Article Text

Abstract
The structure of postgraduate medical training rightly puts enormous emphasis on gathering clinical experience and constantly updating knowledge of relevant medical research to use in practice. At most, this can be contrasted with the slight emphasis on clinical leadership and acquiring the skills to effect change and improve the quality of care. Doctors play central roles in orchestrating the clinical management of patients across multiple settings within the healthcare system. They also routinely encounter the many problems within the systems that they work, affecting their own practices as well as those of other healthcare professionals. They thus represent a tremendous resource for identifying solutions to these problems and playing leadership roles in implementing them. However, physician training programs focus almost entirely on the knowledge and skills to manage clinical problems, with almost no training in skills related to healthcare management or effective quality improvement. In this article, we describe one attempt to improve this situation. In four hospitals in the Severn Deanery in the Southwest of England, first-year doctors carry out a structured and supported quality improvement project of their choice throughout their first year of training. To date, 30 such projects have been or are being run. This has significant benefits for both the trusts they are working for as well as for their own professional development. We describe the successes, difficulties and future of this programme.
- Quality improvement
- Leadership
- Medical education
- Patient safety
- PDSA
Statistics from Altmetric.com
Introduction
The structure of postgraduate medical training rightly puts enormous emphasis on gathering clinical experience and constantly updating knowledge of relevant medical research to use in practice. At most, this can be contrasted with the slight emphasis on clinical leadership and acquiring the skills to effect change and improve the quality of care. Doctors play central roles in orchestrating the clinical management of patients across multiple settings within the healthcare system. They also routinely encounter the many problems within the systems that they work, affecting their own practices as well as those of other healthcare professionals. They thus represent a tremendous resource for identifying solutions to these problems and playing leadership roles in implementing them.1 However, physician training programmes focus almost entirely on the knowledge and skills to manage clinical problems, with almost no training in skills related to healthcare management or effective quality improvement. All the authors of this paper are relatively senior doctors and can attest to the fact that despite being ideally placed to improve systems in healthcare for the first few years of practice they made no improvements to the systems they were working in, and in fact were unaware that they were working in systems. This is still the case for the overwhelming number of doctors. In the 21st century, especially given the current financial situation and demand for culture change in the NHS, this has to change. Doctors need to both do their jobs and also work to improve their jobs by improving the systems they are working in.2
This is not for the first time of saying and has been written and spoken many times elsewhere.3 ,4 Furthermore, doctors’ professional responsibility to fulfil both their direct clinical care role and contribute to improving the quality of services has been explicitly described by the GMC.5
There are multiple schemes that have targeted small numbers of junior doctors (the icing on the cake) that have had success at engagement and education in quality improvement.6–8 These schemes are addressing the ‘icing’, but it is the ‘cake’ we need to concentrate on. The burning question is how do we change the culture to make continuous quality improvement part of the normal day-to-day practice of all doctors from the start of their postgraduate career (and for that matter all healthcare professionals)?
Some work has already begun, the Foundation Doctor Curriculum now states that all foundation year 1 (F1s) should be involved in quality improvement, and the Royal College of Physicians ‘Learning to Make a Difference’ programme has begun to engage doctors of more than 2 years experience.9 ,10 The London Deanery ‘Beyond Audit’ programme has also started to involve all trainee doctors in quality improvement.11
In this article, we describe our work to implement a high-quality programme for F1s in one, then four acute trusts of the Severn Deanery, and how by the intake of August 2015, all the eight acute trusts in Severn will be running a programme where doctors start their postgraduate careers learning both about clinical management of patients and quality improvement.
The Severn Deanery foundation doctor quality improvement programme
The Severn Deanery is one of the postgraduate education structures in the Southwest of England. It has 2300 trainees across eight acute NHS hospitals covering a population of around three million people. Each year, 280 doctors commence as F1s.
