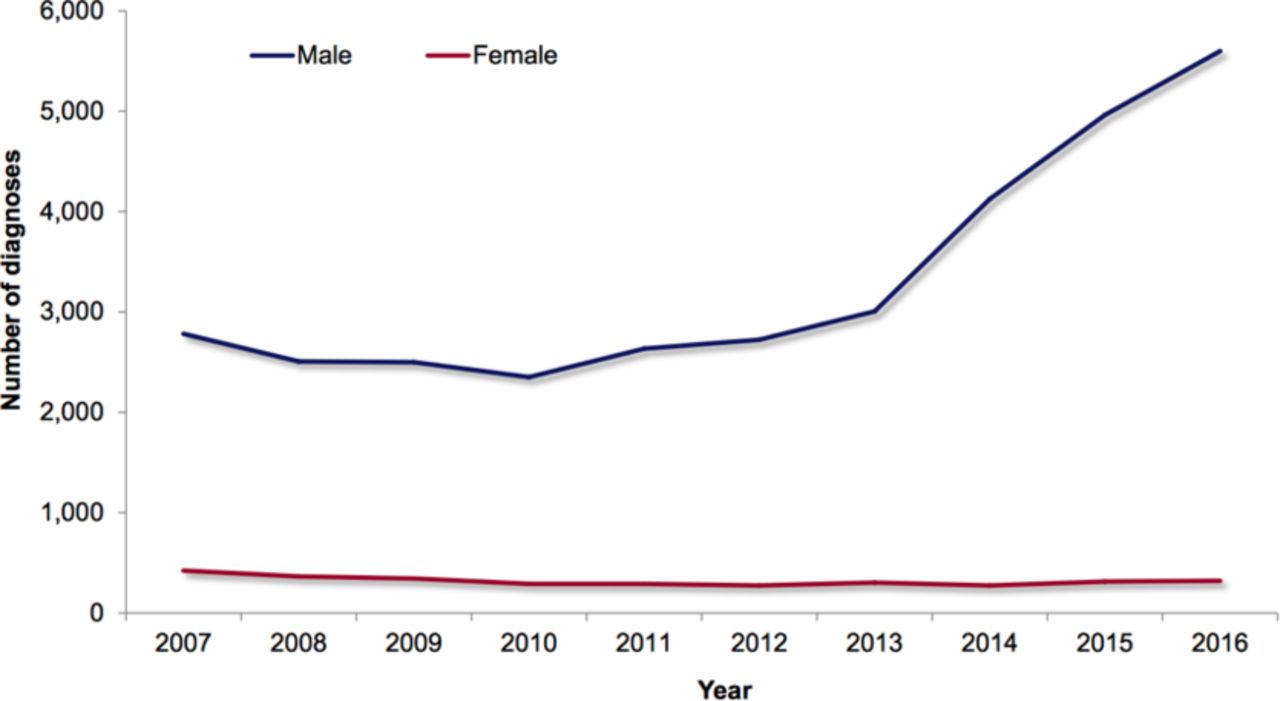
Number of syphilis infections in England between 2007 and 2016.4
Syphilis infection
Syphilis infection involves several stages. Primary syphilis classically presents 9–90 days after infection with a single, non-tender genital ulcer (chancre) representing the first site of T. pallidum invasion. If untreated, the primary infection progresses to secondary syphilis, typically 12 weeks, but sometimes up to 12 months after initial infection. The classical presentation of secondary syphilis is a rash that typically involves the trunk, may involve the hands or feet and may be accompanied by condylomata lata, wart-like lesions around the anogenital region. Latent syphilis results when both primary and secondary syphilis are not treated and is defined by serological proof of infection but no symptoms. It is divided into early and late latent syphilis, with early latent syphilis infectious and late latent syphilis, defined in the UK as more than 2 years after infection, found to generally be non-infectious.5 6
Syphilis progresses to tertiary disease in one-third of patients without treatment, roughly 20–40 years after primary infection.5 Tertiary syphilis involves a severe and self-destructive immune response to a persistent low level burden of T. pallidum.5 This can present as cardiovascular syphilis, gummatous syphilis, late benign syphilis or neurosyphilis.6 It is important to emphasise that neurological symptoms can occur during any phase of infection, and therefore neurosyphilis should only be considered tertiary when presenting in the late-latent period.5 Primary, secondary and early latent syphilis are collectively grouped together as early syphilis, and late latent and tertiary syphilis are grouped together as late syphilis.
Neurosyphilis
Neurosyphilis is a broad term used to describe the direct invasion of T. pallidum into the nervous system and can affect the brain, spinal cord and peripheral nerves.7 Approximately 25%–40% of patients have ‘neuroinvasion’ at some point, typically during the primary or secondary stage of infection, but most spontaneously clear the infection from the cerebrospinal fluid (CSF) without requiring treatment for neurosyphilis and potentially without having any symptoms.8 In patients whose immune system cannot clear the infection, neurosyphilis develops; this can also present with or without symptoms, the latter form known as asymptomatic neurosyphilis.7 There is great debate around the topic of asymptomatic neurosyphilis (discussed below).
