Article Text

Abstract
Introduction Improving the quality and activity of clinicians’ practice improves patient care. Performance-related human resource management (HRM) is an established approach to improving individual practice but with limited use among clinicians. A framework for performance-related HRM was developed from successful practice in non-healthcare organisations centred on distributive leadership and locally provided, validated and interpreted performance measurement. This study evaluated the response of medical and non-clinical managers to its implementation into a large secondary healthcare organisation.
Methods A semistructured qualitative questionnaire was developed from themes identified during framework implementation and included attitudes to previous approaches to measuring doctors’ performance, and the structure and response to implementation of the performance-related HRM framework. Responses were analysed through a process of data summarising and categorising.
Results A total of 29, from an invited cohort of 31, medical and non-clinical managers from departmental to executive level were interviewed. Three themes were identified: (1) previous systems of managing clinical performance were considered to be ineffective due to insufficient empowerment of medical managers and poor quality of available performance data; (2) the implemented framework was considered to address these needs and was positively received by medical and non-clinical managers; (3) introduction of performance-related HRM required the involvement of the whole organisation to executive level and inclusion within organisational strategy, structure and training.
Conclusions This study suggests that a performance-related HRM framework may facilitate the management of clinical performance in secondary healthcare, but is dependent on the design and methods of application used. Such approaches contrast with those currently proposed for clinicians in secondary healthcare in the UK and suggest that alternative strategies should be considered.
- Continuous quality improvement
- Performance measures
- Healthcare quality improvement
- Quality improvement
Statistics from Altmetric.com
Introduction
Clinicians represent a significant human capital resource, cost and determinant for quality and productivity in secondary healthcare. There is increasing interest within the National Health Service (NHS) in the role of managing the performance of clinicians to address the conflict between increased demand for specialist services and limited financial resources,1 ,2 supported by the evidence of variation in their productivity and practice.3–5
Performance management is a form of human resource management (HRM) that aims to develop and improve individuals and their practice through feedback, evaluation and participatory goal setting and has three broad aims:6 define and communicate organisational and individual purpose, values and expectations; establish and engage staff with high and poor performance including through reward and recognition and underperformance strategies; and empower staff through mutual dialogue to evaluate their own performance against objectives. Such approaches are associated with improved employee and organisational performance in non-healthcare organisations7 with evidence of benefit in healthcare settings.8
Doctors’ performance in the UK is currently managed through a number of nationally introduced policies. These include: first, the 2003 Consultant Contract reflecting agreed clinical time commitment but without including expected or benchmarked levels of quality of practice or productivity9 (the latter reduced following its implementation);10 second, clinical audit that aims to improve the quality of care by comparing practice to benchmarked quality standards but has had only limited influence;11 finally, the publication of a small number of nationally managed, generic clinical performance indicators (eg, surgical mortality) using centrally determined data.12 More comprehensive measurement of individual clinicians’ productivity and quality of practice has been proposed, for example, through the job planning process,13 supported by performance-related pay structures with fixed term bonuses for perceived good performance.14 But their introduction has remained limited, reflecting inadequate engagement,15–17 processes and indicators,18 ,19 leadership,20 ,21 data validity22 and quality of local information systems.23
Such previously implemented approaches are additionally subject to criticisms24 that they lead to demotivation25 and dysfunctional behaviour,26 ,27 with limited evidence of effectiveness in sustained improvements in productivity and practice.14 By comparison, where performance measurement is undertaken at a central level, it is not commonly associated with engagement, training or support of departmentally based clinical and non-clinical managers who are expected to address identified performance issues with individual clinicians. In some cases projects are fully externally managed by commercial sector consultancy teams using their own measures, data and interpretation.28
In response to this apparent need to more effectively address doctors performance, it is argued, that systems of performance-related HRM may be of value in managing clinicians in secondary care15 in the NHS to improve both practice29 ,30 and productivity.31 Therefore, Trebble et al32 undertook an in-depth study of good practice in performance-related HRM among successful non-healthcare organisations within commercial, public sector and voluntary sectors. This was used to develop a performance-related HRM framework that was implemented into a large secondary healthcare centre. The aims of this study were to evaluate the response of clinical and non-clinical managers to its design and application.
