Article Text

Abstract
Medication-overuse headache is defined as headache occurring on more than 15days in a month in people with pre-existing primary headache, and developing as a consequence of regular overuse of acute headache treatments. Medication-overuse headache is common in general neurology clinics and can be difficult to manage. Most patients have a background of migraine, which has slowly transformed over months and years from the episodic to chronic form; with this comes an increased use of acute migraine treatment. This paper identifies who is at risk of developing medication-overuse headache, and reviews preventive measures and current treatment strategies.
- medication-overuse headache
- daily headache
- rebound headache
- migraine
- chronic migraine
Statistics from Altmetric.com
Introduction
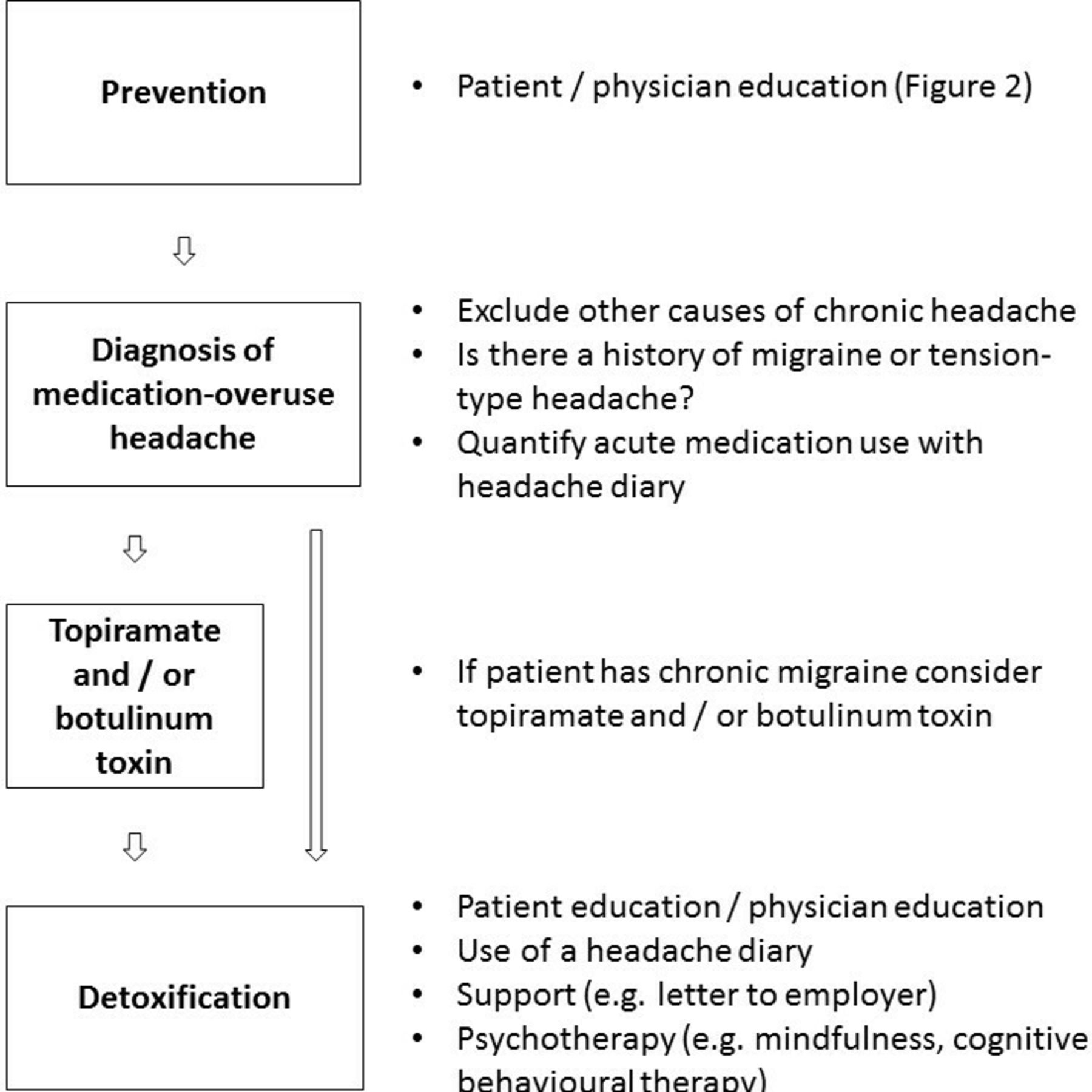
The observation that the analgesics used to treat headache can themselves cause headache1 is a paradox that over the years has led to significant confusion and frustration among both doctors and patients. Furthermore, so-called medication-overuse headache does not occur in everyone who overuses medication, and may occur in people taking analgesics for other conditions associated with chronic pain.2 The latest International Classification of Headache Disorders (ICHD-3),3 an expert consensus view, defines medication-overuse headache (also known as drug-induced headache, medication-misuse headache and rebound headache) as: ‘headache occurring on 15 or more days/month in a patient with a pre-existing primary headache and developing as a consequence of regular overuse of acute or symptomatic headache medication (on 10 or more or 15 or more days/month, depending on the medication) for more than 3 months’ (b ox 1). Medication-overuse headache is therefore considered a secondary headache disorder. It most frequently occurs in the context of chronic migraine and less with commonly chronic tension-type headache. It is a major global health problem with significant morbidity. This paper identifies who is at risk of developing medication-overuse headache, and reviews preventive measures and current treatment strategies (figure 1).
ICHD-31 diagnostic criteria for medication-overuse headache (8.2)
Headache occurring on ≥15 days/month in a patient with a pre-existing headache disorder.
Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache.*
Not better accounted for by another International Classification of Headache Disorders (ICHD-3) diagnosis.
*Regular intake of one or more of paracetamol, aspirin and non-steroidal anti-inflammatory drugs on ≥15 days/month AND/OR ergotamine, triptans and opioids on ≥10 days/month.

Management of medication-overuse headache (MOH).
How common is medication-overuse headache?
Epidemiological studies indicate that up to 4% of the population overuse analgesics and 1% have medication-overuse headache.4 One study estimated that up to 70% of people with chronic daily headache have medication-overuse headache.5
Who gets medication-overuse headache?