Syphilis is often referred to as ‘the great imitator’ and it can present in countless ways. The clinical manifestations of neurosyphilis are similarly varied, and patients may remain asymptomatic for years. Levels of central neurological involvement can be classified into meningeal, vascular or parenchymatous forms with direct invasion of T. pallidum possible at each of these sites.9 Meningeal and vascular neurosyphilis are inflammatory processes that frequently coexist (meningovascular neurosyphilis), particularly in the early years of infection.10 Meningeal involvement can present as aseptic meningitis with symptoms such as headache, photophobia and neck stiffness and can lead to complications such as cranial nerve palsies.9 Vascular syphilis can affect the arterial supply of the brain or spinal cord resulting in ischaemic stroke and, depending on the arterial territory involved, can cause different neurological deficits. Neurosyphilis should therefore always be considered as a differential diagnosis in any patient with ischaemic stroke of unknown cause, particularly in young people.9 Parenchymal neurosyphilis is neurodegenerative in nature and can manifest as general paresis—characterised by memory deficit, emotional lability and psychosis—or tabes dorsalis (also known as syphilitic myelopathy) in which patients may develop sensory ataxia and neuropathic pain in the lower limbs.11 12 Parenchymal changes tend to arise years to decades after initial infection but are now extremely rare due to the widespread availability and prescribing of penicillin.11 13 A fourth, distinct and rare form of central neurosyphilis can emerge in gummatous syphilis, which causes space-occupying lesions that may result in seizures, focal neurological signs, raised intracranial pressure or progressive paraparesis or quadriparesis.9 Peripheral nervous system involvement is not the focus of this review and is less common but can include polyradiculopathy and peripheral neuropathy.14
The synergistic relationship between HIV and syphilis
HIV and syphilis affect similar patient groups. In 2002, the US Centers for Disease and Control Prevention reported the incidence of syphilis to be 77 times greater in HIV-infected individuals than in the general population.15 This is of particular significance because HIV and syphilis have a synergistic relationship wherein syphilis can increase the risk of HIV transmission and acquisition, while HIV can affect the presentation, diagnosis, progression and treatment response of syphilis.16 However, much of the evidence relating to this is in the context of advanced HIV and might not apply to those with CD4 counts ≥350 cells/µL and/or a suppressed HIV viral load.
In terms of HIV acquisition, syphilis causes transient immunosuppression and can weaken the host response to HIV, increasing the likelihood of exposure leading to HIV infection. In addition, chancres are particularly vulnerable, well vascularised sites for HIV to enter the bloodstream and establish primary infection.17 18
The impact of HIV on syphilis is explained by the immunodeficiency caused by HIV; also, the presentation of syphilis may be more severe or atypical, particularly in the severely immunosuppressed. These individuals are more likely to develop multiple, deeper or larger chancres and their primary and secondary infections can overlap.19 This trend continues in the context of neurosyphilis; a review of syphilis cases in Los Angeles between 2001 and 2004 showed a 2.1% incidence of neurosyphilis among those infected with HIV compared with 0.6% among those without HIV.20 The likelihood of developing neurosyphilis has been linked to the degree of immunosuppression caused by HIV, such that patients with a CD4 count of ≤350 cells/µL have a threefold increase in neurological involvement.21
Asymptomatic neurosyphilis
Asymptomatic neurosyphilis is a topic of significant debate and scientific uncertainty. Concerns arose from studies that reported a greater level of neurocognitive impairment in HIV-positive patients with previous early syphilis but no diagnosis of neurosyphilis—who were treated with standard benzathine penicillin G, which does not cross the blood–brain barrier—when compared with those without previous syphilis. Unfortunately, these studies did not consider confounding factors such as alcohol consumption, smoking history, CD4 count, HIV viral load, recreational drug use and other coinfections.22 23
Both pathogens can cause meningeal inflammation, leading to increased CSF penetration by the other infectious agent. Patients with concurrent HIV and syphilis infections have a higher CSF HIV viral load,17 which itself is associated with neurocognitive impairment.17 24 A recent prospective study found no association between neurosyphilis and cognitive impairment in HIV-positive individuals but did identify significantly higher levels of inflammatory markers that are associated with the development of cognitive impairment in the CSF of patients with neurosyphilis.25
A UK study of 64 HIV-positive patients with early syphilis, treated with a single dose of benzathine penicillin G, found only a low risk of asymptomatic neurosyphilis, with only one patient developing asymptomatic neurosyphilis, as determined by CSF variables.26 This contrasts with a study in the USA that found asymptomatic neurosyphilis in 22% of 46 HIV positive asymptomatic patients who underwent lumbar puncture.27 These differing rates of asymptomatic neurosyphilis probably reflect levels of immunosuppression, antiretroviral therapy (ART) status and severity of syphilis infection. The knowledge that syphilis causes neuroinflammation in HIV infection, coupled with uncertainties surrounding the prevalence, clinical significance and optimal treatment of asymptomatic neurosyphilis has left clinicians uncertain about whether all HIV-positive patients should either undergo a lumbar puncture and/or be treated with a neuropenetrative antibiotic regimen.