Application of a framework for performance-related HRM of clinicians
The project was undertaken at Portsmouth Hospitals NHS Trust, a large secondary healthcare provider to a population of 650 000 in Hampshire, UK, employing 373 senior grade clinicians (340 consultant and 33 specialist and associate specialist grade medical staff) across 30 departments and 10 divisions led by medical managers at departmental (clinical director or clinical lead [CD]) or senior (divisional or executive [Chief of Service or medical director or CoS]) levels.
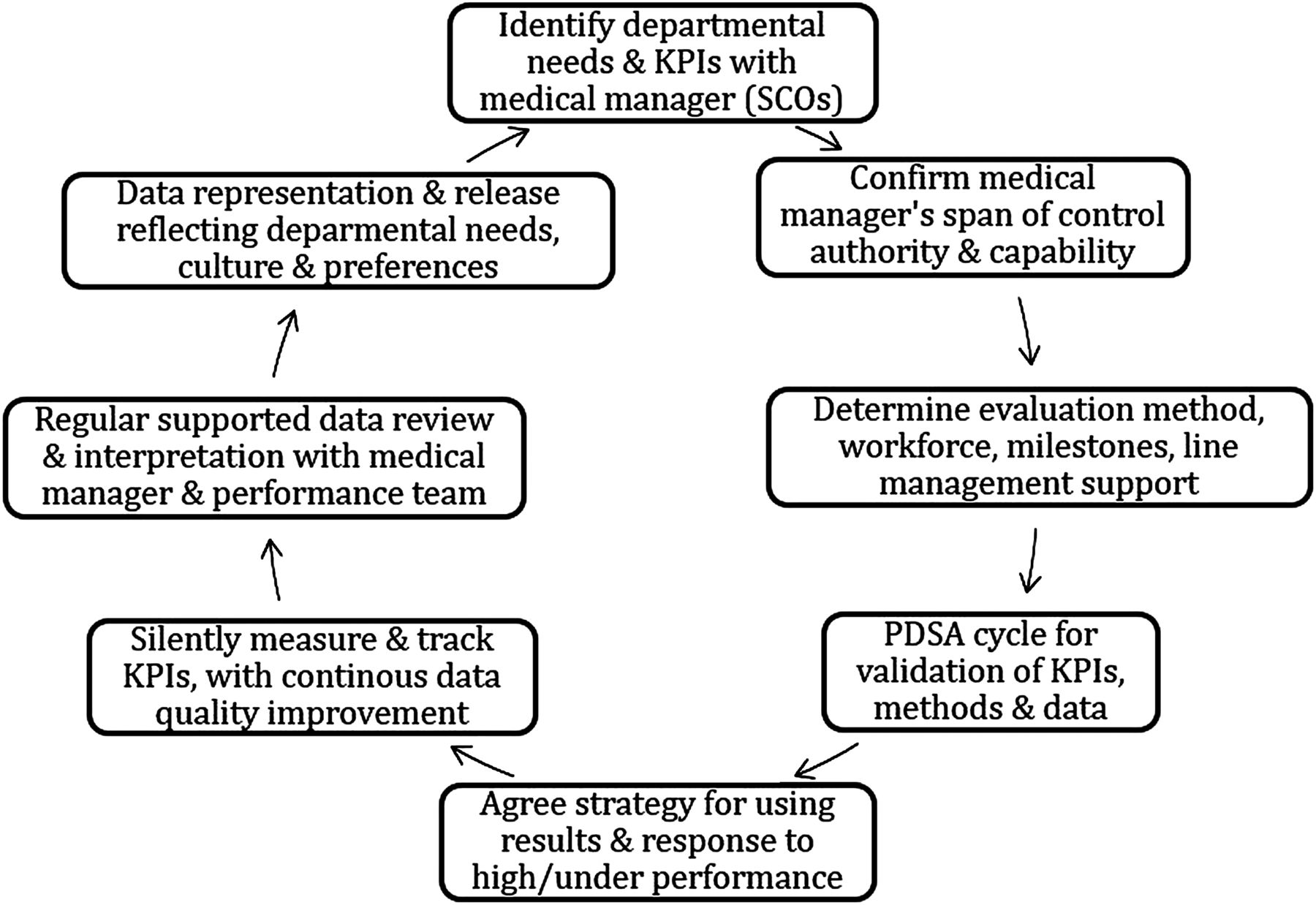
The performance-related HRM framework (figures 1 and 2) was developed based on the observation of successful practice in non-healthcare organisations32 and with reference to published approaches to performance measurement and management33–36 (see online supplementary appendix 1 for full description).

