
Abstract
A survey of 445 doctors in Yorkshire was conducted to ascertain their knowledge and awareness of alcohol units. Only 58% had some knowledge, and general practitioners scored better (69%) than hospital doctors (45%). However, 14% of doctors had no knowledge at all about alcohol units. Those who did not drink alcohol knew less than those who did and trainee doctors had significantly less knowledge than more senior physicians. Junior doctors who often deal with alcohol-related problems in their day-to-day hospital work had a poor knowledge. There needs to be a greater emphasis on alcohol and alcohol-related problems (including how to calculate alcohol units) in undergraduate and postgraduate curricula to improve doctors’ knowledge and awareness of this important subject.
Introduction
The UK government has placed great emphasis on drinking alcohol safely including producing guidance on the recommended maximum weekly alcohol consumption based on units. However it is not clear whether the general public or even medical practitioners are fully conversant with these limits. Even if sober, those who drink may find it difficult to know how much alcohol they are consuming as there may be a significant difference in the alcohol concentration of apparently similar drinks.1 The Department of Health's Alcohol Harm Reduction Strategy requires general practitioners (GPs) to implement management strategies for alcohol-related problems.2 However, patients with significant problems are more likely to attend hospital and less likely to visit their GP.3 The importance of a coordinated strategy to alcohol and alcohol-related problems has been emphasised by a report from the Royal College of Physicians (RCP).4 In a survey conducted among medical outpatients in a Yorkshire teaching hospital in 2004 only 14% had some knowledge of alcohol units.5 In 2005 a survey of GPs and hospital doctors in Leeds was undertaken to ascertain their knowledge of alcohol units using the same questions as the 2004 study.
Methods
Hospital doctors (mostly physicians) working at the Leeds General Infirmary were asked to complete a questionnaire at postgraduate meetings and teaching sessions. In addition all GPs in Leeds primary care trusts were sent an identical questionnaire by post (Table 1). The covering letter asked doctors for their help with a survey on alcohol units, reassured them that it was anonymous and thanked them for their participation. They were asked to record whether they were a GP or a hospital doctor (and grade), and whether they drank alcohol or not. This was followed by three further questions:
the safe limits of weekly alcohol consumption for both sexes and what these were (14 units for women, 21 units for men)
to determine the number of units in a 750 ml bottle of whiskey (40%) (correct answer 30 units)
to discern the highest and lowest alcohol consumption from four fictitious drinking patterns (Table 1). Using the formula that the percentage volume of alcohol is equal to the number of units in a litre of that alcoholic drink, the correct answers to the four fictitious drinking patterns are 28 units, 42 units, 36 units and 12 units respectively. The daily lager drinker therefore consumed the highest number of units and the sherry drinker the least.
The study questionnaire.
A correct answer for each question scored 1 point, unanswered questions were assigned a 0 score as it was presumed this was due to an inadequate level of knowledge. A total score could therefore range from 0 to 3.
