
ABSTRACT
We evaluated factors and outcomes associated with elapsed time to surgery (ETTS) in 1,081 men and 2,891 women (mean age 83.5 years ±9.1) undergoing hip fracture surgery (from 2009–2019). Mortality rates were 4.8%, 6.3%, 6.2% and 10.3% (chi-squared 19.0; p<0.001), and hospital length of stay (LOS) >19 days were 31.9%, 32.8%, 33.8% and 43.2% (chi-squared 18.5; p<0.001) for ETTS <24 hours, 24–35 hours, 36–47 hours and ≥48 hours, respectively. There were no differences between ETTS categories for failure to mobilise within 1 day of surgery, pressure ulcers or discharge to nursing care. After adjustment for age, sex, American Society of Anesthesiologists' score and years of data collection, compared with Sunday, the risk of ETTS ≥36 hours was highest on Friday (odds ratio (OR) 3.50; 95% confidence interval (CI) 2.43–5.03) and Saturday (OR 4.70; 95% CI 3.26–6.76). Compared with ETTS <24 hours, there were increases in the risk of death when ETTS ≥48 hours (OR 2.31; 95% CI 1.47–3.65) and LOS >19 days (OR 1.34; 95% CI 1.02–1.75). The median (interquartile range (IQR)) LOS for ETTS <24 hours was 12.7 days (IQR 8.0–23.0), 24–35 hours was 13.5 days (IQR 8.4–22.9), 36–47 hours was 14.1 days (IQR 8.9–23.3) and ≥48 hours was 16.9 (IQR 10.8–27.0; p<0.001). The 10-year period of collection did not change the conclusion. Admissions towards the end of the week are associated with delayed ETTS for hip fractures, while delay in surgery, particularly beyond 48 hours, is associated with increased risk of mortality and prolonged LOS.
Introduction
The Best Practice Tariff for hip fractures was introduced in 2010 to financially incentivise individual hospitals by paying them a supplement for each patient over 60 years of age whose care satisfied six clinical standards. These included the elapsed (waiting) time to surgery (ETTS) within 36 hours from arrival in an emergency department.1 This criterion was supported from studies showing that beyond this 36-hour threshold, the risk of mortality and a prolonged length of stay (LOS) in hospital was increased.2–4 In addition, delays in hip surgery have also been associated with increased risk of complications, including myocardial infarction, deep vein thrombosis, pulmonary embolism and pneumonia.3 Furthermore, a shorter ETTS is associated with a greater opportunity to return to independent living.5 However, several studies have disputed these findings, reporting no association between ETTS and mortality.6–8 Other studies have variably reported ETTS thresholds in relation to outcome measures, ranging between 24 hours and 72 hours.9 The underlying reasons for delays in surgery are not certain but may be related to inter-study differences, such as patients' underlying health status while delays in echocardiography contribute to longer ETTS.10 In addition, the time of admission has been a focus of research in many studies, showing an association between delays in surgery with admission during weekend, evening or night time, and holiday periods.11–13
Therefore, the 36-hour threshold set by the Best Practice Tariff requires re-evaluation to strengthen its validity, while it is essential to identify preoperative factors that could influence the ETTS in order to minimise surgical delays. Herein, we examined both the preoperative factors and postoperative outcomes in relation to ETTS in the same group of patients undergoing surgery for hip fractures.
Methods
Study design, participants and setting
We conducted a cross-sectional study of older individuals admitted with hip fractures to a single NHS hospital over a 10-year period (2009–2019), serving a catchment population of over 410,000 people. Through our participation in the National Hip Fracture Database (NHFD) Audit Programme, data were prospectively collected by a trauma coordinator for patients admitted with a hip fracture from time of admission to discharge.14–16 The data comprised clinical characteristics and care quality. All data were updated regularly into a database managed by the lead orthogeriatrician who checked these data to ensure completeness and accuracy. Further data inspection was carried out by an independent investigator. Any anomalous data were resolved by examining the original data electronically-stored by our hospital.