Eight stages of the performance-related human resource management framework (see online supplementary appendix 1).
{kind=link}
{kind=link}
The system of developing performance measurement and data-based decision making for performance improvement (KPI, key performance indicator; PDSA, Plan-Do-Study-Act; SCO, success critical outcomes).
Methods
A semistructured qualitative questionnaire was developed to evaluate the attitudes of medical and non-clinical managers following the implementation of the performance-related HRM framework. The questionnaire was based on themes identified by the project team and involved managers during the framework's implementation. Content validation was undertaken through interviews with three senior medical managers and five senior clinicians not otherwise involved and an interim analysis. An independent, human resources MSc student (MP) was responsible for questionnaire development, data collection, input and analysis.
The study cohort consisted of departmental and senior medical and non-clinical managers (including business intelligence and human resourcing, and administrative staff) involved in the framework's implementation. Participation was offered through email with those agreeing providing informed consent prior to recorded interviews, typically lasting 0.5 to 1 h. Responses were transcribed and anonymised, with only the interviewer aware of the subject's identity. Qualitative data analysis was undertaken through a process of summarising and categorising (coding) of meaning and structuring (ordering) using narrative to identify recurrent themes.37
Ethical approval for the study was granted by University of Southampton (reference number 5858), with local Trust recognition as a service evaluation (according to the policy activities that constitute research at Portsmouth Hospitals Trust, this work met criteria for operational improvement activities exempt from ethics review).
Results
Implementation of the performance-related HRM framework
The framework was implemented by a dedicated project team (including a senior medical manager, human resources manager, business intelligence analyst and administrator) between September 2011 and April 2013 (including 7 months of preparatory work). Departments were recruited through a variety of routes including job planning, the medical human resources department or direct approaches to the project team.
A total of 18 work streams (each representing a clinical speciality) were undertaken involving 14 departments individually or through cross-departmental (eg, the acute medical admission service) work. Each work stream was supported by medical and non-clinical managers at departmental level working collaboratively for the introduction of individualised and team level clinician performance data as a basis for managing performance within their department. This included a willingness to engage in dialogue with individual clinicians relating to variations in performance and how this could be addressed.
The envisaged barriers to the framework's implementation due to resistance by clinicians were not seen with only two departments failing to engage due to perceived inadequate interest (and therefore commitment) by the department and its management team.
Changes in performance measurement and practice among clinicians were demonstrated following the implementation of the framework, examples of which are shown (see online supplementary appendix 2). These included engagement with ward management (eg, providing patient predicted discharge dates for inpatients) and identifying variation in admission rates and length of in-patient stay and theatre utilisation.
Evaluation of the response of medical and non-clinical managers
A total of 29 interviews were undertaken from an invited cohort of 31, and including 20 medical managers (14 departmental, 6 senior) and 9 non-clinical managers. Two medical managers declined (one departmental and one senior) due to time limitations. Departmental medical managers had typically less than 5 years of management experience and senior medical managers more. Among non-clinical managers, three were operational, three human resources, two business intelligence, and one ward administration, with relevant experiences between 5 and 20 years.
Three themes emerged after data analysis and are presented with conclusions supported by verbatim comments from interviewees including medical managers at departmental (clinical director or clinical lead) (CD) and senior (CoS) level, and non-clinical managers and administration staff (managers).
Views of previous performance management practices
The majority of the cohort (19/29) considered that the performance of clinicians was not traditionally managed effectively in employing secondary healthcare organisations, including through job planning or annual appraisals (non-clinical managers in particular (7/9)) with a reliance on clinicians’ self-motivation for performance improvement and delivering outcomes (20/29).
I don't necessarily believe they (doctors) were performance managed with any objectivity, because there was no performance data available to manage with. So it was mostly around experiences, reputation, how they work and how they are seen by their peer group, very much on a subjective basis. (Manager 1)
Two reasons were commonly advocated. First, clinicians were considered to have high levels of autonomy (20/29) and were reluctant to be managed, and medical managers were felt to have only limited or no authority. This was considered, in some instances, to lead to an individualistic approach to patient care with poor adherence to team working or concordance to departmental and organisational objectives.