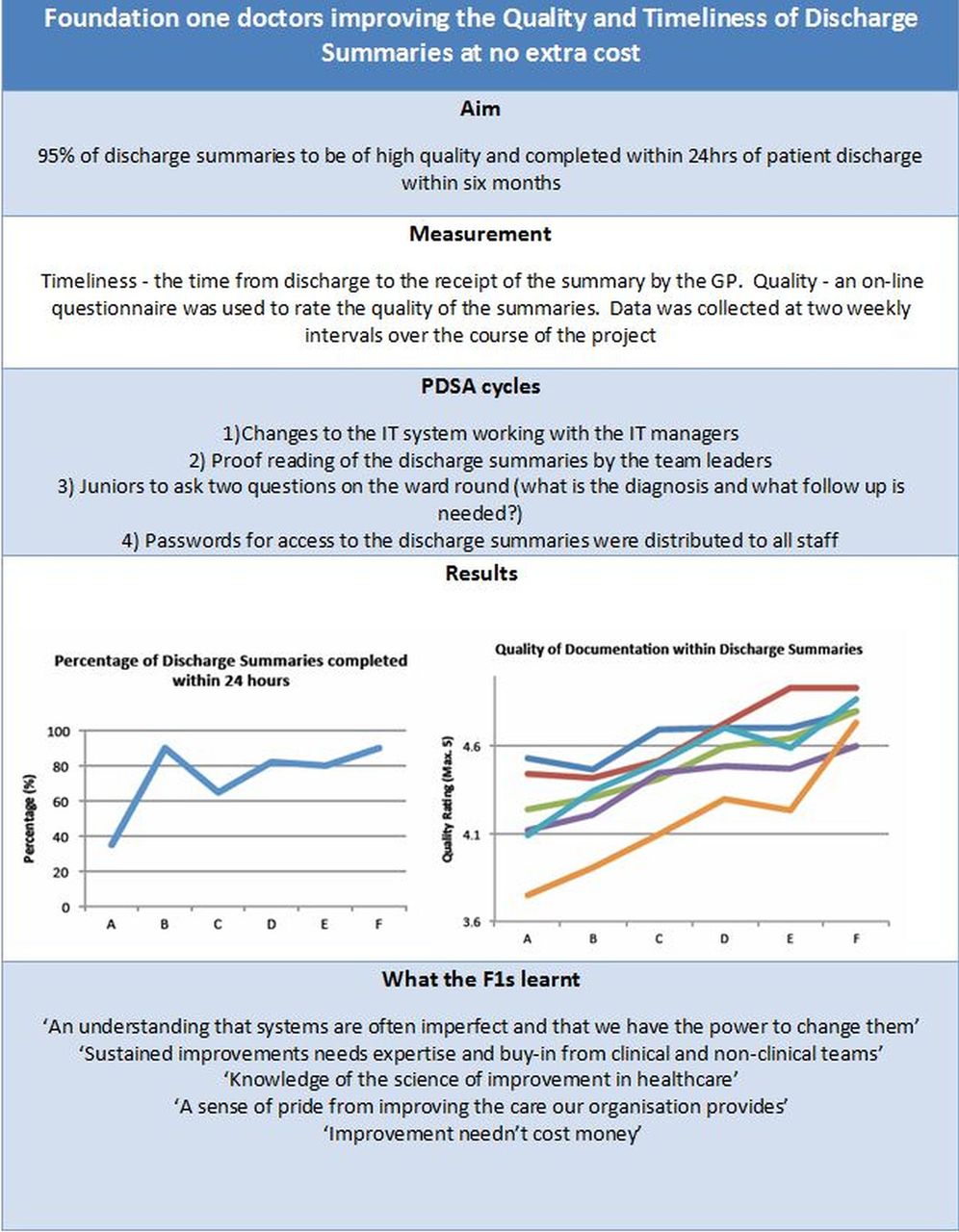
In 2009, we trialled a programme in one hospital (Taunton and Somerset NHS Foundation Trust) that was originally developed by Peter Wilcock in Salisbury Hospital NHS Foundation Trust.12 In the first year of this programme, 10 F1s volunteered, and a single project on the timeliness and quality of discharge summaries was carried out (see figure 1). This proved to be a politically astute choice of the F1 doctors as it received both attention and praise from the Trust Board, as this was significant and relevant to an issue with the local commissioner for health, Somerset Primary Care Trust. From August 2010, based on what was learnt from the pilot project, the programme has been run yearly for all F1 doctors. To date, the programme has run a further 14 projects (4–6 per year) in Taunton. From that beginning, this programme was spread to North Bristol NHS Foundation Trust (2010), United Bristol Hospitals NHS Foundation Trust (2011) and the Royal Bath United NHS Trust (2012). The plan is that by 2015 it will be run in all hospitals across the region for all 280 F1 doctors.

{kind=link}
An example improvement project.
The programme consists of a structured and supported quality improvement project run by groups of F1s. During their induction before they start as F1s, the programme and The Model for Improvement are explained in a brief session. The F1s are then allowed to settle into the role of being a doctor, but they are asked to look out for any systems that they think are unsafe or just plan inefficient (ie, what makes the F1's job harder than necessary). During the first few months there are teaching sessions in their compulsory teaching time on topics, such as patient safety, team working and system measurement. In the autumn (end of September) a longer session takes place to choose the service improvement projects they will work on and which team they will join. As many F1s as possible attend this session, together with the group mentors, the quality leads for the hospital and at least one hospital executive. The F1s identify the problems they have observed and through facilitated discussions, the ideas are narrowed down to feasible projects; with the number of projects matching the number of groups in the programme, with each group consisting of around 10 doctors. The project has to be such that it can be feasibly addressed in 9 months with limited resources (no budget line is attached to this work). Assigned to each group is a mentor who helps them but does not do the work. The number of F1s varies between 30 and 50 in the hospitals, so there are between three and six projects run each year in each hospital.
Over the next 6–8 months, the F1s organise themselves and apply The Model for Improvement to affect change. Practically, this involves measurement of the current situation for 1–2 months, identifying who does what, frequency of events, pathway and so on. They plan their own interventions and test these through repeated PDSA (plan-do-study-act) cycles, while collecting data to evaluate the changes. A final presentation of the project to the Trust's Executive Board and Clinicians in July of their F1 year is a celebratory occasion with success and failure treated just the same. This forum provides the opportunity for F1s to showcase their work, and has also been a highly informative ‘eye-opener’ for the senior clinicians and executives of the reality of their hospitals. The structure of this programme remains fundamentally unaltered from its original trial, however, subsequent adaptations are tested each year to suit local expertise and constraints allowing for progressive development.