Preoperative factors included age, sex and residency prior to admission; American Society of Anesthesiologists' (ASA) score; and cognitive function using 4AT (alertness, abbreviated mental test-4, attention and acute change or fluctuating course) in a subsample of 1,116 patients; and anticholinergic cognitive burden (ACB) in a subsample of 529 patients. Postoperative outcome measures comprised mortality; LOS in hospital; new pressure ulcers acquired in hospital; failure to mobilise within 1 day of surgery; and new discharge to higher level of care, including nursing care.
Categorisation of variables
Mobilisation within 1 day after surgery was defined as patients with hip fractures who were able to start rehabilitation no later than the day after surgery.17 Since there exists no definition for prolonged LOS in hospital, we used the threshold according to the top tertile (19 days) in this study. Delirium with or without chronic cognitive impairment was defined as those with a 4AT score ≥4; an ASA grade ≥3 indicated severe systemic disease.18,19 The ACB scale was calculated from scores based on the list of medications developed by the Aging Brain Care Program.20 A high ACB was defined as a score ≥2.
Change in discharge destination was defined as those who came from their own home before hospital admission but did not return home directly after discharge and transferred to places where increased care was provided, including rehabilitation units, residential homes or nursing care.
Statistical analysis
Group data are given as mean values ± standard deviation (SD). Differences in LOS between ETTS groups were tested by analysis of variance (ANOVA) or by Kruskal–Wallis tests (with non-normally distributed data). Differences between categorical outcome variables were assessed by chi-squared tests. Logistic regression was conducted to assess the association of different ETTS groups with outcome measures and are presented in three models: unadjusted; adjusted for age and sex; and adjusted for age, sex, day of admission, ASA and years of data collection. Analyses were performed using SPSS Statistics v25 (IBM, Armonk, USA).
Results
General description
A total of 3,972 patients (1,081 men (27.2%)) and (2,891 women (72.8%)) with mean age of 83.5 years ±9.1 were analysed. A quarter of patients were aged >90 years, 52.7% with an ASA grade ≥3, 20.5% with a 4AT score ≥4 and 10.6% with an ACB score ≥2. There were 3,077 (77.5%) patients who came from their own home, 24 (0.6%) from rehabilitation units, 529 (13.3%) from residential care, 246 (6.2%) from nursing care, 87 (2.2%) from hospital and nine (0.2%) from other types of residence. The proportions of patients in the categories of ETTS <24 hours, 24–35 hours, 36–47 hours and ≥48 hours were 61.7%, 17.8%, 11.1% and 9.4%, respectively. After hip surgery, 49% failed to mobilise within 1 day, pressure ulcers occurred in 3.3%, 5.7% died in hospital and 33.3% (top tertile) of patients stayed longer than 19 days. The median LOS during admission was 13.3 days (interquartile range (IQR) 8.3–23.3). Among patients who were admitted from their own home and survived to discharge, 59.2% returned back home, 25.1% were newly discharged to rehabilitation, 2.1% to residential care, 4.5% to nursing care and 4.0% to other residence (Table 1).
Outcomes of 3,972 patients undergoing surgery for a hip fracture
Factors associated with ETTS
Age and sex
There were no significant differences in age or sex of patients and ETTS. The mean ages (SD) for ETTS <24 hours, 24–35 hours, 36–47 hours and ≥48 hours were 83.6 years (SD 9.1), 84.0 years (SD 9.2), 83.3 years (SD 8.9) and 82.5 years (SD 9.6), respectively (ANOVA: F=2.4; p=0.070). The proportions of patients for the corresponding ETTS categories from either sex were also similar: 62.0%, 18.5%, 10.1% and 9.4% for men, and 61.5%, 17.6%, 11.5% and 9.4% for women (chi-squared 1.8; p<0.621).
Physical status, delirium and ACB score
There was an increasing trend with ASA grade ≥3 among patients who had ETTS <24 hours, 24–35 hours, 36–47 hours, and ≥48 hours: 51.1, 56.1, 53.2, and 57.7% (chi-squared 8.3; p=0.040). The ETTS was not associated with 4AT or ACB (Table 2).