We work together to meet a demand, but it's like I have a football team, where everyone wants to score a goal. A team has to work together. At the end we all have an aim and we need to work at our particular pitch. If someone holds the ball and wants to keep the ball (resources) to him/herself, then it puts the rest of us in a very difficult situation. (CD 3)
A second factor (19/29) was the perceived poor quality of clinical performance data and limited capability to accurately ‘drill down’ to individual clinician level, further confounded by recognised variation in doctors’ roles, workload and skill mix. This inhibited the valid direct comparison of individual performance and risked potentially erroneous and detrimental judgement of a doctor's practice, leading to poor engagement of clinicians and their medical managers (four of nine managers, 4/14 CDs). From the perspective of senior medical managers and non-clinical managers, further issues included a perceived failure of clinical ownership and an absence of consequences of poor performance (three of nine managers).
Most people knew that the data was wrong, and they ignored it. And no one can really use incorrect data to moderate people. (CD 6)
… Lack of ownership…. They (clinicians) don't always see the problem as their own and try to resolve; they think it more of a managerial responsibility. (CoS 4)
Evaluating the performance of clinicians was considered valuable in terms of ensuring equitable organisational contribution and recognising ‘hard workers’ (17/29). Access to individualised performance data was considered to facilitate this, in addition to informing management discussions, transparently identifying variation of clinician (consultant) performance as a basis for performance improvement, and from the non-clinical manager perspective, facilitating the convergence of individual and organisational aims.
If there are 10 consultants in a certain department, some of them are doing really amazing work for the Trust, and some of them are just working for their own interests. I don't think we have been fair for those people who have been working hard for us. (Manager 3)
However, interviewees commonly reported that discussing and addressing clinical performance issues should be undertaken internally within departments (23/29, including all the non-clinical managers), with the perception that external oversight would not be trusted or allow an adequate understanding of departmental or clinical specific issues. There was also considerable agreement that ownership of performance data should remain with the respective clinicians (21/29) of whom a third felt that this was crucial (7/21), and the majority (14/21) that this was needed for data interpretation using their knowledge of respective clinical roles and work. This was felt to be essential to promote the trust of performance data by clinicians and therefore to changing practice. There was some support (6/14 CDs) for releasing performance data more widely as long as it was felt to be accurate. It was considered that extra-departmental review should remain available in the event that peer pressure was insufficient to resolve performance issues, and potentially supported by human resource managers.
What may look like huge difference on paper may be for very valid reasons. Performance data doesn't tell you anything about what type of patient or complications we are dealing with. Judging performance based purely on figures or numbers, is not quite right (CD 5)
… The way to change peoples’ behaviour and attitude is to give them hard evidence, they need to believe the data and own the data. (Manager 1)
Impact of introducing a performance management framework
The majority of medical and non-clinical managers (27/29) responded that implementing the performance-related HRM framework had positively changed or reinforced their attitudes to clinical performance management. It also positively reinforced belief in the central role of medical managers in such approaches. The interviewees considered that the framework provided accessible organisational (and formal) support for medical managers that was essential for the implementation of clinical performance management (11/29) and specifically by CDs (10/14) addressing performance issue with their colleagues.
Approximately half of the cohort had previously attempted to use individualised data relating to the quality or activity of clinicians in order to improve practice and considered such practice beneficial. However, the majority of those who had not (12/29) demonstrated a positive change in their opinion towards this practice following exposure to the framework, and disproportionately among non-clinical managers. Similarly, interviewees demonstrated a positive change in attitudes towards using individual performance review (IPR) by CDs of their colleagues (10/29), that was subsequently introduced by five CDs (among the remainder of the cohort most considered they were already attempting IPR through job planning, 360° annual appraisal or supervisory meetings).
It demonstrated that performance can be improved with confrontation avoided. (CD 2)
It made us feel more committed to it (measuring doctor's performance). It crystallized things. Use of facts rather than emotions on the things that needed to done for improvements. (CD 10)
… Because the (the performance management) project has given some formalized structure … of justification and validation, it has really empowered us to move our performance forward. (CD 11)
Medical and non-clinical managers demonstrated a uniformly positive response to releasing performance data to clinicians through the approaches included within the framework (13/29), with two more managers already recognising benefits from previous practice. However, in some cases clinicians receiving individualised data were noted to express concerns and challenge the process (6/29), express a lack of trust of data (13/29), that possibly reflected a reaction to being perceived as performing below average. This emphasised the need for accurate objective data. The release of individualised objective performance data was considered to have been motivational for clinicians to improve practice (13/29) (eg, through peer pressure), provide a platform for discussion of performance issues (7/13) and lead to clinician (consultant) engagement.
