Article Text

Abstract
Aims: To compare prevalence, reasons, motivations, initiation, perceived helpfulness, and communication of complementary and alternative medicine (CAM) use between two tertiary children’s hospitals.
Methodology: A study, using a face-to-face questionnaire, of 500 children attending the University Hospital of Wales, Cardiff, UK was compared to an identical study of 503 children attending the Royal Children’s Hospital, Melbourne, Australia.
Results: One year CAM use in Cardiff was lower than Melbourne (41% v 51%; OR = 0.67, 95% CI 0.52–0.85), reflected in non-medicinal use (OR = 0.41, 95% CI 0.29–0.58) and general paediatric outpatients (OR = 0.38, 95% CI 0.21–0.67). Compared to Melbourne, factors associated with lower CAM use in Cardiff included families born locally (father: OR = 0.58, 95% CI 0.44–0.77) or non-tertiary educated parents (mother: OR = 0.54, 95% CI 0.38–0.77). Cardiff participants used less vitamin C (OR = 0.31, 95% CI 0.18–0.51) and herbs (OR = 0.49, 95% CI 0.34–0.71), attended less chiropractors (OR = 0.25, 95% CI 0.06–0.37) and naturopaths (OR = 0.08, 95% CI 0.02–0.33), but saw more reflexologists (OR = 3.33, 95% CI 1.08–10.29). In Cardiff, CAM was more popular for relaxation (OR = 1.92, 95% CI 1.03–3.57) but less for colds/coughs (OR = 0.4, 95% CI 0.27–0.73). Most CAM was self-initiated (by parent) in Cardiff and Melbourne (74% v 70%), but Cardiff CAM users perceived it less helpful (OR = 0.46, 95% CI 0.31–0.68). Non-disclosure of CAM use was high in Cardiff and Melbourne (66% v 63%); likewise few doctors/nurses documented recent medicinal CAM use in inpatient notes (0/21 v 2/22).
Conclusions: The differences in CAM use may reflect variation in sociocultural factors influencing reasons, motivations, attitudes, and availability. The regional variation in use and poor communication highlights the importance of local policy development.
- complementary and alternative medicine
- comparison
- reasons
- motivations
Statistics from Altmetric.com
The reasons and motivations for the use of complementary and alternative medicine (CAM) by children and families, lack extensive study.1–3 CAM prevalence and cost is escalating; a 1993 survey revealed that 48.5% of Australians used CAM, with the follow up study in 2000 indicating that Australians spent A$2.3 billion on alternative therapies, a 62% increase since 1993.4,5 A systematic review in 1999 found that 9–70% of children used CAM.6 Paediatric primary care studies report CAM usage of 21–33%;7,8 usage is 12–53% in hospital based studies.9–12 Comparing the differences in CAM use between two populations allows exploration of the sociocultural reasons and motivations for use. Determining CAM use in paediatric populations has been hampered by differences in definitions, methodology, populations, and estimates of prevalence.6,8,9,11–13 There has been no direct comparison of two paediatric populations using the same methodology. Thus the primary aim of this paper was to compare two large, hospital based population studies, to identify differences in use and explore reasons and motivation for use. Secondary aims were to compare disclosure, potential interactions, and local indicators of use to assist in establishing policies.
METHODS
A study completed in Melbourne from October 2001 to February 2002 at the Royal Children’s Hospital (RCH) in Victoria, Australia comprises the comparison population.10 The Cardiff study was undertaken at the University Hospital of Wales (UHW) from January to February 2004 in the UK. These are both tertiary centres, UHW being the tertiary paediatric hospital in Cardiff and South-West Wales, UK, and RCH is the main tertiary referral hospital for metropolitan Melbourne and Victoria, Australia. In 2001, the population of Wales was 2.9 million (<16 years = 0.59 million); that of Victoria was 4.6 million (<15 years = 0.94 million).14,15 Each centre had almost identical numbers for the five groups studied—any inpatients, and outpatients from endocrinology, general paediatrics, respiratory medicine, and gastroenterology. Consecutive presentations of any neonate, child, or adolescent of any age to the above hospital areas were sampled to provide a broad cross-section. Identical exclusion criteria included insufficient knowledge of the English language or children admitted to intensive care.