Successes and achievements of the programme
Since its start 4 years ago, 30 projects have been completed or are in progress by the F1s. Many of these projects represent a small but critical contribution to patients’ pathways, and are often problems that are unknown or unrecognised by senior clinicians and managers. Projects include weekend handover, discharge summaries (see figure 1), ECG verification, utilisation of common clinical equipment boxes, timely phlebotomy, discharge blood checking, extended nil-by-mouth times, venous thromboembolism reassessment and many more. The output in the first three years of the Taunton and Somerset experience comprises 14 various presentations of the F1s work at regional, national and international conferences including four prizes and two publications to date.
The benefits of this programme are:
-
It delivers quality improvement for the hospital directly improving care and creating a more efficient service.
-
It teaches the next generation of clinical leaders crucial quality improvement and patient safety skills in a real and meaningful way. As this is experiential, learning by doing it ‘sticks’ in a very different way to traditional teaching and courses. This is an excellent format that cultivates the shared leadership skills described in the Medical Leadership Competency Framework, in particular, the softer skills of ‘working with others’.13
-
A further benefit of the programme is the excitement generated by the junior doctors among the other healthcare workers in the hospital, one of the programme mentors commentated ‘we cannot wait to see what innovations they will come up with this year’.
-
Most importantly is the effect it has on the doctors as members of staff in the hospital. Each new group of doctors are highly driven and intelligent; sadly, early clinical practice often starves them of autonomy and they often perceive they face a working environment that is not receptive to their ideas of change.14 This work engages the F1s with the mission and vision of the organisation to deliver high-quality healthcare and make the most of resources which importantly includes the energy of these highly motivated people.
Key learning
Throughout the several PDSA cycles the programme has been through, we have identified several core principles that seem to hold true in different settings with different groups of F1s:
-
Self-determination. The single most important factor is the F1s must choose the project themselves, if they do not have ownership of this it will never work well. From those with previous experience of what works, they can be advised about the choice, but the idea has to be theirs.
-
Groups are crucial. The projects take time and effort, and attempting them individually will almost certainly fail. From our experience, group sizes of 6–10 seem ideal.
-
Volunteers are better. In the same way as the first point, if the F1s feel they are doing the projects because they want to it will work better. This does pose a slight challenge as the point is to up-skill all doctors (the ‘cake’). One compromise that we have found very effective is to make the first sessions compulsory, and for all F1s to choose a project group and then further participation is voluntary. In practice, most F1s will then carry on their projects and somewhat ironically more will actually ‘do’ a project if it is voluntary rather than compulsory.
Difficulties in spread
This programme has been delivered by the enthusiasm of the authors and others. No specific time or resources were given to it initially, and it has only been once success has been demonstrated that hospital trusts have started to allocate time and resources to it. This has made spread difficult. Although trusts have personnel with enough quality improvement knowledge to organise such a programme, they often do not have the capacity to move this forward. Conversely, permanent postgraduate education staff who theoretically have the time to teach and mentor this sort of programme do not have the appropriate quality improvement knowledge and contextual experience.
Practically, spread has been achieved by the movement of two of the authors who are still in training and so have rotated to other hospitals in the region, copying the programme to their new hospitals. This has been both a strength and weakness of this programme. By spreading it very much from the bottom up it has been effective in a way that a top down dictated approach would have failed, but against that spread has been slow. The basic problem is that most ‘senior’ doctors are not familiar with quality improvement and The Model for Improvement specifically, and are thus unable to mentor. This will be hard to change, but as we will outline below, a solution exists in the now increasing number of junior doctors who are graduates of this programme.
The future
The 64 000 dollar question is how to spread a programme that is largely based on the enthusiasm of a few committed individuals. Just telling hospital trusts that they must do this programme will not result in a real change, as they may just pay lip service to this, and the term ‘quality improvement project’ could become as unpopular to junior doctors as ‘clinical audit’ has become.15
So how do we translate this approach further? First, quality improvement methodology is spreading among consultants. Foundation directors can build their skills to use with the F1s and continuing support from the Local Education and Training Boards will progress this. In addition, using the skills of the graduates of this programme is a growing resource already. As they finish their first year as doctors, and their first quality improvement project, a proportion will move to another hospital in the region and move further away as the years go on. These juniors with real experience of running quality improvement can themselves mentor and continue the programme in new hospitals and healthcare settings. The F1s from the first year of the project are now in their fourth year as doctors and are actively engaged in mentoring new project groups. It is through this gradually increasing number of ‘quality improvers’ that we will be able to achieve our aim of having all F1s finish their first year as doctors with a comprehensive understanding of how to improve the systems they work in; we will have ‘baked the cake’.
Footnotes
-
Contributors All authors did all the following three things: (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.