Diagnosis of neurosyphilis
The presence of syphilis infection and neurological symptoms should raise significant suspicion of neurosyphilis. The following investigations must be interpreted with an understanding of their limitations and in the context of the clinical picture.
Microscopy
Genital syphilis can be diagnosed by swabbing a chancre and performing dark-ground microscopy, which shows the presence of T. pallidum.5 This technique is still used in genitourinary medicine clinics and can be used on samples obtained from biopsies, including in suspected cases of neurosyphilis.
Blood tests
Syphilis can be difficult to diagnose due to the several weeks’ delay between exposure and seroconversion. When suspected, patients are screened with an ELISA (table 1). Other treponemes that affect humans include the endemic treponematoses bejel (T. pallidum subsp. endemicum) and yaws (T. pallidum subsp. pertenue), so a positive test needs to be taken in the context of the clinical picture and history.28 A confirmatory test called the T. pallidum haemagglutination (TPHA) or T. pallidum particle agglutination (TPPA) is then performed, although in some settings this may be the only treponemal-specific test performed. ELISA, TPHA and TPPA remain positive for life. In people with a positive TPHA/TPPA, either a venereal disease research laboratory (VDRL) or reactive plasma reagin (RPR) test is carried out; these detect anticardiolipin antibodies in the blood and are given as a titre that can assess burden of infection, monitor response to treatment and diagnose treatment failure or reinfection.5 28
How to interpret syphilis serology
CSF analysis
The diagnosis of neurosyphilis with CSF analysis is often difficult. CSF abnormalities include elevated white cell count (with predominance of lymphocytes), elevated protein and a reactive CSF VDRL or RPR. These CSF abnormalities must be taken in the context of the clinical findings.6 29 Headache and visual disturbance are strongly associated with symptomatic neurosyphilis in HIV-positive people; however, as described earlier, the manifestations are extremely variable and these symptoms are non-specific.9 Neurological symptoms and signs must be very carefully sought in patients with syphilis and HIV coinfection and the possibility of asymptomatic neurosyphilis borne in mind.30 In asymptomatic individuals, the diagnosis is based on CSF abnormalities alone and these may be less marked.9 Neurosyphilis may be the first presentation in a patient with HIV, so all patients diagnosed with neurosyphilis should be tested for HIV.
Several clinical and laboratory variables can aid the diagnosis of neurosyphilis in the context of HIV and help to decide which patients should undergo CSF examination and receive enhanced treatment with a neuropenetrative regimen (boxes 1 and 2). There is consensus that in the presence of neurological symptoms such as headache or altered mental state, a CSF analysis should be performed regardless of laboratory results. However, there is debate about the indications for CSF analysis in patients who are asymptomatic. European and Canadian guidelines state that patients with a CD4 count of ≤350 cells/µL or a VDRL/RPR titre of ≥1:32 should undergo lumbar puncture, although this differs from the CDC recommendation.31 32 Ghanem et al found these criteria to be most reliable in identifying asymptomatic neurosyphilis.27 The lack of systematic research into this area contributes to a lack of consensus on which patients will benefit from screening and enhanced treatment for neurosyphilis.
Indications for a lumbar puncture
Neurological signs
Ocular involvement
CD4 count <350 cells/µL*
Venereal disease research laboratory/reactive plasma reagin titre>1:32*
Antiretroviral therapy naïve*
*Consider.
Factors suggesting neurosyphilis
Neurological signs
Ocular involvement
Positive CSF test including: VDRL, RPR, TPHA, TPPA, PCR
CSF pleocytosis: >20 cells if antiretroviral therapy naïve, >10 cells if antiretroviral therapy exposed.
CSF, cerebrospinal fluid; RPR, rapid plasma reagin; TPHA, Treponema pallidum haemagglutination; TPPA, Treponema pallidum particle agglutination; VDRL, venereal disease research laboratory.