The questionnaire was designed and piloted by the Melbourne group after a literature review failed to locate a validated questionnaire that would appropriately answer our research questions. Data were collected in a short (5–10 minute), face-to-face interview with the patient or parents/carers. The two page, 20 question survey obtained demographic data and prescription medicine use from all participants. If the child had used CAM in the past year, further questions assessed CAM type, reasons and motivations for use, initiation of therapy, perceived helpfulness, cost, and communication with doctors. Medicinal CAM was defined as naturopathic, herbal, homeopathic, or traditional Chinese medicine, health products, dietary and food supplements, or vitamins and minerals. Non-medicinal CAM was chiropractic, naturopathy, traditional Chinese therapy, acupuncture, osteopathy, aromatherapy, iridology, therapeutic massage, reflexology, Buteyko breathing, kinesiology, reiki, hypnosis, special exercises, or modified diet. Any other forms of CAM not listed above were sought and included if disclosed. The use of non-prescribed vitamins/minerals was included as they have been documented to cause adverse events or interactions, and were taken with therapeutic intent.16 Inter-interviewer agreement within each study was performed. Calibration between the two research groups occurred prior to the Welsh study to ensure comparable techniques.17 UHW had four interviewers and RCH three; none were involved in the medical treatment of the patients.
The South-East Wales Local Research and Ethics Committee and the Royal Children’s Hospital Ethics in Human Research Committee approved each study. In Melbourne the data were entered into a Microsoft Access database and Stata version 7.0. The Cardiff group used an Excel database and performed comparative analysis using SPSS version 11.0. Comparison used Pearson χ2 testing; p values <0.05 were considered statistically significant. The Melbourne study determined the sample size by estimating that for prevalence ranges of 10–60% (based on literature review), sample size estimates with 95% confidence would be 138–369. Hence 500 were chosen to provide an adequate sample size, with a convenient 100 for each group selected.10
RESULTS
Melbourne studied 503 children (from 750 eligible), including 101 inpatients, 102 respiratory patients, and 100 each from general paediatrics, diabetes, and gastroenterology outpatients.10 Cardiff studied 500 children (from 581 eligible), 100 from each group (mixed endocrinology rather than diabetics only).
Prevalence
CAM use was less prevalent in Cardiff than Melbourne (table 1).
Sociodemographics of total study populations and CAM users, Cardiff versus Melbourne
