Article Text

Abstract
Over two decades have passed since posterior reversible encephalopathy syndrome (PRES) was first described in 1996. It has becoming increasingly recognised because of improved and more readily available imaging modality. The exact pathophysiological mechanism is not completely understood and remains controversial at present. Precise diagnosis is essential to guide prompt, proper management. Our ability of differentiating it from other acute neurological disorders is likely to improve as we learnt more about the spectrum of this entity in the last 20 years. We emphasise the importance of recognising its diagnostic criteria and biomarker, which would be of great relevance to either outcome evaluation or study design. PRES has a favourable prognosis generally, but neurological sequelae and even fatalities can occur, especially in severe forms that might cause substantial morbidity and even mortality, particularly when the syndrome is complicated by intracranial haemorrhage or brain infarction. In this review, the pathophysiology, approach to diagnosis, some controversies as to the prognosis, as well as the future research direction of PRES are described.
- posterior reversible encephalopathy syndrome
- pathophysiology
- diagnosticcriteria
- imaging biomarker
- prognosis
Statistics from Altmetric.com
- posterior reversible encephalopathy syndrome
- pathophysiology
- diagnosticcriteria
- imaging biomarker
- prognosis
Introduction
Posterior reversible encephalopathy syndrome (PRES) was likely first described as a clinical syndrome with similar imaging appearance encompassing several aetiologies by Dr Hinchey and colleagues in New England Journal of Medicine in 1996.1 PRES refers to a clinicoradiological disorder of reversible subcortical vasogenic brain oedema in patients with classic acute neurological symptoms (eg, seizures, encephalopathy, headache and visual disturbances) in the setting of pre-eclampsia/eclampsia, renal failure, hypertension, cytotoxic or immunosuppressive medications, autoimmune disorders, sepsis, thrombocytopaenia, hypocalcaemia, alcohol withdrawal and many other potential causes2 3; however, notably, the term ‘hypertensive encephalopathy’ and the reversibility of such had been described numerous times over earlier decades.4 Initially termed ‘reversible posterior leukoencephalopathy syndrome’, a new name, ‘posterior reversible encephalopathy syndrome’, was proposed, as it became clear that cortical areas were also commonly affected, particularly in earlier or milder disease, while the deeper white matter was typically involved in more severe cases.5 Neuroimaging usually reveals vasogenic oedema that is cortical–subcortical in milder cases and being located predominantly in bilateral parieto-occipital regions, followed by high posterior frontal, temporal, cerebellar, basal ganglia and brainstem locations, respectively.6 7 PRES is generally considered to be a reversible entity both radiologically and clinically, and typically has a favourable prognosis, although uncommonly cytotoxic oedema or haemorrhage leads to complications or long-term neurological deficits in a minority.7 8
Clinicians in multiple disciplines such as neurology, obstetrics, nephrology, emergency or intensive care centre, oncology, rheumatology, haematology, and solid organ transplantation surgeons may potentially encounter such patients as with PRES. Although studies on PRES have increased exponentially, the scientific literature on this disorder is comprised of case series and many case reports; however, the incidence in the general population is still unknown. The increasing utility of multimodalities MRI in the last two decades has led to recognition, characterisation and familiarity of this syndrome, although most of the evidences are obtained from single-institution, retrospective, observational studies. Everyone involved in the management of patients with acute neurological symptoms has been faced with the possibility of diagnosing ‘PRES’. In clinical practice, this syndrome has developed into an umbrella term for various types of encephalopathies as reported by the investigators. Unfortunately, it is often proving a distraction from the main clinical issue, which is to identify the cause of the problem. To some junior colleagues and colleagues from other specialities, it is unclear that to call a condition of PRES is not the end of the diagnostic process but only the beginning of it.
In this review, the pathophysiology, approach to diagnosis and prognosis, as well as the future research direction of PRES are described. We emphasise the importance of recognising the diagnostic criteria and biomarker, which are not defined previously yet, and would be of great relevance both to outcome evaluation and study design. Most importantly, some controversies as well as possible study directions for future research of PRES are highlighted.
Pathophysiology
The major aetiologies of PRES comprise hypertension, eclampsia, immunosuppressive/chemotherapy medications (such as ciclosporin A, tacrolimus, methotrexate and others), sepsis and autoimmune disorders. It seems that PRES may be multifactorial, and how the pathophysiology may lead to PRES in each is diverse. The lowering of the cerebral autoregulation curve leads to PRES in hypertension and eclampsia. However, chronic endothelial injury/ischaemia may play a key role in lowering this in those two aetiologies, while ciclosporin and tacrolimus seem to injure the endothelium in a different way, which is why more than 50% of patients with PRES related to those two medications do not have a clinically elevated blood pressure. For autoimmune disorders, it is presumably to be endothelial injury induced by antigen–antibody interaction and inflammation of endothelial cells.