Results
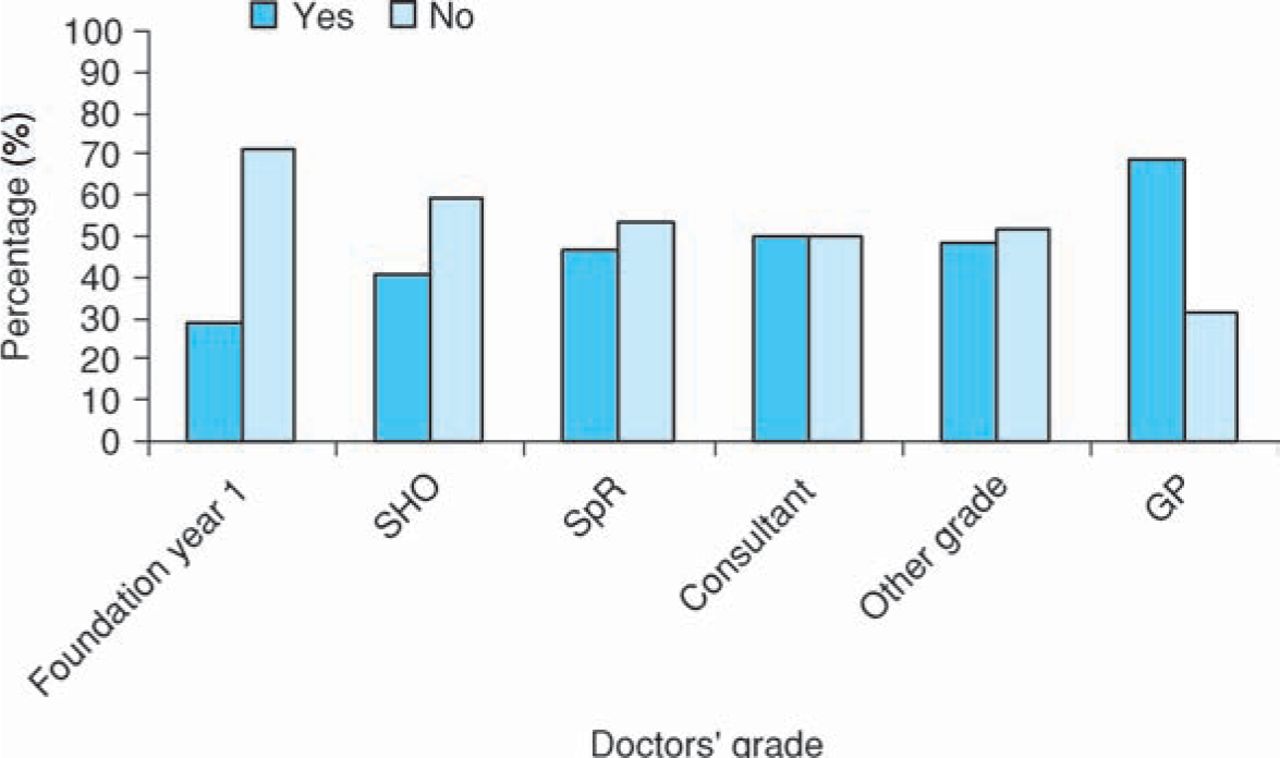
A total of 480 questionnaires were sent to GPs and 245 (51%) were returned. A further 320 questionnaires were distributed to hospital doctors and 200 were returned (62%). All responses were anonymous. The majority of doctors (79%, 351/445) claimed familiarity with alcohol units. Overall 58% (258/445) of doctors knew the safe alcohol limits for both sexes. GPs scored better (69%) than hospital doctors (45%), and for the latter group, knowledge improved with increasing seniority (Fig 1). Doctors listed as ‘other grade’ in the table were mostly experienced staff grade physicians or associate specialists.

Doctors’ knowledge of safe limits of weekly alcohol consumption according to grade. GP = general practitioner; SHO = senior house officer; SpR = specialist registrar.
Doctors responded to all three of the final questions and the majority had some knowledge − 154 (35%) scored 1 point while 151 (34%) scored 2 points. Interestingly, only 18% (78/445) were fully conversant with alcohol units and scored 3 points, but 14% of the doctors (62/445) had no knowledge about alcohol units and scored 0. Only 16 doctors felt that they were unfamiliar with alcohol units, but only 18% (78/429) scored the full 3 points. Teetotal doctors had significantly less knowledge about alcohol units than those who drank (p<0.003, Table 2).
A comparison of doctors’ knowledge: drinker versus non-drinker.
Discussion
‘Standard drinks’ was the term used until 1987 when ‘units’ were first introduced. The first UK government recommendation of a safe upper limit for drinking alcohol in a week was in 1992 and this was subsequently changed in 1995 to a daily recommendation, when the dangers of binge drinking were recognised.6,7 Further strategies have since been adopted to reduce alcohol-related harm with public education of ‘sensible drinking’ habits being a key strand to this policy and this has also been emphasised by the RCP.4 However, this is no simple task: a small glass of wine, for example, is 1 unit provided the strength is 10% alcohol by volume (ABV) and the glass is 100 ml. However, most wines are stronger than this and the capacity of a wine glass can be as large as 250 ml. Moreover the alcohol industry does not always state the content in units on the product. Accurately calculating alcohol units can be complex, but in essence the %ABV equals the number of units of alcohol in a litre of that liquid.