The CSF VDRL is the ‘gold standard’ in terms of specificity for neurosyphilis but has significant limitations; its variable sensitivity (30%–70%)%) means a non-reactive CSF VDRL does not exclude the diagnosis of neurosyphilis. However, because CSF VDRL is highly specific, a reactive CSF VDRL confirms the diagnosis.33 CSF RPR is easier to perform but has lower sensitivity than VDRL.34 CSF treponemal tests such as the TPPA can be used in conjunction with VDRL as they are highly sensitive but non-specific, and therefore a negative treponemal test excludes the diagnosis of neurosyphilis. Some studies suggest high-titre CSF TPPA results are more specific for neurosyphilis.6 33 CSF PCR, although not widely available, has sensitivity of 70%–76% and a specificity of 87%–92%.35
Even in centres where each of these tests is available, the results can often be inconclusive and the diagnosis may be made on CSF pleocytosis alone. Challenges arise here as HIV itself can cause CSF pleocytosis.9 Patients with neurosyphilis generally have a CSF white cell count >10 cells/µL. However, if an HIV-positive patient has positive syphilis serology and a non-reactive CSF VDRL, a cut-off of >20 cells/µL is often used.29 Clinicians need to be cautious when deciding an appropriate cut-off as patients on ART and/or with an undetectable plasma HIV viral load are less likely to have CSF pleocytosis, and therefore the lower cut-off of >10 cells/µL might still be appropriate in this group. It is, however, still unclear as to whether the pleocytosis is due to syphilis, HIV, a combination of both or an alternative diagnosis, so CSF pleocytosis is a poor diagnostic tool for neurosyphilis.29 A raised protein >0.45 g/L may also suggest neurosyphilis but again lacks specificity.36
This lack of an ideal diagnostic test has prompted research into new CSF diagnostic markers. The B-lymphocyte chemoattractant chemokine CXCL13 has proven to be the most promising and could be used independent of CSF pleocytosis and CSF VDRL.37 Levels decline after treatment so CXCL13 could potentially also be used as a marker of treatment response.38 If CXCL13 is to be used in clinical practice, we need its sensitivity and specificity needs to be established and to identify recommended cut-off values.38
Neuroimaging
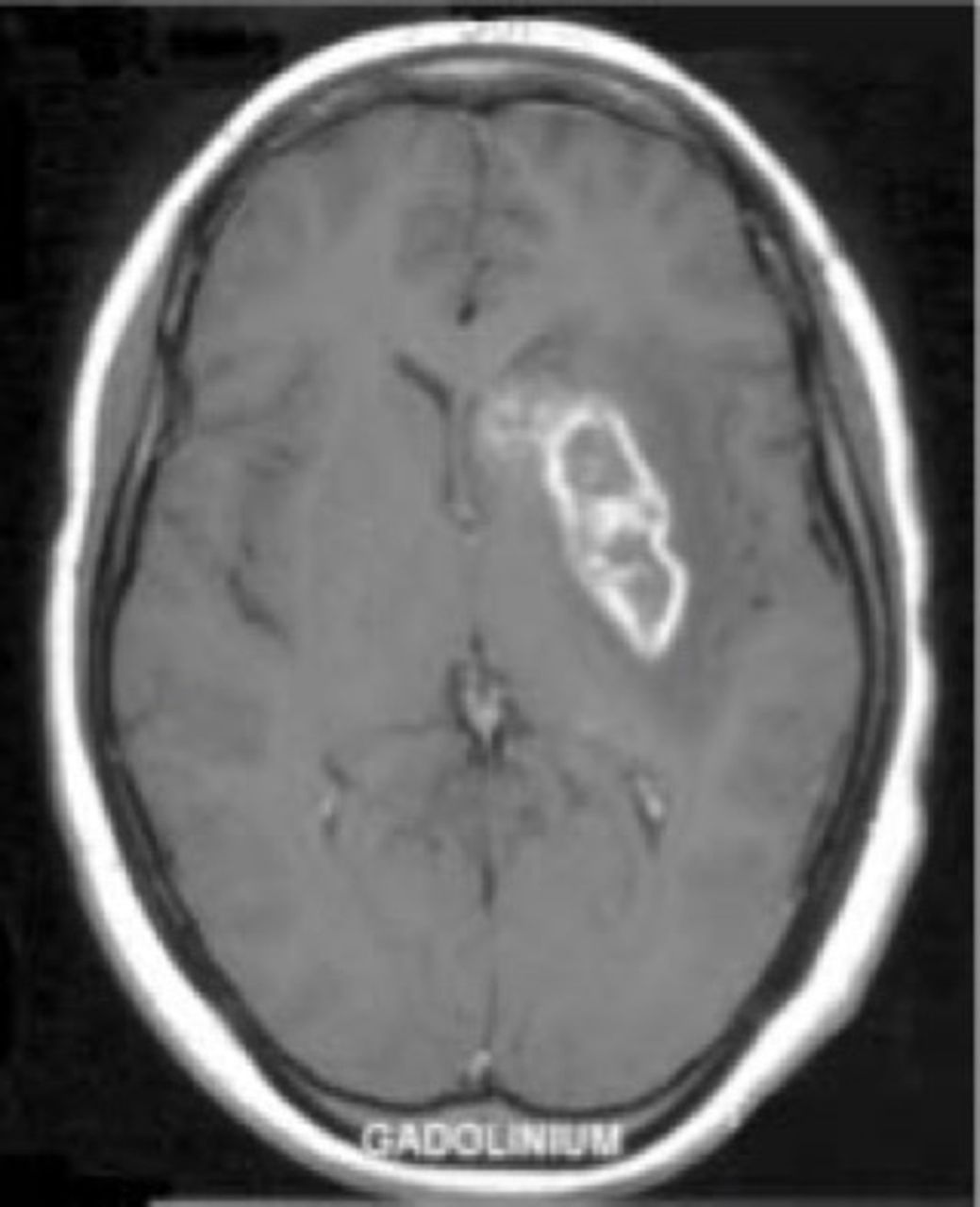
Imaging can sometimes help in diagnosing and monitoring of neurosyphilis, although no abnormality is specific for the condition and scans can be normal. Owing to the meningovascular inflammation that predominantly involves small-sized to medium-sized vessels, perhaps the most common findings are areas of infarction or haemorrhage—often within the middle cerebral and basilar artery territories—along with meningeal enhancement, non-specific white matter lesions and mild generalised atrophy (figures 2 and 3).39 40 MRI is preferable to CT scanning, given its superior parenchymal resolution and better characterisation of potential posterior fossa or spinal cord involvement. CT, MRI or even formal catheter angiography may be indicated to demonstrate vessel narrowing or irregularity, particularly when suspecting alternative diagnoses such as non-infective cerebral vasculitides.39 41