While the causes of PRES are numerous and diverse, they all share key pathophysiological events including activation and injury of the endothelium, activation of the immune system and associated release of cytokines.9 This is usually followed by hypoperfusion of multiple organ systems including the brain, abnormal vascular autoregulation, breakdown of the blood–brain barrier (BBB) and subsequent brain oedema.10 However, the exact pathophysiological mechanism is not completely understood and remains controversial at present. At least four distinct theories with two contrary pathophysiological mechanisms for PRES have been proposed.11
The ‘vasogenic’ theory is the more traditional hypothesis, which postulates that severe hypertension leads to vascular autoregulation breakthrough, followed by cerebral hyperperfusion with associated vascular injury, damage to the BBB and secondary vasogenic oedema.10–12 This theory may accurately describe the pathophysiology of PRES in patients with severe hypertension, which exceeds the upper limit of autoregulation at mean arterial pressures (MAPs) greater than 150–160 mm Hg. This theory effectively explains the resolution of symptoms and cerebral oedema after the normalisation of blood pressure. However, this theory does not account for the full spectrum of pathophysiology of this disorder, as most patients with PRES present with moderate hypertension below this MAP limit, and since 20%–30% of cases present with nearly normal blood pressure.13 Additionally, recent studies have reported that cases with severe hypertension have lower cerebral oedema than cases with normal blood pressure.14
The other three alternative theories share a similar mechanism, where endothelial dysfunction causes resultant hypoperfusion and ischaemia.6 15 The ‘cytotoxic’ theory posits that the primary insult is due to endogenous stimulus such as chemokines or exogenous toxins, such as chemotherapy or immunosuppressive therapy.11 The ‘immunogenic’ theory suggests a primary inflammatory insult that involves T-cell activation and cytokine release. According to both of these theories, one of these aforementioned primary process causes subsequent endothelial dysfunction that can lead to vasoconstriction of microvasculature, which may be further exacerbated by hypertension and an associated autoregulatory response.11 Cerebral vasoconstriction may then be followed by cerebral hypoperfusion and ischaemia, ultimately resulting in the vasogenic oedema characteristic of PRES.10 This has traditionally been thought to have a more ‘posterior’ appearance on imaging due to the histological presence of relatively less sympathetic innervation of the arterioles in the posterior circulation relative to the anterior circulation, in which such innervation is thought to have a protective effect via autoregulation. 16 17 Antihypertensive treatment reduces vasoconstriction due to this ‘protective’ autoregulatory response, and may therefore be effective in reversing the findings of PRES. In a similar fashion, the ‘neuropeptide’ theory postulates that the key mechanism involves release of endothelin-1, prostacyclin and thromboxane A2, which leads to vasospasm and ischaemia followed by vasogenic oedema.11 Each of these three theories described above can account for PRES in normotensive and moderately hypertensive patients. Additionally, these pathophysiological mechanisms are supported by recent magnetic resonance (MR) perfusion investigations, which have demonstrated cerebral hypoperfusion in PRES.10
Although there are at least four different pathophysiological concepts as we summarised that may create the imaging findings underlying this ‘syndrome’, and in reality they share the common imaging and clinical manifestation of very different diseases. However, several cerebral perfusion imaging studies in patients with PRES have reported conflicting results.10 ,18–21 Increased perfusion has been observed in oedematous zones, which confirms the hypothesis of cerebral hyperperfusion as a result of a blood pressure that exceeds the upper limit of cerebral autoregulation.22 23 In contrast, single-photon emission computed tomography (SPECT) and MR perfusion imaging demonstrate hypoperfusion in lesional areas in patients with PRES of varying aetiologies.18 24 Different perfusion patterns in PRES may also be explained by the variety of aetiological aspects, causing a diverse pathophysiological response; furthermore, patients may have variations in vasculature as well as potentially variations in collateral circulations, which have yet to be studied in detail by perfusion imaging in patients with PRES. In line with the main hypotheses for the pathophysiology of PRES, conflicting perfusion patterns may be a result of primary hypertension and cerebral hyperperfusion versus endothelial dysfunction, cerebral vasoconstriction and subsequent cerebral hypoperfusion. Such findings on perfusion imaging may be reflected by prior angiographic studies, which have observed vasculopathic findings in many patients with PRES on magnetic resonance angiography (MRA) or conventional angiography.25 26 Such vasculopathic findings are usually reversible and include cerebral vasoconstriction, vasospasm (diffuse or focal) and string-of-beads stenosis, typically in the posterior circulation.10
Given the heterogeneity of aetiologies of PRES, clinical course and imaging manifestations, there are different versions or combinations of these mechanisms that may be responsible in specific cases. In order to clarify this, in the future, it may be better to refresh this issue by defining the groups of underlying conditions that may present as ‘PRES’ and differentiate PRES accordingly. This would allow to discuss the pathophysiological features and consecutive imaging and clinical findings for a specific subtype of PRES and aid in educating the uninformed readers about the whole concept.