At the beginning it was difficult for everyone to grasp the idea, but gradually everyone accepted it as we realised it gives us quite valuable information. (CD 12)
… Passive approach initially and surprisingly some of the poor performance people did come to talk to me and they were actually quite surprised that they are not performing as well as they thought they were. (CD 2)
With respect to the consequences of performance evaluation, for example, rewards and recognition or under performance management, managers did not demonstrate a notable change in attitudes following the use of the performance management framework (19/29). However, this appeared to reflect pre-existing beliefs in their importance including motivational but also potentially detrimental effects.
Organisations don't really know how to incentivise people, part of it is because they don't know what to measure. Sometimes it's not about money; sometimes all they (doctors) need is just a simple ‘thank you.’ (CoS 3)
The role of the organisation in clinical performance management
Respondents recognised the importance of a Trust strategy for the implementation and running of a performance management system (26/29). A number of managers (11/29) suggested that such a strategy should be aligned with and developed with clear objectives. It was also advocated that within the strategy, there was a need for clearer definition of ‘poor performance’ (9/29) and a need to understand its underlying causes. Finally, there was a perceived need to develop a forum based learning culture among medical managers to discuss and share their problems and experiences associated with dedicated training “in how to use that information to evaluate performance for medical workers” (CoS 6).
(Trust strategy would assist in managing clinicians by): 1) by showing me who is performing and how; 2) by giving me legitimate authority to address their performance. (CoS 2)
Strategy and a template should be simple, and appropriate for every department, which would provide a framework to have a “discussion”. Performance data should be sent out every 3 months and it should be part of clinical governance meetings. (CD 10)
Discussion
This study evaluated the attitudes of medical and non-clinical managers to the implementation of a performance-related HRM framework developed from observation of the practice of successful non-healthcare commercial, public and voluntary sector organisations. Evaluation of the attitudes of medical and non-clinical managers to its implementation provided a number of key observations. First, that previous approaches to managing performance were ineffective due to the insufficient empowerment of medical managers compared with a relatively autonomous body of clinicians, and the poor quality of performance data that was used to challenge practice. Furthermore, that the performance management of clinicians was more effective if managed internally within departments. Second, that the structured performance-related HRM framework positively changed attitudes of medical managers towards individualised performance measurement and as a basis for performance improvement and was associated with high levels of engagement among medical and non-clinical mangers. Third, considerable importance was attributed to providing accurate data that reflected the need for validation of the processes involved. Finally, the role of the organisation in educating, coaching and supporting medical managers in addressing clinical performance issues was considered essential.
The response of clinicians to the implemented framework contrasts with previous attempts to implement performance management and other forms of performance-related HRM that have been characterised by poor engagement, resistance or confrontation.15 ,17 ,38 ,39 It is advocated by some that this reflects cultural difference in attitudes to change and organisational commitment between doctors and managers40 and by others as reflecting poor quality of management practice.41–43 However, a major difference is that previous performance management approaches have typically relied on nationally provided data considered to be insufficiently validated for individual performance evaluation,44 with external interpretation (eg, ‘naming and shaming’)27 or extrinsic motivation strategies such as financial reward. These approaches have been subject to considerable criticism that they lead to dysfunctional responses39 ,45 or with respect to their potential for misinterpretation, reducing overall quality of care46 and the detrimental effects on doctors where data that is inaccurate or invalid is openly published.47
An explanation of this difference in response to the implemented framework may relate to the multifactorial nature of resistance by clinicians to performance and other HR management approaches.5 Parkin argues that resistance to change can be considered as relating to content (eg, loss of autonomy, power or job security) or process (insufficient trust, information or social influence).48 From a doctor's perspective it may reflect fears of negative evaluation or interference with their work or limited understanding of what it entails.49 Moreover, although participatory approaches to change are commonly advocated and attempted, there is evidence that clear and decisive leadership may be more important even when top down and unilateral.50 The high levels of clinical engagement and low levels of clinical resistance noted to the implemented framework may reflect attempts to address these factors. For example, there was considerable investment by the project team in building trust with medical managers, coaching them in leadership and using performance management to empower their roles with clarity of objectives. Medical managers used their knowledge of their department's work, staff and historical factors to interpret data with a continuing process of adjustment through review and feedback during the course of the project, typical of transformational change.51 Furthermore, medical managers, and their departments, were accorded ‘ownership’ of their own work stream data providing a level of autonomy that may have contributed towards obtaining trust and engagement and allowed the recognition of departmental culture and practice. Finally, the aims and processes involved in the framework were transparent to clinicians, managers and other staff. Such approaches are consistent with those proposed by the British Medical Association13 and identified among high performing secondary healthcare organisations.52