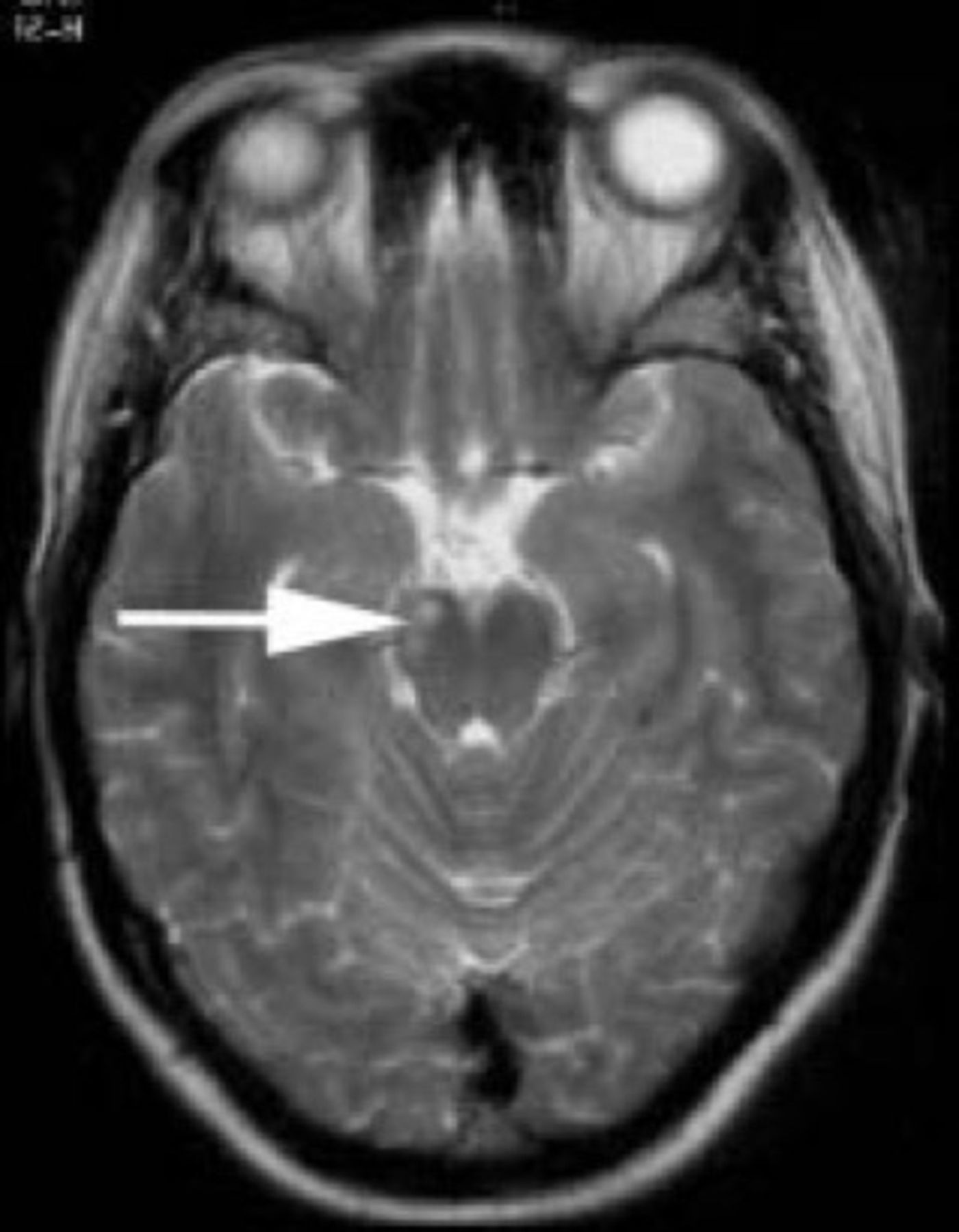
MR scan of brain showing T2 signal alteration in the right cerebral peduncle (arrowed) of a patient with meningovascular neurosyphilis.40
{kind=link}
{kind=link}
{kind=link}
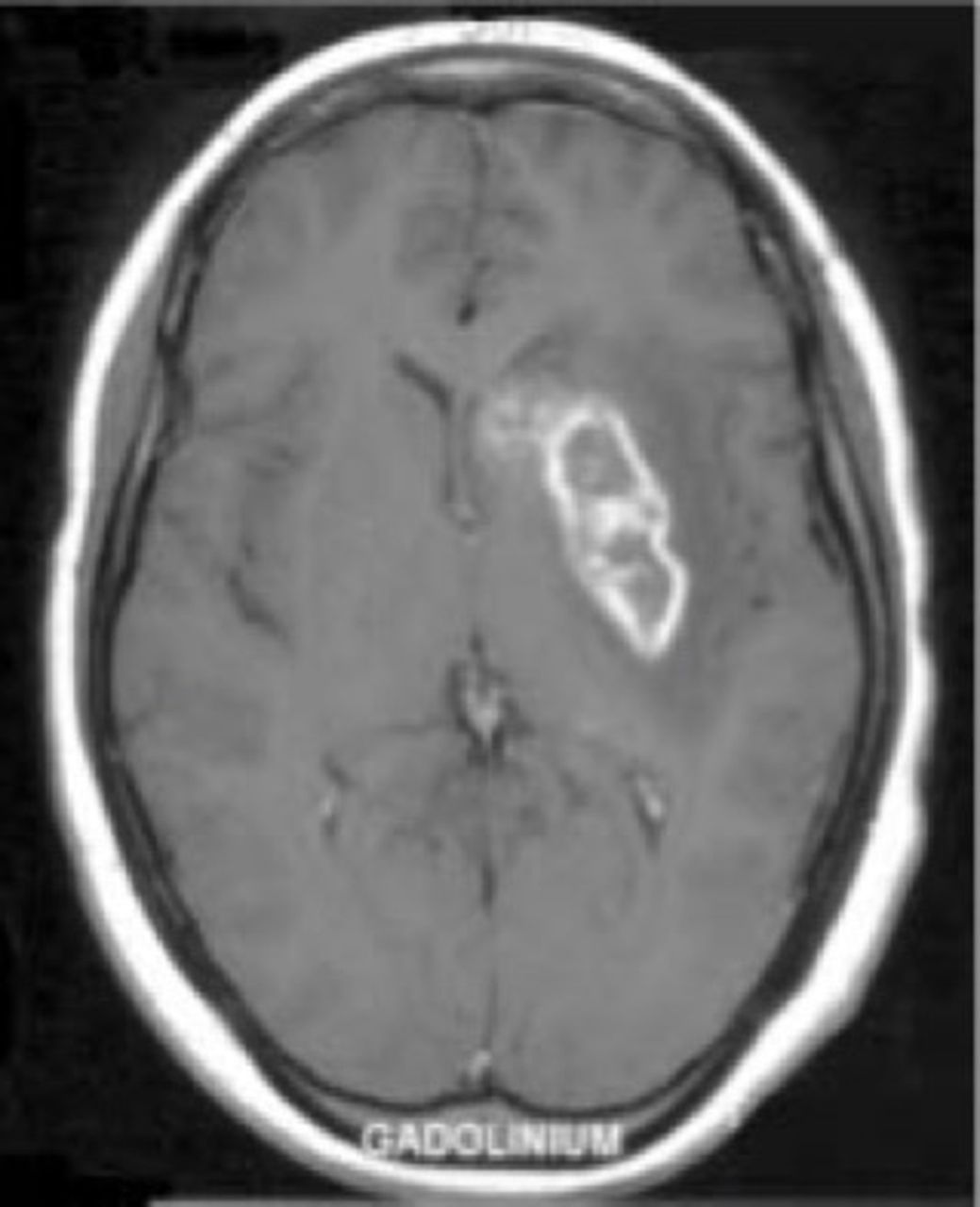
MR scan of brain (T1-weighted image with gadolinium) showing cerebral infarction in a 22-year-old HIV-positive patient with neurosyphilis.40
Differential diagnosis
Neurosyphilis should be a differential diagnosis for any HIV-positive patient presenting with unexplained neurological symptoms, as listed in box 3. Challenges arise due to the overlap of neurological manifestations caused by both organisms and the numerous pathologies that can develop in advanced HIV infection. Either organism can independently cause acute or chronic meningitis, vasculitis, cranial neuropathies, cognitive decline, myelopathy and peripheral neuropathy.42 All HIV-positive patients with neurological symptoms, including cognitive impairment, should undergo an appropriate diagnostic workup to exclude common viral infections (particularly herpes simplex, varicella zoster and enterovirus), cryptococcal meningitis, tuberculosis, toxoplasmosis, lymphoma, progressive multifocal leucoencephalopathy and to identify a detectable HIV viral load causing HIV encephalitis.13
Potential manifestations of neurosyphilis
(Aseptic) meningitis
Chronic headache
Psychiatric illness
Cognitive impairment
Ischaemic stroke
Seizures
Mass lesion
Cranial (poly)neuropathy
Optic neuritis/optic atrophy
Ataxia
Transverse myelitis
Myelopathy
(Poly)radiculopathy
Peripheral neuropathy
Treatment
Penicillins remain the treatment of choice for all stages of syphilis, with no reported cases of penicillin resistance. Guidelines currently recommend that, in the absence of central nervous system involvement, early (primary, secondary and early latent) syphilis should be treated with a single dose of benzathine penicillin G 2.4 million units (MU) intramuscularly, and late latent syphilis should be treated with three doses benzathine penicillin G 2.4 MU intramuscularly at 1-week intervals, regardless of HIV status (table 2).6 Although this is the first-line recommended regimen, a large review found that in HIV-positive patients, it is associated with serological failure (defined as a less than fourfold decline in RPR/VDRL titre) in 0%–33% of cases. ART reduces this risk by roughly 60%.17
Treatment regimen options for different stages of syphilis