Diagnostic criteria
Established diagnostic criteria have been lacking so far and clinical as well as imaging findings are often non-specific. Therefore, the diagnosis of PRES can, at times, often only be made after excluding other diagnoses. The presence of neurological symptoms, vasogenic oedema as the leading neuroimaging finding and a clinical context of associated comorbidities or trigger factors are usually suggestive of PRES.27 Provenzale et al included the following criteria for diagnosis: (1) regions of hyperintense signal primarily within posterior white matter; (2) presence of at least one of risk factors for PRES; and (3) absence of another likely cause of white matter lesions.28 Casey et al suggested that a ‘cortical and subcortical’ appearance is characteristic on fluid attenuated inversion (FLAIR) MRI.5 Covarrubias et al used the following inclusion criteria: (1) acute clinical presentations; (2) the presence of a known risk factor for PRES; (3) MRI findings consistent with PRES.29 Bartynski et al performed a series of PRES studies using the criteria for confirmation of PRES that include: (1) complete or partial expression of the typical PRES pattern; (2) reversibility on follow-up imaging; (3) vasogenic oedema as demonstrated by diffusion-weighted imaging (DWI); and (4) a presentation consistent with clinical neurotoxic syndrome.10 13 To determine the incidence of typical and atypical regions of involvement as well as unusual imaging manifestations, McKinney et al used criteria for inclusion as a confirmed case of PRES, which included a clinical diagnosis of PRES based on discharge data and an appropriate clinical basis for PRES based on symptoms of a neurotoxic syndrome in combination with typical imaging findings consistent with PRES.3 Brain MRI studies of identified candidates were scrutinised for signs compatible with PRES in a series study from Berlin by Liman et al, variable degrees of vasogenic oedema, variable degrees of reversibility and a clinical constellation compatible with PRES.30Another retrospective cohort study from Europe by Legriel et al defined PRES as a variable combination of acute neurological clinical changes associated with neuroimaging findings consistent with PRES, including vasogenic oedema measured by DWI and apparent diffusion coefficient (ADC) values or at least partial reversibility on follow-up imaging when DWI were not available.31 Gao et al defined PRES fulfilling the following criteria: (1) presentation with acute clinical symptoms; (2) presence of known risk factors; (3) distributions of T2 weighted imaging (T2WI) or, T2-fluid attenuated inversion recovery (T2-FLAIR) hyperintensities compatible with typical PRES imaging patterns; (4) clinical and imaging abnormalities mostly or completely resolved after proper therapy; and (5) other possible causes of encephalopathy or vasogenic oedema should be ruled out; the criteria for inclusion were similar to those of others before.32 As such, several atypical and rare variants (eg, ‘unilateral’, ‘central’ and ‘cerebellar’) have been identified that are reversible; thus, the awareness of the myriad imaging appearances of PRES is increasing.3 ,33 34
No guidelines exist to direct this assessment at present; therefore, clinical judgement is crucial. The symptoms and signs of PRES (eg, confusion, seizures, headache and visual symptoms) are non-specific and may be also seen in many other neurological disorders; however, seizure is the most common presenting clinical symptom.8 35 The symptoms and signs are non-specific in isolation, thus necessitating brain imaging with the primary intent to exclude alternative diagnoses. However, the diagnosis of PRES is not simply radiological; the clinical context and the judgement of the clinician are crucial to making the correct diagnosis. Studies on PRES have traditionally relied on the radiological presence of vasogenic oedema as a mandatory diagnostic criterion. Consequently, this clinical syndrome has inappropriately been labelled as a radiological diagnosis, with most case series selecting PRES cases with relatively favourable outcomes, although the resolution of MRI lesions is slower than clinical recovery. Consequently, our operational definition of the syndrome has defined the version of PRES that is heretofore described in the literature, while the clinical context and accurate clinical judgement are crucial to making the correct diagnosis.3 32 Hence, a combination of the clinical symptoms with imaging findings is essential in making the diagnosis of PRES.