Proportions of patients by elapsed time to surgery
Day of admission
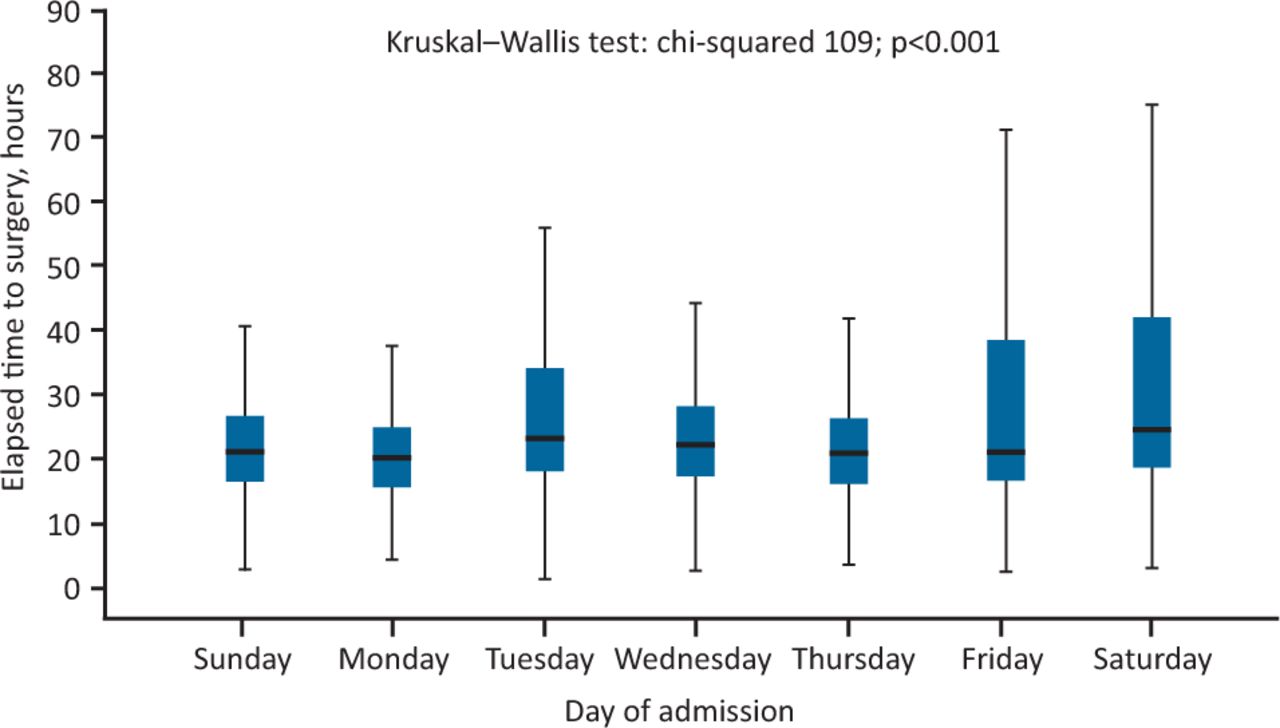
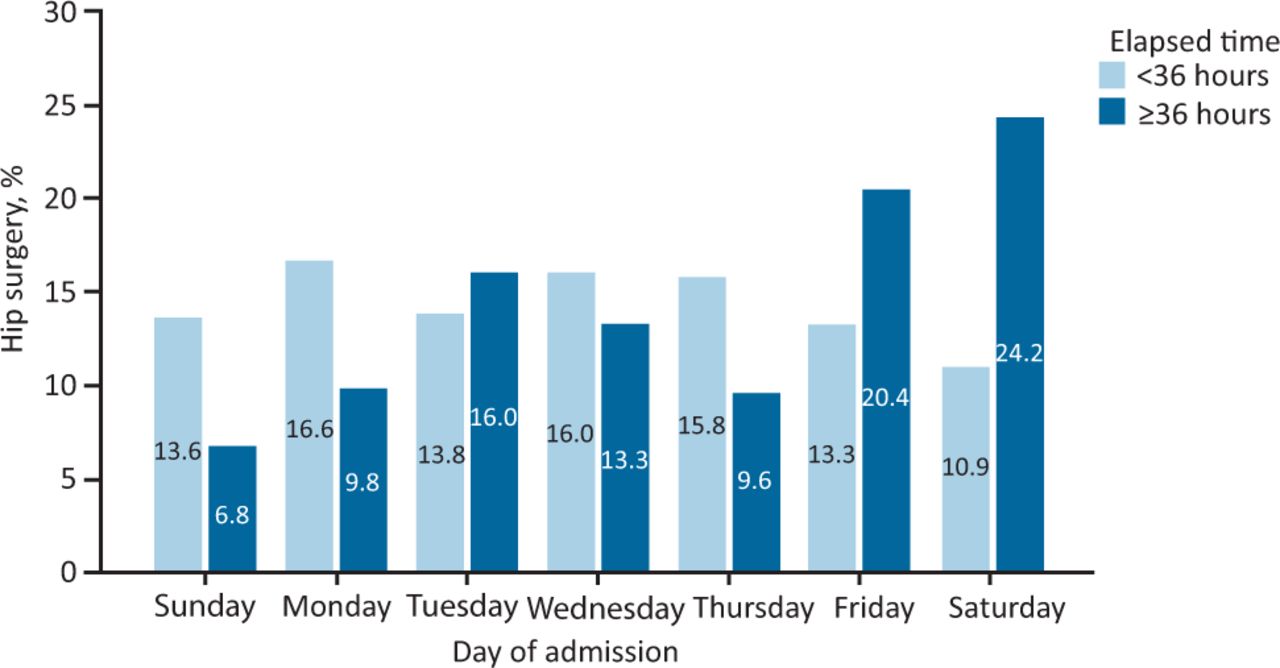
The median time (IQR) of ETTS was shortest at the beginning of the week, starting from 20.9 hours (IQR 16.3–26.6) on Sunday and 20.2 hours (IQR 15.6–24.7) on Monday. This increased to 23.0 hours (IQR 18.0–34.2) on Tuesday, and to 22.1 hours (IQR 17.3–28.1) on Wednesday before falling to 20.9 hours (IQR 