Common medical problems such as stroke, heart failure, hypertension, diabetes mellitus, osteoporosis, peptic ulcer disease, depression, confusion and falls may all be compounded by excessive alcohol consumption. Alcoholics are heavy users of health services for both physical and mental illness.8 Unfortunately healthcare professionals often have negative attitudes towards the issues of alcohol consumption. This stance may reflect lack of time, negative personal attitude or lack of understanding of severity of alcohol-related problems.4 In a survey of 36 doctors from a London teaching hospital, alcohol-dependent patients were viewed as violent and aggressive and doctors tried to avoid them by delegating care.9 Overall, these doctors had little confidence in treating this group, who in turn were more dissatisfied with their care than control groups of patients. An RCP working party identified lack of education and training of medical and nursing staff to be an important reason for the negative attitude towards patients with alcohol problems.4
Improving the public's perception of alcohol units remains a key target in alcohol-related harm reduction. The Office of National Statistics reported consistent improvement in the knowledge of the general population about units and safe drinking. In 2004 56% of beer-consuming adults knew that one unit is equivalent to half a pint of beer, and 66% of wine-consuming women knew that a small glass of wine represents one unit.10 In that survey 81% of respondents said that they were aware of measuring alcohol consumption in units.
The current survey showed that 79% of interviewed doctors drank alcohol, a prevalence similar to the general population in the UK. It is important for doctors to ascertain the actual amount of alcohol intake rather than accepting a patient's account. One might expect doctors to be fully conversant with alcohol units if they are to be in a position to educate patients. In this study, only 18% of doctors were fully conversant, although the majority laboured under the misconception of having a good knowledge. This is extremely important as doctors, regardless of whether they drink or not, must be in a position to counsel patients.
A previous UK survey revealed that only one in four practice nurses knew the sensible drinking limits for both men and women in primary care.11 There has been no similar study undertaken to ascertain doctors’ knowledge of alcohol units. This survey showed that junior doctors have a particularly poor knowledge about alcohol units. This may be because they do not have as much experience in dealing with alcohol-related problems, and the undergraduate teaching on this subject may be fairly brief. Currently, there is no requirement for medical schools to provide properly structured educational programmes on alcohol and the amount of teaching on this subject varies considerably.12,13 Similarly there is no provision of postgraduate training and certification for doctors and nurses wishing to develop a special interest in management of alcohol-related problems. This has implications both for national policy on alcohol-harm reduction and for doctors applying government guidelines in clinical practice.
Study limitations
This was an opportunistic study, of self-reported data, enabling a higher return of questionnaires with minimum cost.
Conclusions
This survey suggests many doctors have a poor knowledge of alcohol units and are not in a good position to counsel patients. It is possible that the guidelines are difficult to understand, and their implementation would be facilitated by better labelling of alcoholic drinks by manufacturers to include alcohol units. However, most important of all a better education strategy of the general population and medical practitioners is needed. The authors entirely endorse the recommendations of the RCP working party and would suggest that education on alcohol and alcohol units is incorporated into all medical undergraduate curricula and also teaching programmes for junior doctors (foundation trainees, specialist and emergency medical trainees and general practice vocational trainee registrars) to ensure doctors are better placed to counsel patients and deal with alcohol-related problems in the future as proposed by the Alcohol harm reduction strategy for England.2
Contributors and sources
AKD conducted the literature search, was the lead author and was guarantor of the paper. JAJS designed the questionnaire and instigated the patient survey. EK assisted in collecting and compiling the data. OJC suggested extending the survey to hospital doctors, facilitated this and helped draft the paper. RMW provided statistical support. The guarantor accepts the full responsibility for the work and/or the conduct of the survey, had access to the data, and controlled the decision to publish.
Ethical approval
Leeds East Research Ethics Committee did not wish to review the project.
Funding
The cost of the postal survey was borne by the lead author.
- © 2009 Royal College of Physicians








{kind=link}