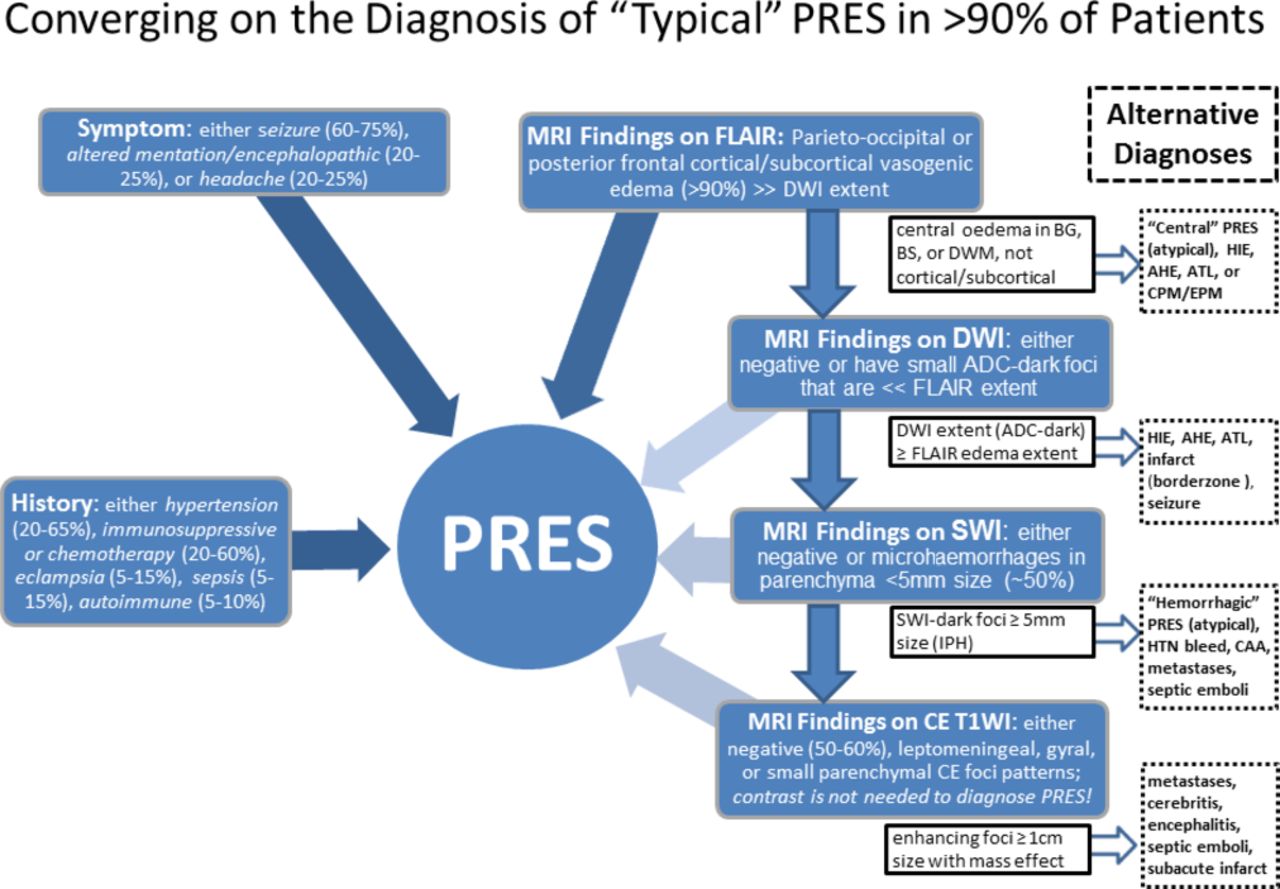
The diagnosis of PRES is typically a clinicoradiological one, which can be arrived at rather rapidly in most patients, versus a circuitous path in a small minority.3 ,37 The reasoning for this variability is perhaps the vast array of potential aetiologies and clinical symptoms presentations, when viewed in sum total. However, it may be fortunate that >90% of patients have typical radiological and clinical presentations.3 ,37 38 For example, over 95% of patients have a cortical–subcortical appearance of vasogenic oedema, regardless of the presence of smaller foci of cytotoxic oedema on DWI, contrast-enhancing foci or microhaemorrhages (MHs), and over 95% involve the parieto-occipital region (and high precentral/posterior frontal region) disproportionately to the remainder of the brain.3 37 38 Combined with this ‘typical’ radiological appearance of PRES, the clinical symptoms are mostly commonly seizures (60%–75%), and less commonly altered mentation and headaches (in 20%–25% each), which account for over 90% of symptomatology.3 ,37 38 Meanwhile, the aetiologies of PRES depend on the cohort, type of hospital and geography and are typically available within the clinical history on presentation; these are most often hypertension (20%–65%), immunosuppressive or chemotherapy medication (20%–60%), eclampsia (5%–15%), sepsis (5%–15%) or autoimmune disease (5%–10%), which together also account for over 90% of patients’ aetiologies of PRES. Thus, using a ‘90% rule’, a patient presenting with cortical–subcortical parietial–occipital–posterior frontal oedema, and having one of the above-mentioned common symptoms and aetiologies, is extremely likely to have PRES, regardless of findings on DWI, susceptibility weighted imaging (SWI) or postcontrast imaging. The consternation in diagnosis often arises in obtunded patients with frank encephalopathy (ie, not