By definition, medication-overuse headache occurs in people with primary headache who overuse acute medication. Most have a background of migraine or less commonly of tension-type headache. Rarely, it develops in people with cluster headache, although typically there is also a background of migraine or a family history of migraine.6 Although any analgesic can cause medication-overuse headache, triptans and opioids appear to carry the most risk, and do so in a shorter period.7 Opioid dependence is common among migraineurs and can be difficult to treat. Medication-overuse headache is three to four times more common in women than men and its peak incidence is in the fourth decade.8 Those with psychiatric comorbidities, including anxiety and depression, appear most susceptible.9 Other risk factors include: age below 50 years; low education level; chronic musculoskeletal or gastrointestinal complaints; smoking; physical inactivity; high caffeine intake; and tranquilliser use.10
Pathophysiology
The pathophysiology of medication-overuse headache remains poorly understood, but probably reflects the complex interplay between brain networks involved in chronification of pain and exposure to certain psychosocial and socioeconomic stressors in genetically predisposed people. Medication-overuse headache seems to result from increased neuronal hyperexcitability in the cerebral cortex and in the trigeminal nervous system.11 Hyperexcitability of cortical neurones is associated with the development of the cortical spreading depression that accompanies migraine aura. Hyperexcitability of the trigeminal nervous system facilitates peripheral and central sensitisation, and so is important in chronic pain development.
Medication-overuse headache should perhaps be reclassified as a disorder occurring only in people with chronic migraine.12 It can develop in people with cluster headache without migraine—although with a family history of migraine—suggesting that certain genes involved in migraine increase the risk of medication-overuse headache, rather than the migraine itself.6 Polymorphic variants of the dopaminergic gene system and of other genes related to drug-dependence pathways appear the most closely associated with medication-overuse headache.13 All of these molecules are involved in pain modulation. Prolonged exposure to analgesics can alter neurotransmitter metabolism in pain pathways. Imaging studies in people with medication-overuse headache provide evidence of structural and functional brain alterations.14
Diagnosis
Medication-overuse headache has no distinct features and there are no specific laboratory tests that support the diagnosis. According to ICHD-3,3 the diagnosis can be made in patients with pre-existing headache disorders who regularly use acute or symptomatic treatments on more than 10–15 days/month, and have done so for more than 3 months (b ox 1). For ergotamines, triptans and opioids, this is >10 days/month; for other simple analgesics, including paracetamol, aspirin and non-steroidal inflammatory drugs, it is >15 days/month.