16.1–26.4) on Thursday. The ETTS increased again to 22.0 hours (IQR 16.6–38.4) on Friday and peaked at 24.5 hours (IQR 18.7–42.1) on Saturday (Kruskal–Wallis test: chi-squared 109; p<0.001; Fig 1). The proportion of patients with ETTS <36 hours were generally lower at the beginning of the week and peaked on Friday and Saturday (Fig 2). Compared with Sunday admissions, the risk of having ETTS beyond 36 hours were highest on Friday (adjusted OR 3.50; 95% CI 2.43–5.03) and Saturday (adjusted OR 4.70; 95% CI 3.26–6.76; Table 3).
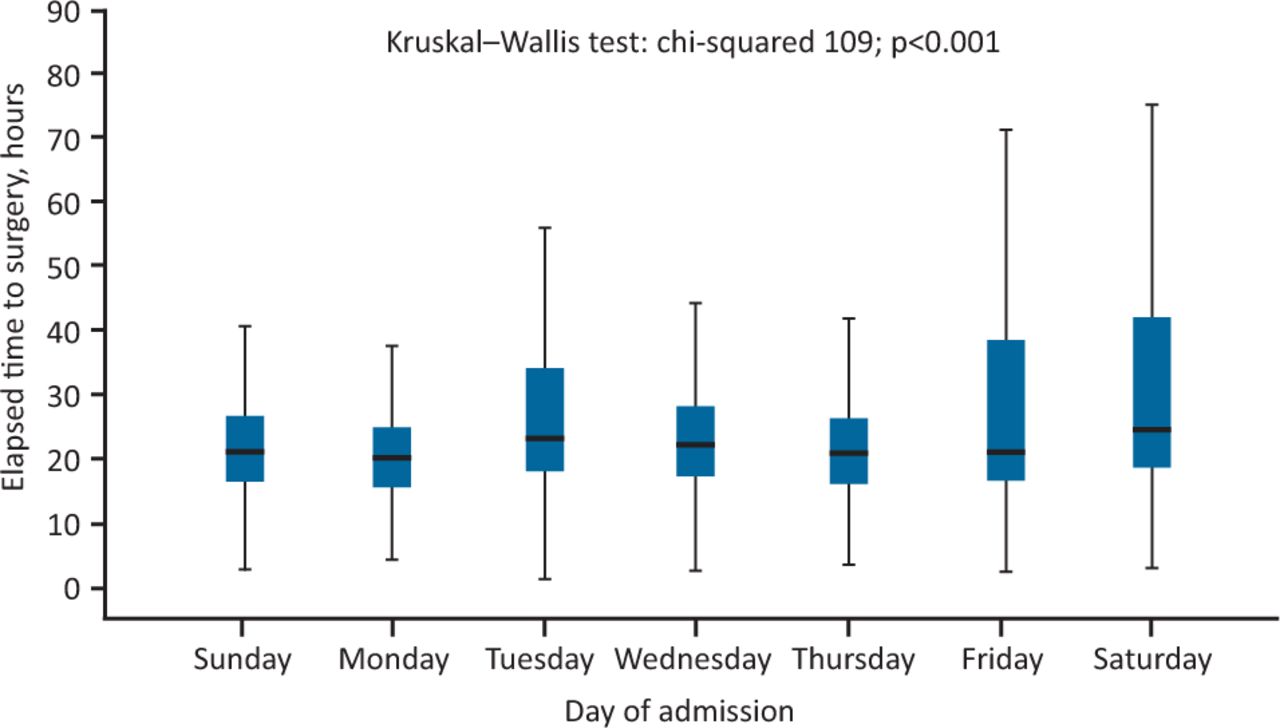
Elapsed time to hip surgery relating to days of admission. Boxes represent median and interquartile range values and whiskers indicate 95% confidence intervals.
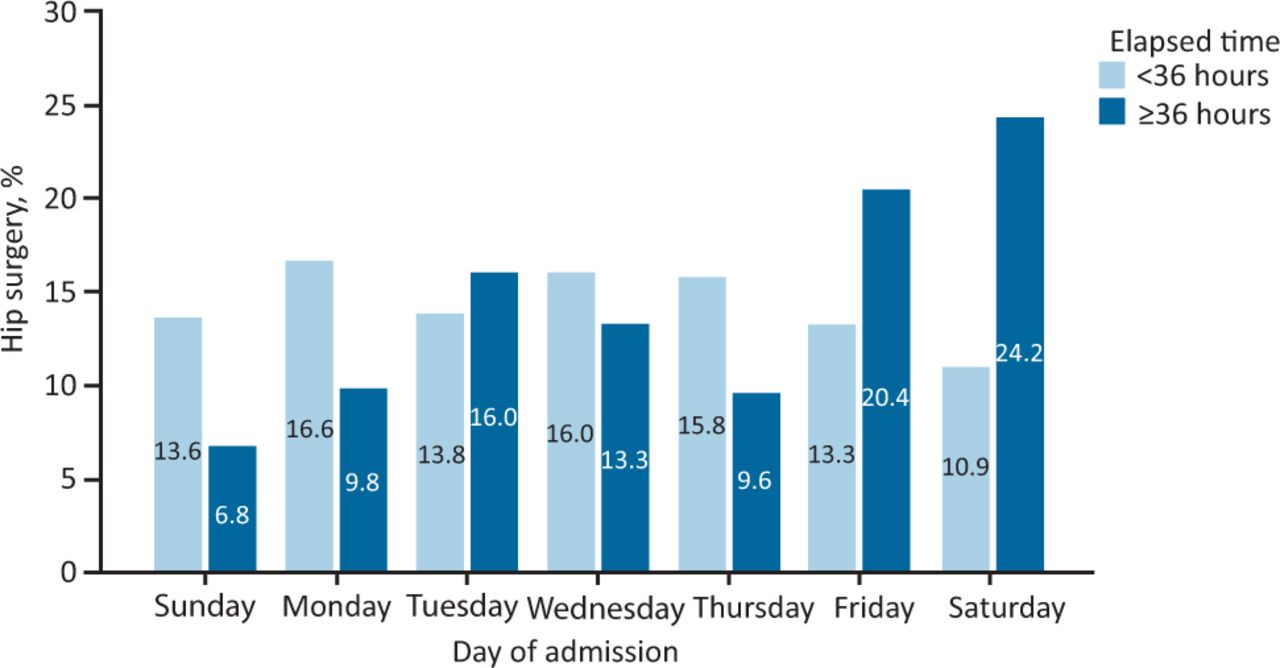
Proportions of patients admitted with hip fractures on different days of the week relating to elapsed time within or beyond 36 hours.