able to provide additional history) that exhibit atypical or severe appearances, whether ‘central’ PRES, frank >5 mm-sized haemorrhages or unilateral (‘tumefactive’) PRES.3 ,29 ,33 34 ,39 In this regard, we propose a preliminary diagnostic algorithm that combines clinical and radiological features for the vast majority of patients using a ‘90% rule’, which can in many cases be detected with a paucity of clinical data, whereas ‘atypical’ PRES can be a diagnostic dilemma that at times may necessitate a thorough review of past records and sequential imaging (figure 1). Notably, in this algorithm, hypoxic-ischaemic encephalopathy, border zone infarct, meningoencephalitis, acute toxic leukoencephalopathy, acute hepatic encephalopathy, cerebral amyloid angiopathy, central/extra pontine myelinolysis and lupus cerebritis are potential diagnostic considerations to name a few.3 ,6 ,40–42 Given the retrospective nature of nearly all larger PRES studies, such an algorithm needs to be confirmed prospectively but might serve as a starting point for future prospective studies.
{kind=link}
A radial convergence diagram demonstrating an algorithm to converge on the diagnosis of ‘typical PRES’ in over 90% of patients. Note ‘Alternative Diagnoses’ on the right side for each MRI appearance inflection point, which in some cases can be ‘atypical’ PRES (ie, occurs in <10% of PRES). ADC, apparent diffusion coefficient; AHE, acute hepatic encephalopathy; ATL, acute toxic leukoencephalopathy; CAA, cerebral amyloid angiopathy; CE, contrast enhancing; CPM/EPM, central pontine/extrapontine myelinolysis; DWI, diffusion-weighted imaging; HIE, hypoxic-ischaemic encephalopathy; HTN, hypertension; IPH, intraparenchymal haemorrhage; PRES, posterior reversible encephalopathy syndrome.; FLUID, fluid attenuated inversion recovery; BG, basal ganglia; SWI, susceptibility weighted imaging, BS,brainstem; DWM, deep white matter.