In patients with an established diagnosis of neurosyphilis, treatment success depends on patients reaching sustained treponemicidal penicillin levels in the CSF. To ensure CSF penetration, neurosyphilis is treated with an intensified regimen of 1.8–2.4 MU procaine penicillin intramuscularly once daily for 10–14 days with oral probenecid 500 mg four times daily. Alternatively, inpatient treatment can be given with benzyl penicillin 10.8–14.4 g in total daily dose, given as 1.8–2.4 g intravenously every 4 hours for 10–14 days to those who are acutely unwell.6 In our centre, we treat all coinfected patients with procaine penicillin regardless of whether either a lumbar puncture has been performed or neurosyphilis diagnosis has been confirmed because of the concern of asymptomatic neurosyphilis. At this site, Warwick et al reported high serological treatment success rates at 98% at 6 months as well as good patient adherence despite the prolonged course of intramuscular treatment.43 A global shortage of probenecid however makes it unfeasible to treat patients presumptively for neurosyphilis without CSF analysis.
In patients with neurosyphilis who have a significant penicillin allergy, the best option is probably penicillin desensitisation.31 32 44 When penicillin-based regimens are not available, doxycycline 200 mg twice per day for 28 days is recommended.6 Due to its tolerability and resistance concerns, erythromycin and azithromycin are no longer recommended, particularly in men who have sex with men, where syphilis is highly prevalent.45 A small observational study reported that ceftriaxone 1–2 g per day intramuscularly for 10 days is an effective alternative to penicillin; however, evidence is limited.46 High-dose oral amoxicillin plus oral probenecid also proved to be highly effective in a retrospective observational study of patients with early and late syphilis and HIV infection.47
Corticosteroids and the Jarisch-Herxheimer reaction
The Jarisch-Herxheimer reaction is an acute feverish illness with associated headaches, myalgia and rigors that patients commonly experience several hours after starting treatment. It is a proinflammatory response caused by the destruction of large volumes of treponemes and occurs particularly among those with high VDRL/RPR titres. Guidelines recommend that patients with neurosyphilis be prescribed 3 days of oral prednisolone 40 mg—24 hours before and 48 hours after starting syphilis treatment.48 Although there are only limited data, it appears that corticosteroids do not reduce the incidence of the reaction but may reduce its severity.6 Given that corticosteroids have little or no effect on symptomatic neurological sequelae and that they cause immunosuppression, it is safer not to prescribe them to immunosuppressed patients. The only caveat to this is in cases of ocular syphilis where a Jarisch-Herxheimer reaction can worsen symptoms, which may not be reversible, and therefore clinicians should consider prescribing corticosteroids. In cases of advanced immunosuppression, seek guidance from an HIV specialist when considering prescribing these.