Other factors may have also contributed to the successful implementation of the framework. First, performance data was presented to clinicians by their medical manager team leader (consistent with ‘social influence’) who actively engaged with the responses of their colleagues but without ‘linear causality’ (automatic assumptions from performance measurements without interpretation) or direct accountability (blame).53 Second, the project team undertook cross organisational engagement and training, recognising the contribution of different staff to the framework from data input by administration staff to ensuring concordance to contractual agreements by human resources managers to obtaining support from the senior management. Third, recognition that introducing performance management was as important from an organisational perspective as from that of individual clinicians, an approach that is supported by studies of the cultural characteristics of high performing hospital Trusts.54 Finally, the framework aimed to improve clinicians’ performance through intrinsic motivation strategies25 for example, using self-actualisation, perceived peer group comparisons and feedback on the quality of their service,45 and not extrinsic ones such as increased pay.
The framework in this project also differed from performance management approaches reported in the literature, including in healthcare, that focus on the appraisal process and its consequences.55 ,56 The approach taken in the current framework was more consistent with the holistic approach reported by Armstrong that involves individuals and teams using shared understanding to recognise and address performance on an on-going basis with an emphasis on leadership and developmental approaches.57 Also, Otley's management framework approaches performance focusing on five complementary themes that include organisational strategy, objectives and feedback loops58 with the subsequent theoretical framework that includes both aspirational and practical components of a performance approach aligned to the needs of the organisation.59 The framework is therefore consistent with strategic HRM 60 with similarities to high performance work systems61 that have also demonstrated benefits in improving performance in healthcare.62
The findings of this study have implications for the management of clinicians within the NHS. This includes that, first, there may be a need to review how medical and non-clinical managers are trained and supported and particularly in how they address performance-related HRM of their colleagues. Second, that there should be an emphasis on performance measurement in secondary healthcare organisations conforming to the proposed requirements for a sustained performance culture and clarity of what this entails, and developing a sense of community and common purpose, honesty and truth about practice, ownership and accountability as groups and individuals.63 Third, recognition that healthcare performance measurement alone is insufficient to promote sustained and supported productivity improvements, but requires an inclusive HRM strategy that “nurtures and encourages the pursuit of efficiency”64 from the clinician treating patients to the executives setting organisational strategy.
This study is subject to a number of potential criticisms. First, there is an absence of clinical data to confirm the effect on clinical outcomes. Second, the study does not provide objective evidence of sustained performance improvement that would require a longer period of evaluation. Finally, the transferability of management systems from external organisations to healthcare remains controversial although supported by advocated similarities in management practices and response to change,21 ,65 ,66 and that good practice is independent of its operating environment.26 ,67
In conclusion, there is a need to introduce effective strategies to transform healthcare quality and productivity in secondary healthcare in the NHS. This study suggests that a performance management framework based on successful practice in non-healthcare commercial, public and voluntary sector organisations, can engage medical and non-clinical managers with performance measurement, and provide a system of implementation for performance improvement. If the differences in clinical engagement between the respective approaches are confirmed on a wider scale it may suggest that alternative strategies should be considered in the use of healthcare data to improve the performance of clinicians in the NHS.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
Footnotes
-
Contributors TMT, NH, NC and MP were responsible for study design; MP was responsible for data collection and analysis; TMT was responsible for preparatory work, the development of the framework and manuscript preparation; TMT, NH and RH were responsible for performance data collection and analysis; PMH, TP and NC contributed to preparatory work and manuscript preparation.
-
Funding This work was supported through funding from NHS South Central Strategic Health Authority.
-
Competing interests None.
-
Ethics approval Ethical consent approved through University of Southampton. Reviewed and confirmed as service evaluation by local research department Portsmouth Hospitals Trust.
-
Provenance and peer review Not commissioned; externally peer reviewed.