Table 2 highlights demographic differences between the total samples from Cardiff and Melbourne. The age range in Cardiff was 0–19 years, the same as Melbourne.
Table 2 also highlights differences between CAM users in Cardiff and Melbourne. The most important finding is that compared to Melbourne, locally born Cardiff parents and non-tertiary educated Cardiff parents were less likely to have CAM using children compared to their Melbourne counterparts.
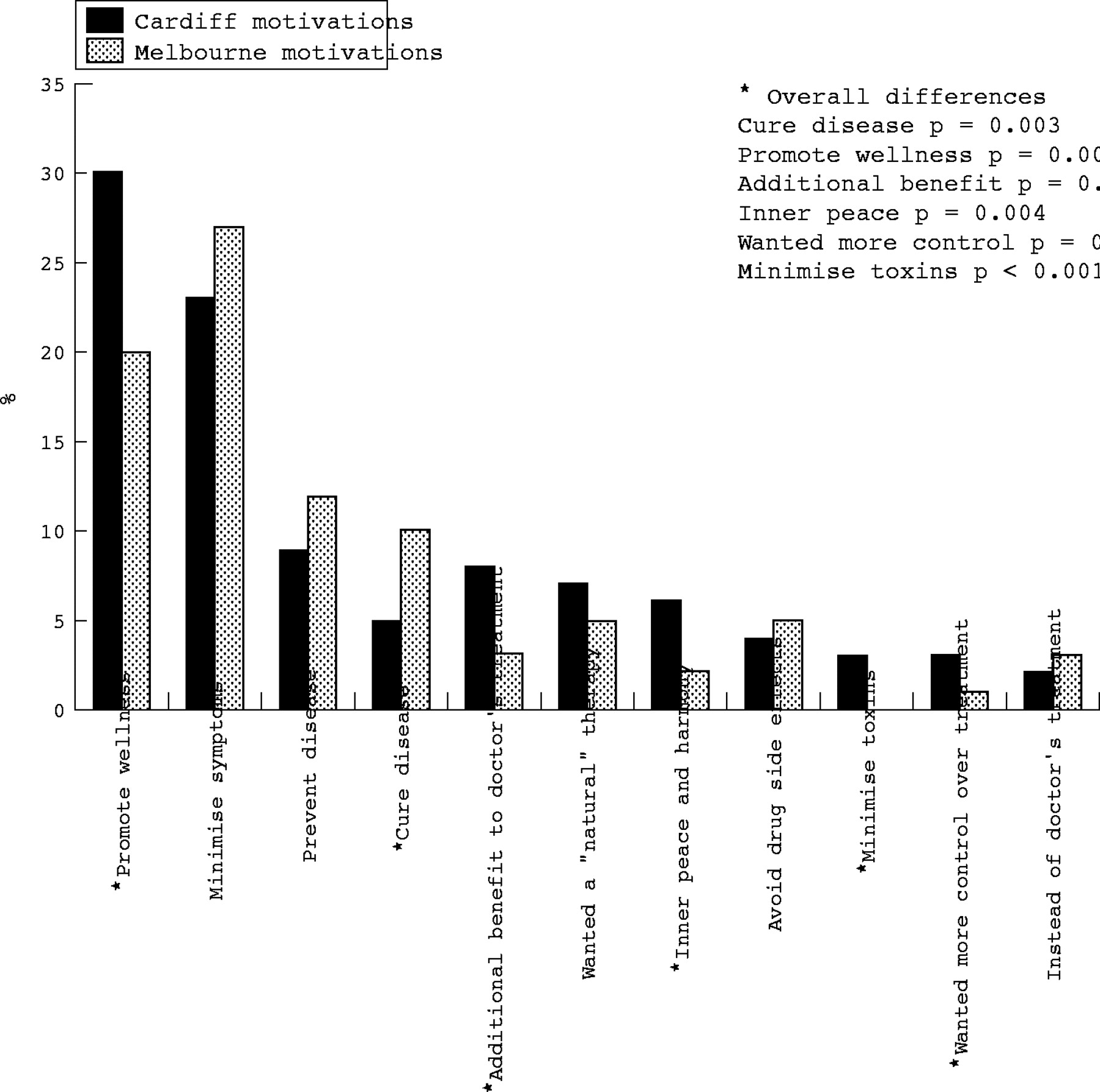
Figure 1 compares reasons and figure 2 motivations for CAM use in Cardiff and Melbourne, highlighting differences. In both studies the majority of CAM therapies were self-initiated (parent/patient or family/friends): Cardiff 74% versus Melbourne 70%. However, Cardiff CAM users perceived it as less helpful (57% v 74%; OR = 0.46, 95% CI 0.31–0.68).
In the last month, similar numbers of total participants were combining medicinal CAM and prescription medications in Cardiff (18%) and Melbourne (17%), and combining herbs and prescription medicines in Cardiff (3%) and Melbourne (4%).
Lack of disclosure to medical practitioners was prominent in both studies: 66% Cardiff versus 63% Melbourne. Less Cardiff medicinal CAM users thought the “doctor needed to know” about the CAM use than in Melbourne (45% v 83%; p < 0.001). Both studies showed poor documentation of medicinal CAM use in the past month in the inpatient notes by doctors/nurses (0/21 in Cardiff v 2/22 in Melbourne).
High CAM use was defined as a participant using four or more CAM in the past year (Cardiff, n = 14; Melbourne, n = 46). In Cardiff, high CAM use was associated with a tertiary educated mother (5% v 1%; p = 0.02) and all parents and children were born in the UK. Use of homeopathy (33% v 2%; p < 0.001), herbs (20% v 1%; p < 0.001), and aromatherapy (33% v 1%, p < 0.001) were more likely in high CAM users. In Melbourne, high CAM use was associated with age >2 years (p = 0.03), being an only child (p = 0.04), and female sex (p = 0.03).
DISCUSSION
No previous direct comparison between two paediatric populations with the same methodology has been reported. Both Cardiff and Melbourne found a high prevalence of CAM use compared with previous studies.2,8,11,13 We found lower prevalence and less regular CAM use in Cardiff relative to Melbourne. This difference was mainly accounted for by less use of specific medicinal (vitamins/minerals, herbs, naturopathy) and non-medicinal CAM (chiropractic, naturopathy, and therapeutic massage) in Cardiff, exemplified by the general paediatric group. We speculate that some of the differences may be explained by sociocultural variation, prevailing attitudes, and lower availability in Cardiff.