Ocular syphilis
Syphilis can affect the eyes in many ways. Conceivably the most well remembered ocular manifestation is Argyll Robertson pupils, which accommodate but do not react to light and thus demonstrate light–near dissociation. This finding is highly specific for syphilis but can also occur in diabetic neuropathy or as part of a dorsal midbrain syndrome. Anterior or posterior uveitis is perhaps the most common, but papillary conjunctivitis, scleritis, neuroretinitis and retinal vasculitis also occur, usually in secondary and tertiary stages. Furthermore, syphilis is on the important list of differential diagnoses for presentations of progressive optic neuropathy, and thus should be excluded in patients whose optic neuritis is ‘atypical’. Ocular syphilis appears to be a type of neurosyphilis, although it is not always accompanied by syphilitic meningitis or abnormal CSF results. However, given that the recommended treatment is the same neuropenetrative regimen used for neurosyphilis,48 it may not be necessary to perform CSF analysis in every case.
Monitoring
Patients who have been treated for neurosyphilis should have their blood RPR/VDRL titres monitored 3 monthly with serological response defined as a fourfold decline in titre or reversion to a seronegative state.6 Patients with HIV may show a slower time to serological response of up to 12 months due to loss of immune function such that there is a low-level production of antibodies. Those with serological failure—a less than fourfold decline in titre, static titre or increase in titre—need a thorough history and examination to determine whether this could be due to treatment failure or reinfection. Such patients may need to repeat CSF analysis.49
Repeat lumbar puncture should also be performed if there is significant CSF pleocytosis (>10 cells/µL) or positive CSF-VDRL at initial CSF examination. CSF examination should be repeated at least 6 monthly until the cell count is normal but may be necessary more frequently depending on the clinical picture. Repeat CSF examination may also show a reduced CSF VDRL concentration as a result of treatment, but these changes occur slowly and persistent abnormalities do not necessarily suggest treatment failure. Patients with a pleocytosis persisting after 6 months, without alternative explanation, probably need retreatment.50
Future research
We require further research to determine to what extent previous or ongoing syphilis infection in people living with HIV contributes to neurocognitive decline and which patients with HIV and syphilis coinfection should be actively investigated for neurosyphilis. We need comparison of serological and clinical outcomes of patients with HIV and early syphilis treated with single-dose benzathine penicillin G compared with the neuropenetrative procaine penicillin regimen. We also need more research to validate improved diagnostic markers such as CXCL13.