Day of admission and elapsed time to surgery ≥36 hours
Outcomes associated with elapsed time to surgery
Mortality in hospital
The rate of mortality was lowest when hip surgery was performed within 24 hours (4.8%), which rose slightly among those who had surgery between 24 hours and 35 hours (6.3%), and between 36 hours and 47 hours (6.2%). When the ETTS was more than 48 hours, the rate of mortality rose very significantly to 10.3% (chi-squared 19.0; p<0.001; Fig 3a).
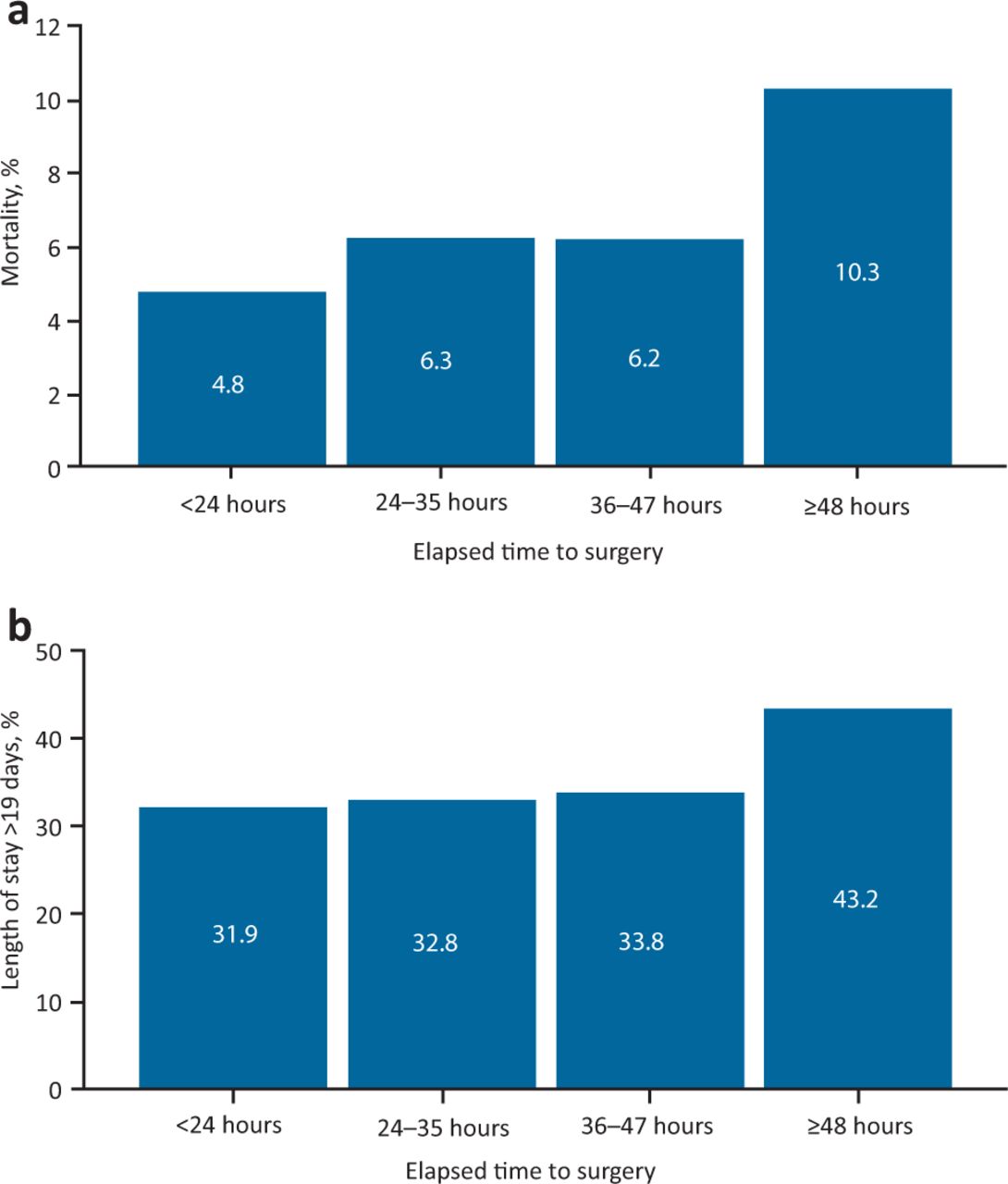
Different categories of elapsed time to surgery. a) Mortality rate. b) Proportions of patients in the top tertile of length of stay (>19 days) in hospital.