In clinical practice, medication-overuse headache most often develops in people with migraine (or less commonly tension-type headache) who report increased frequency or worsening of pre-existing headache or the development of new headache associated with medication overuse. Medication-overuse headache may be indistinguishable from the pre-existing headache. This can sometimes be difficult to untangle because the transition from episodic to chronic migraine or tension-type headache often induces more regular use of analgesics. A diagnosis of medication-overuse headache is therefore often retrospective, following drug withdrawal.
Before making a diagnosis of medication-overuse headache, it is important to consider other secondary causes of chronic daily headache. For example: Are there high-pressure symptoms or signs to suggest raised intracranial hypertension? Has the patient started a new medication? Do they have a history of weight loss or systemic symptoms to suggest vasculitis or malignancy? Have they developed hypertension? Is there obstructive sleep apnoea? Has there been a change in libido or menstruation, or other symptoms to suggest pituitary disease? Is there a history of depression or chronic fatigue? Patients need a careful physical examination to exclude hypertension, and focal neurological deficits (including visual field deficits), and papilloedema. Some may also need further investigation,15 including brain imaging.16
Be aware of those rare patients who can recall the day and sometimes the time of onset of a new continuous daily headache that has lasted more than 3 months: they have ‘new daily persistent headache’ rather than medication-overuse headache.17
Prevention
Education remains the single most important way to prevent medication-overuse headache. It is important to advise people with frequent episodic migraine or tension-type headache from an early stage to avoid medication overuse, especially of readily available over-the-counter simple analgesics. It is often useful for patients to keep a headache diary to record frequency of analgesic use or ‘painkiller days’. Clinicians should prescribe opiates and triptans only at doses that are likely to avoid development of medication-overuse headache. Sometimes it is difficult to achieve this, especially if there are comorbidities that require regular analgesia. Often patients acknowledge medication overuse but remain stuck in a cycle of drug dependence in order to function. Clinicians should consider using the general practitioner/patient letter to document how best to avoid developing medication-overuse headache.