Sociocultural themes
CAM as a social phenomenon is increasingly reported in the literature. Astin proposed a philosophical congruence theory, where “treatment promotes health rather than just focusing on illness”.18 His findings supported three types of CAM users: a holistic health view (body–mind–spirit); those having transformational experiences who then see the world differently; and “cultural creatives”—individuals with a commitment to environmentalism, spirituality, and “love of the foreign and exotic”.19 Saks referred to this “search for greater control over the self”20 and Furnham expanded on the CAM “type” and adds that people “shop for health” and “want an emphasis on wellness not illness”.21 Coulter and Willis speculated the growth of CAM relates to a “post-modern” thesis: as social change and globalisation accelerates, faith in medical science’s ability to solve the problems of the living has declined. Concurrently “individualism” is growing—those seeking greater levels of control and empowerment in their lives, utilising tools such as the internet. Increased migration in the past 20 years is implicated in transmission of established medicines from other lands (for example, traditional Chinese medicine).22

Motivations (including differences) for CAM use overall, Cardiff and Melbourne.
Comparison of attitudes
The above principles may help explain the high prevalence in both centres. We speculate that these principles reflect the attitudes of Melbournians to a greater extent than Cardiff residents. The Cardiff locally born group were less likely to use CAM than the Melbourne locally born group. Comparison of demographics and census data shows less overseas born residents in Cardiff than Melbourne (3.2% in Wales v 23.4% in Victoria).14,15 Thus the more “culturally varied” population of Melbourne may have influenced the attitudes of those locally born, producing more “cultural creatives” who are more likely to use CAM.
Tertiary education was associated with CAM use in Cardiff, similar to other studies supporting education as a predictor of CAM use.2,18 Melbourne did not show this trend, mainly due to children of lower educated parents in Melbourne using more CAM than expected. We speculate that education as a factor was diluted by differing attitudes and availability in Melbourne. The higher prevalence among older children in Melbourne reflects previous findings2,8 and may represent greater “individualism”.
The finding that Cardiff participants perceived CAM less helpful than Melbournians is important as most CAM was self-initiated in both studies. This suggests that high CAM prevalence may be related to “word-of-mouth” promotion of its use by parents themselves. Other studies have found word-of-mouth2 and perceived efficacy18 to be important determinants in CAM use.
The higher motivation to cure disease in Melbourne may be explained by the higher use of vitamins, herbs, and naturopathy to prevent and treat coughs and colds. The more common holistic motivations in Cardiff represent small numbers and are less important than the overall trend, indicating similarity in motivations between centres.
Comparison of availability
Different profiles of available CAM practitioners between countries may reflect patterns of usage.23 Approximating the number of CAM practitioners per capita in Wales versus Victoria suggests lower availability in Cardiff. In 2004, chiropractor registrations were: Wales (n = 17), Victoria (n = 928) (0.6 v 20 per 100 000 population)14,15,24,25 (personal communication, Badenoch K. Chiropractors Registration Board of Victoria, 4 October 2004). The number of naturopaths registered in Wales (n = 10) was much lower than in Victoria (n = 300) (0.3 v 6.5 per 100 000.14,15,26,27 By contrast, results for reflexologists were much closer: Wales (n = 20), Victoria (n = 59) (0.7 v 1.3 per 100 000)11,12,28,29 (personal communication, Hall N. British Reflexology Association, 4 October 2004). The predominance of using non-medicinal CAM for “relaxation” in Cardiff may reflect the proportion of aromatherapists and reflexologists practising, just as the predominance of “musculoskeletal” indications in Melbourne may reflect the high proportion of chiropractors. The limitation of analysing this trend is that CAM practitioners are predominantly self-regulatory, so it is difficult to ascertain specific numbers of practitioners.
Private health insurance (PHI) was associated with CAM use in Melbourne, but not Cardiff. Melbourne participants had more PHI (48%), which is reflected in national statistics (45% Australians v 9% British).30,31 Thus PHI may be used to pay for CAM more, as reflected by some Australian policies which cover up to 13 types of CAM for up to $900/year,32 including chiropractic, massage, and naturopathy, three of the commonest non-medicinal CAM in the Melbourne study. By contrast, an example UK policy only covered four CAM up to £250.33 None of the top three non-medicinal CAMs in the Cardiff study (aromatherapy, reflexology, therapeutic massage) were covered.