Length of stay in hospital
The proportion of patients staying in hospital longer than 19 days (top tertile) whose ETTS <24 hours, 24–35 hours and 36–47 hours rose only slightly from 31.9% to 32.8% and 33.8%, respectively, then sharply to 43.2% for those with ETTS ≥48 hours (chi-squared 18.5; p<0.001; Fig 3b). In addition, the LOS in hospital (median (IQR)) increased gradually with ETTS from <24 hours (12.7 days (IQR 8.0–23.0)) to 24–35 hours (13.5 days (IQR 8.4–22.9)) and 36–47 hours (14.1 days (IQR 8.9–23.3)), and sharply when ETTS was ≥48 hours (16.9 days (IQR 10.8–27.0); Kruskal–Wallis test: chi-squared 49.5; p<0.001); pairwise comparisons showed LOS did not differ significantly between ETTS categories <24 hours, 24–35 hours and 36–47 hours, while LOS in ETTS category ≥48 hours was significantly longer than LOS in all other ETTS categories (Fig 4).

Hospital length of stay relating to different categories of elapsed time to hip surgery. Boxes represent median and interquartile range and whiskers indicate 95% confidence interval.
Compared with ETTS within 24 hours, the age- and sex-adjusted risk of mortality or prolonged LOS did not increase when the ETTS was within 48 hours. After 48 hours, there were increases both in the risk of death (adjusted OR 2.31; 95% CI 1.47–3.65) and prolonged LOS (adjusted OR 1.34; 95% CI 1.02–1.75; Table 4). Further adjustments for ASA grade and day of the week did not substantially change the association between ETTS and mortality or prolonged LOS.
Logistic regression to estimate the risk of adverse outcomes
Failure to mobilise within 1 day of surgery and pressure ulcers
There were no differences between ETTS categories for failure to mobilise within 1 day of surgery, pressure ulcers or discharge destination including to nursing care (Table 2).
Discussion
In this study, both preoperative factors and postoperative outcomes in relation to ETTS were analysed in the same group of patients, a process lacking in the current literature. A number of factors were associated with ETTS, most notably the days of admission. There was also a weak association with ASA, but not with age, sex, delirium or ACB. The risk of mortality and prolonged LOS did not differ between a range of ETTS up to 48 hours but increased sharply thereafter. There was no evidence of detrimental effects in relation to ETTS, including failure to mobilise within 1 day of hip surgery, pressure ulcers or discharge to high level of care (nursing care). Our findings suggest that the recommended ETTS within 36 hours by the Best Practice Tariff for hip fractures is conservative and falls within the margin of relatively low risk.
Factors associated with elapsed time to surgery
Clear patterns of the relationship between days of admission and ETTS emerged. At the beginning of the week (Sunday and Monday), the ETTS was shortest and the proportions of patients with ETTS beyond 36 hours were lowest. By contrast, the ETTS was longest and there were higher proportions with ETTS ≥36 hours towards the end of the week (Friday and Saturday). This ‘weekend effect’ is consistent with those from previous studies.11,21 We also observed a slightly higher proportion of patients with poor physical function (ASA ≥3) to have ETTS beyond 48 hours, which is also similar to findings from previous reports.22 This delay may reflect a period required to stabilise high-risk patients before surgery. However, the ETTS was not influenced by the patients' age or ACB. There was also no association between ETTS and delirium status, in contrast to a previous report of an association between these two variables.23
Elapsed time to surgery and outcomes
Our findings are consistent with previous studies on the association between ETTS and mortality and prolonged LOS.2,4 ETTS has previously been variably reported, ranging from 24 hours to 72 hours, making it difficult to define the precise impact of surgical delays. The present study found no significant differences in outcomes between ETTS up to 48 hours. Beyond 48 hours, the proportions of those dying and with prolonged LOS increased significantly. Our findings of mortality and ETTS are very similar to those observed in a study of Norwegian patients.24 The observations suggest that the recommended ETTS within 36 hours by the Best Practice Tariff for hip surgery may err on the side of caution.