Case 1
A 42-year-old HIV-positive man presents to a sexual health clinic with a primary chancre and evidence of T. pallidum on dark ground microscopy. His most recent CD4 count is 55 cells/µL, and he is not on ART. Neurological examination including funduscopy is normal.
This man should certainly be offered a lumbar puncture. He is at high risk of neurosyphilis as well as other opportunistic infections that can cause meningoencephalitis. If the lumbar puncture identifies a white cell count <10 cells/µL and a negative CSF VDRL, then you can be confident he does not have neurosyphilis. If he refuses a lumbar puncture, then start outpatient treatment with a neuropenetrative regimen such as procaine penicillin with probenecid for 14 days or doxycycline for 28 days. It is not advisable to give corticosteroids to someone with this level of immunosuppression.
Case 2
A 26-year-old HIV-positive man presents with a 24-hour history of fever, headache and neck stiffness. He is on ART, his most recent CD4 was 550 cells/µL and he reports having attended a sex party 4 weeks ago. Syphilis serology identifies positive EIA and TPHA but negative VDRL. Lumbar puncture shows a white cell count of 12 cells/µL, predominantly lymphocytes, and CSF VDRL is negative.
The bloods suggest either primary syphilis or a previously treated infection. Correlating this with previous serology and a good history should help to establish which. If primary syphilis is likely, then this event signifies neuroinvasion of T. pallidum, which patients often clear spontaneously but given the symptoms and pleocytosis he should be treated with a neuropenetrative penicillin regimen. If this is not a case of primary syphilis, then other causes of his symptoms and pleocytosis, such as viral meningitis, should be sought.
Case 3
A 60-year-old HIV-positive man with a CD4 count of 623 cells/µL and on effective ART presents to a specialist HIV and neurology clinic with a history of cognitive decline. His bloods show a positive EIA and TPHA but negative VDRL. He does not recall receiving treatment for syphilis in the past. His MR scan of brain shows generalised atrophy. Lumbar puncture identifies a white cell count of 8 cells/µL, and all other tests including CSF-VDRL are negative.
This man has certainly had syphilis in the past, and he may well have been treated without remembering. However, his bloods may indicate late-latent infection that may be the cause of his cognitive impairment. A negative CSF VDRL does not rule out this diagnosis, and he should be treated for neurosyphilis while continuing other investigations for his cognitive decline.
Key points
When HIV-positive individuals develop neurological symptoms, always consider syphilis in the differential diagnosis.
When people who are not known to be HIV positive develop neurosyphilis, always perform an HIV test.
HIV-positive individuals with serological evidence of syphilis require a detailed history and examination for neurological signs.
Consider lumbar puncture for all patients with HIV and syphilis coinfection who have neurological signs, or if the CD4 count is <350 cells/µL, serum reactive plasma reagin/venereal disease research laboratory (VDRL) titre is ≥1:32, or they are not on antiretroviral therapy.
If cerebrospinal fluid (CSF) VDRL is negative, still consider neurosyphilis in patients with neurological signs and/or a CSF white cell count is >10 cells/µL in treated HIV infection, or >20 cells/µL in untreated infection
Acknowledgments
Many thanks to the library staff at Brighton and Sussex University Hospitals NHS Trust for their assistance with sourcing papers.
References
Footnotes
Contributors EH and DL conducted the literature search and appraised the evidence. EH and DL prepared the manuscript. MM, AWB, BHR and JHV reviewed the manuscript and provided specialist input.
Funding None declared.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Provenance and peer review. Commissioned. Externally peer reviewed. This paper was reviewed by Nicholas Davies, London, UK.
Other content recommended for you
- Syphilis
- Syphilis
- Diagnostic performance of PCR assays for the diagnosis of neurosyphilis: a systematic review
- Ocular syphilis among HIV-infected patients: a systematic analysis of the literature
- Treatment of syphilis in HIV-infected subjects: a systematic review of the literature
- Serological response to syphilis treatment in HIV-positive and HIV-negative patients attending sexually transmitted diseases clinics
- Syphilis in adults
- Clinical efficacy and tolerability of 1.5 g/day oral amoxicillin therapy without probenecid for the treatment of syphilis
- Re-evaluation of serological criteria for early syphilis treatment efficacy: progression to neurosyphilis despite therapy
- Neurosyphilis in a suspected case of giant cell arteritis