Although these comparisons of availability apply more to parents than their children, it remains possible that consumer forces affect CAM acquisition by parents for their children.21
The government sponsorship of CAM is predominantly through primary care in both countries. In 2001, 49% of UK general practitioners were providing some form of CAM, with 58% being paid for by the NHS.34 In Australia, Medicare only provides rebates for acupuncture, which is extensively provided by general practitioners to adults.35
Communication and policy
Both studies found moderate rates of combining prescription medicines and CAM, risking adverse events36 (although herb–drug combinations were fortunately less common). This raises important issues of safety, especially in view of the poor communication shown by parents and doctors/nurses (worse in Cardiff) in the studies compared. These findings are not new, and support previous studies of poor CAM disclosure rates by parents/carers (63–79%),7–9,37 with paediatricians unlikely to raise the subject (only 6% asked in a US study).37 The same US study found poor communication despite 53% of parents wanting to discuss CAM.37
To address communication and safety, the Melbourne study provoked policy and guideline development,38 as the Cardiff study has done. A policy may promote dialogue in the inpatient and outpatient setting by giving patients and parents/carers “permission” to discuss CAM and staff a framework and safety nets to work within. Identifying and documenting CAM use, discussing potential interactions with pharmacists and parents, and notifying suspected adverse events from CAM can improve our care of children.
Determining factors associated with high CAM use can be incorporated into local policy. Our comparison shows this can differ markedly between regions. Hence it would be sensible to incorporate into a Cardiff policy screening questions relating to parental education, and use of aromatherapy, herbs, and homeopathy. In Melbourne, questioning females, families with one child, and children older than 2 years would be more relevant.
Limitations of the study
There were a number of limitations in our study. Sampling bias was minimised by interviewing consecutive inpatients and outpatients at both sites. The initial eligible populations differed but the final samples were the same size. The same definition of CAM and questionnaire were used, and attempts to calibrate interview techniques between sites were made, but variation between interviewers remains possible. The use of CAM and questions of reasons and motivations is subject to recall bias as it is a retrospective account over the past year. The studies were conducted two and a half years apart, so some differences may be time related. All interviews took place in busy wards and outpatients, which may limit disclosure in some instances, but this was the case at both sites. Exclusion criteria were identical, including non-English speaking candidates. This minimises some of the comparative differences, but highlights the need for further research in specific ethnic groups. The Melbourne group had no data on income, weakening the socioeconomic comparison. Population bias may have occurred with the different endocrine patient profiles.
What is already known on this topic
-
Communication between CAM users and medical practitioners is poor
-
The potential for interactions between CAM and prescription drugs raises important safety issues
Conclusions
Doctors need to be aware that CAM use is highly prevalent in children. Comparison of CAM use between these tertiary paediatric hospitals reveals lower use in Cardiff. These differences may be due to variation in sociocultural factors influencing reasons, motivations, attitudes, and availability of CAM. Regional variation, poor communication, and the risk of interactions highlights the importance of local policy development.
What this study adds
-
The reasons and motivations for CAM use have been explored, with an emphasis on sociocultural influences such as attitudes and availability
-
Local differences in CAM use and poor communication are highlighted, emphasising the importance of developing locally applicable policies on CAM to improve communication and safety
Prevalence of complementary and alternative medicine use, Cardiff versus Melbourne, over past year
Sociodemographic differences, Cardiff versus Melbourne: (A) total participants; (B) CAM users versus non-users
Types of CAM used: medicinal and non-medicinal, Cardiff versus Melbourne

{kind=link}
{kind=link}
Reasons (including differences) for CAM use overall, Cardiff and Melbourne.
Acknowledgments
We acknowledge the following: Dr Ajay Ready and Dean Whittle for interviewing participants; Dr Robert Newcombe, Department of Epidemiology and Public Health, Cardiff University for statistical assistance; Mrs Janine Cincotta for data entry and Ms Jenny Cope for database design and data entry.
REFERENCES
Footnotes
-
Published Online First 15 September 2005
-
Competing interests: none