Although weekend admissions are associated with delayed time to surgery, there is little current evidence to suggest an increased risk of mortality.11,25 This is consistent with the current study and suggests a complex chain of events (involving multiple factors) leads to delays in surgery and subsequent outcomes; for example, a study has indicated that patients admitted during holiday period were at higher risk of death than those admitted on weekends or weekdays (8% vs 2.5% vs 1.8%, respectively).13 Crucially, the role of joint care between orthogeriatric and orthopaedic teams has been vital to improve quality of care for patients with a hip fracture. An orthogeriatric service has played an integral part in the management of hip fractures for more than about 11 years at our centre. This service comprises a multidisciplinary team, caring for patients with fragility fractures from the point of admission to discharge, and follows guidance from the ‘blue book’ published jointly by the British Orthopaedic Association and the British Geriatrics Society in 2005.26 The service also participates in a web-based audit tool (the National Hip Fracture Database) that allows hospitals to monitor the quality and outcomes of care provided to the individual patient.27 It also contributes to a 2010 pay-for-performance initiative (the Best Practice Tariff for hip fractures) that rewards hospitals with a supplement for each patient over 60 years of age whose care satisfied a number of clinical standards. These includes a period within 36 hours from arrival in an emergency department, or from the time of diagnosis if an inpatient, to the start of anaesthesia; admission under the joint care of a consultant geriatrician and a consultant orthopaedic surgeon; admission using an assessment protocol agreed by geriatric medicine, orthopaedic surgery and anaesthesia teams; and assessment by a geriatrician in the preoperative period (within 72 hours of admission), postoperative geriatrician-directed multi-professional rehabilitation team and fracture prevention assessments (falls and bone health).1 The level of staffing is also important. A study found that patients admitted during holiday period were at even higher risk of mortality than weekend and weekday admissions (8% vs 2.5% vs 1.8%, respectively).13
It is worth noting that the definition of weekend admissions has been inconsistently reported (ie Friday to Sunday, or Saturday and Sunday).11,28 We found that Friday and Saturday were associated with higher proportions of patients with delay in time to surgery, while Sunday and Monday were associated with the lowest proportion. By contrast, surgery at the weekend has not been shown to associate with increased risk of mortality.21
The evidence for the value of orthogeriatric service in hip fracture management is overwhelming, as indicated by a drastic improvement in a number of key performance indicators including shorter ETTS and LOS in hospital, and a lower risk of complications (such as pressure ulcers and mortality).29 This model should serve as benchmark for other surgical disciplines; for example, the National Emergency Laparotomy Audit (NELA) has shown that older patients who undergo emergency laparotomy have better outcomes if they were supported by comprehensive geriatric assessment, and yet the geriatric medicine co-management is not included in the emergency laparotomy Best Practice Tariff.30,31 There is, therefore, an urgent need for establishing a similar service model as it is for hip fracture.
The strengths of our study include the relatively large sample of a single centre, comprising a homogeneous population. Both the preoperative factors and postoperative outcomes were simultaneously tested in the same group of patients. This study is limited by its cross-sectional design, therefore, causal links between preoperative factors and postoperative outcomes could not be established. As such, prospective studies are necessary to assess the direct impact of 7 day working to remove the weekend effects on adverse outcomes.
Conclusion
Days of admission (towards the end of the week) are associated with delay in time to surgery, particularly beyond 48 hours, for hip fractures, while delay in surgery is associated with increased risk of mortality and prolonged LOS in hospital.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}