Treatment strategies
Treating medication-overuse headache is therefore difficult and needs to be individualised. In practice, there are two approaches: either to reduce analgesic medication without additional treatment, or to do so following treatment with certain migraine preventatives.
Advice to patients
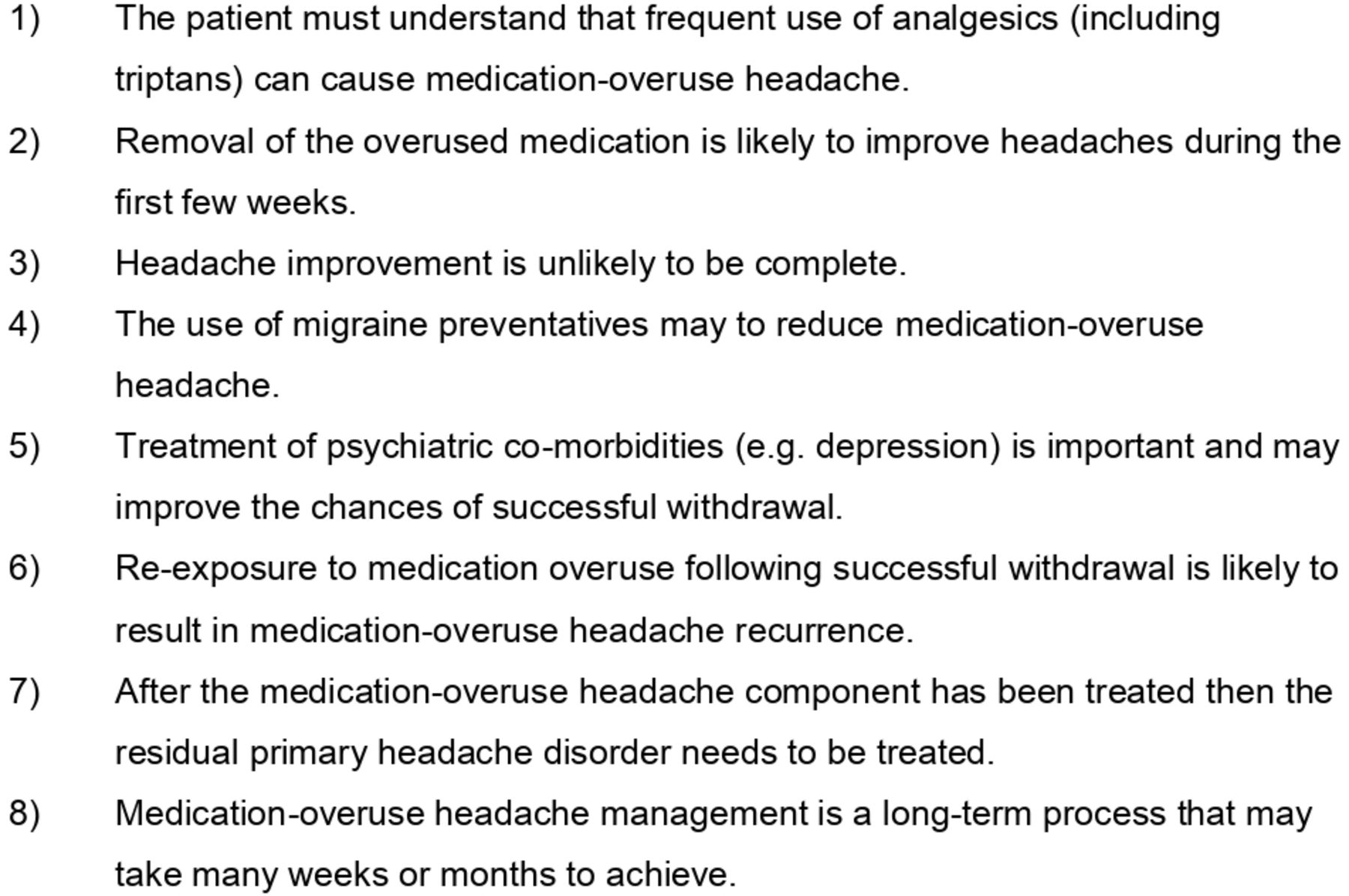
Before a trial of drug withdrawal or of adding a migraine preventative is it important to prepare the patient for what lies ahead and to manage expectations. Eight factors should be considered when treating patients with medication-overuse headache18 (figure 2).
{kind=link}
{kind=link}
Advice to patients before embarking on drug withdrawal18
Drug withdrawal
Patients are asked to withdraw their analgesics to an acceptable level. In the case of simple analgesics this should be headache on fewer than 15 days in a given month and for opioid/triptans it should be headache on fewer than 10 days. The speed of drug withdrawal depends on the class of drug being overused.19
For triptans and simple analgesics, abrupt withdrawal is preferable. Withdrawal headaches are to be expected and usually last for 2–10 days. Other commonly encountered symptoms include nausea, vomiting, sleep disturbance and anxiety. Patients overusing triptans typically improve over 7–10 days, while those overusing simple analgesics improve over 2–3 weeks.20 Several studies have shown that patients with simple analgesic and/or triptan-induced medication-overuse headache can significantly reduce their analgesic use following appropriate advice, and that this strongly associates with fewer headache days.21 A study by the Danish Headache Centre found that a 2-month outpatient detoxification programme without any acute migraine medication for breakthrough pain was more effective than permitting limited use of acute migraine medication (maximum 2 days/week).22 Simple analgesic and triptan overuse can therefore often be managed as outpatient.
Opioid medication overuse, however, is more troublesome and may need inpatient supervision. Withdrawal should be more gradual and take longer. People with substantial opiate overuse may benefit from inpatient detoxification, together with intravenous lidocaine infusions.23 However, this approach is often limited by access to hospital beds and availability of a headache or pain specialist to oversee inpatient treatment. The psychological and physiological dependence associated with opioid overuse adds to the difficulty of this approach. Importantly, people with opioid overuse must not feel that the treating team regard them as ‘addicts’, but rather as individuals who depend on opioids to lessen their headaches. Mindfulness and cognitive–behavioural therapy may also help.24
According to a recent systemic review and meta-analysis of different treatments, there are no high-quality data to support using corticosteroids or non-steroidal anti-inflammatory drugs during the withdrawal period in medication-overuse headache.25
Migraine prevention
Adding migraine preventatives can help the management of medication-overuse headache; once established they may facilitate subsequent attempts to withdraw acute headache medications. Trial data indicate that topiramate26 and botulinum toxin are useful.27 Topiramate should be started at a dose of 25 mg daily for a week, and increased by 25 mg daily every 2 weeks aiming for a maintenance dose of 50 mg twice daily. Some people benefit from as little as 50 mg daily, while others may need up to 400 mg daily. Topiramate is often poorly tolerated compared with other preventatives. Common side effects include: numbness and tingling in hands and feet; drowsiness; problems with speech, memory, concentration and coordination; and loss of appetite and weight loss. Less common but more serious side effects include: kidney stones; acute-onset angle-closure glaucoma; and significantly low mood. Topiramate should be avoided in pregnancy and at doses above 200 mg/day can reduce the efficacy of the combined contraceptive pill/oral contraceptives. Botulinum toxin significantly helps people with chronic migraine27 with and without medication-overuse headache28 and is frequently used in headache centres. Although the original trial data showed only a modest reduction in headache days per month compared with placebo (–8.2 vs –6.2), the benefits in the clinical setting appear much greater and cumulative. The exact mechanism of action of botulinum toxin in migraine remains unknown but it probably reduces peripheral and central sensitisation, both of which are involved in the chronification of pain.
Although drug withdrawal is the most effective treatment, most people find this difficult and report significant deterioration in their headaches, anxiety and, when withdrawing opioids, autonomic disturbance. These symptoms may last for up to a week but longer if they have overused opioids.20 Drug withdrawal requires planning: some people’s lifestyles and nature of employment do not allow this. In practice, patients should warn family members and employers of likely short-term deterioration and clinicians should consider writing a cover letter to employers.
Conclusions
The pathogenesis of medication-overuse headache is poorly understood but appears closely related to that of chronic migraine. Many people increase their analgesic use over time without necessarily realising there is a problem; they often remain unaware of the long-term consequences until advised that they have medication-overuse headache. Therefore, education is important in preventing its development. The diagnosis is sometimes difficult and headache diaries may play an important role. Although some people can successfully wean medications themselves, this often requires support; clinicians should advise patients that they will probably get worse before they get better. Detoxification without access to any acute medication treatments is probably the most effective strategy. People taking simple analgesics and/or triptans can often achieve this as an outpatient. It is more difficult for those overusing opioid medications and if their use is substantial they may require detoxification as an inpatient. Topiramate and botulinum toxin may help in managing medication-overuse headache, but the final goal should always be to reduce the frequency of acute headache medication use.
Key points
Medication-overuse headache is very common in patients with chronic migraine.
Medication-overuse headache may occur in patients who take triptans or opiods on >10 days / month or simple analgesics on > 15 days / month for more than 3 months.
Prevention through doctor and patient education remains the most important treatment strategy.
Detoxification may take up to 8 weeks and is best achieved with complete withdrawal of acute migraine medications.
Migraine preventatives, including topiramate and botulinum toxin have been shown to be beneficial in some patients.
References
Footnotes
Contributors BRW is the sole author of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed by Richard Stark, Melbourne, Australia.
Other content recommended for you
- Management of medication overuse headache
- Management of medication overuse headache
- Headache management: pharmacological approaches
- Assessing and managing medication overuse headache in Australian clinical practice
- Headache
- Chronic migraine
- The international classification of headache disorders, 2nd edn (ICDH-II)
- The Severity of Dependence Scale detects people with medication overuse: the Akershus study of chronic headache
- Management of children and young people with headache
- Management of chronic migraine