Neuroimaging is critical for prompt recognition of this potentially reversible entity, as well as in differentiation from other diseases, especially for patients in pregnancy and the puerperium.43 ,38 Since FLAIR improves the ability to diagnose and detect subcortical and cortical lesions in PRES as compared with conventional T2-weighted images, FLAIR is considered essential in patients with suspected PRES to allow more confident recognition of the often subtle imaging abnormalities.5 Additionally, DWI combined with ADC maps is quite sensitive and accurate for differentiating cytotoxic oedema from vasogenic oedema.28 29 ,32 In practice, ADC mapping may be helpful if the clinical diagnosis is unclear or difficult, particularly when hypoxic-ischaemic injury is a consideration.3 6 SWI may be of additional benefit, as it can depict either frank haemorrhage or even early MHs that may develop as a sequela of PRES; however, the clinical relevance of microbleeds in PRES has yet to be determined.44
Prognosis
PRES was initially described as a reversible benign entity and is increasingly recognised and favourably treated. Early data show that PRES has a good short-term and long-term prognosis.36 With the increased report of PRES cases with unfavourable outcome or prognosis, ‘malignant’, ‘severe’ or ‘fatal’ PRES or population in ‘critically ill’ or ‘critical care’ condition have been described in a number of literatures.45 46 Large series have enhanced our understanding of its clinical and radiological presentations, associated disorders and prognosis. At present, the data on the prognosis in patients with PRES from larger studies are still limited and the prediction of which remains controversial.47
The prognosis of PRES is mainly determined by the underlying condition, since most neurological symptoms are reversible in the majority of patients. Different causes or risk factors of PRES may share the similar clinical symptoms and prognosis. Recurrence is infrequent, even though trigger factors for PRES were repeatedly experienced by the patients.36 Hypertension should not be the decisive factor or prerequisite for the development of brain oedema in PRES even in brainstem dominant pattern, although which is more prone to occur in patients with hypertension.48 Nevertheless, appropriate reduction of blood pressure may prevent lesion progression from vasogenic oedema into cytotoxic oedema, infarction or even permanent neurological deficits.49 There is consensus regarding elimination of the aetiological factor in PRES secondary to cytotoxic medication; however, long-term management of immunosuppressants or chemotherapy remains a challenging issue that is usually decided on individual basis.50–52 The combination of multiple causes or risk factors is likely to have no effect on its clinical symptoms, while the number of which may make a difference on the recovery duration in patients with PRES. In most situations, patients with unfavourable outcomes are more frequently seen in state of neurotoxicity such as chemotherapy, sepsis and frequently have serious underlying medical conditions, such as neoplasm, autoimmune disease or infection/sepsis/shock. However, elimination of these neurotoxic states may be difficult in such challenging clinical settings.53 However, a delay in the elimination of the causative factor may also represent an important predictor of poor outcome, which might further explain the seemingly worse prognosis of these patients.54 Physicians should be alert of the potential aetiologies of PRES in order to reduce morbidity by providing rapid diagnosis and proper treatment.
However, since PRES is often accompanied by severe complications, neurological sequelae may persist in some patients. In a recent retrospective chart review, the authors found that pre-existing diabetes mellitus and corpus callosum involvement of PRES-associated lesions were strong predictors of poor outcome.55 Although the presence and degree of elevated blood pressure have been shown in many studies, these do not correlate with either the clinical outcome or MRI severity or grading of vasogenic oedema.3 ,7 ,10 ,56 Accordingly, Singer and colleagues have observed a complete resolution of neurological signs and symptoms in 84% of cancer patients with PRES, with the neuroimaging being reversible in 81%; notably, the mortality rate in that cohort was reported to be 19% but, none of the deaths were directly associated with PRES.57 58 Regarding death from PRES, permanent neurological deficits or even death have been occasionally reported in various subsets of populations with PRES.43 ,52 58 A series of recently published investigations reported PRES-specific mortality from 8% to 19%, as well as poor outcome in 26%–37%, respectively; much of the discrepancies in reported morbidity and mortality rates in the literature may be due to large differences in sizes of the included populations, the retrospective nature of most studies or the cohort makeup of aetiologies in each study (eg, in community populations where hypertension is most common vs immunosuppressed patients in tertiary care centres).52 53 59 For example, just as seizures are perhaps the most common initial presenting symptom, there is a concern that epilepsy may be a long-term sequela of PRES.60 In this regard, a recent retrospective study on 220 patients from Belgium found that symptoms of epileptic seizures, encephalopathy, visual disturbances, hypertension, renal failure and chemotherapy were the best clinical predictors of PRES, while headache, immune suppression and autoimmune disease were not useful for the clinical diagnosis of PRES.51 Interestingly, certain neurological sequelae, in particular epilepsy, motor deficits and mydriasis, may persist in individual cases and may require long-term treatment.7 35 60 This is in line with a retrospective study in 35 paediatric cases of PRES triggered by cancer treatment, which also reported a long-term requirement for anticonvulsive treatment due to persistent epilepsy in 19% of patients; other studies have found that persistent epilepsy occurred long-term after PRES in 2/75 (2.7%) and 4/102 (3.9%) patients.7 35
Regarding MRI severity, preliminary retrospective studies suggest that there may be a significant correlation with clinical outcome, but the need to identify comorbidities exists.3 6 10 56 For example, recent retrospective study of PRES including 103 patients reported significant differences between patients discharged home and those referred for rehabilitation or who died in hospital with respect to the following factors: severe oedema, aetiology, altered mental state at onset, altered coagulation and length of hospital stay >30 days in univariate analyses.50 Karia et al also found that while the MRI severity correlated with clinical outcomes in 135 patients, the presence or pattern of gadolinium-based contrast enhancement in PRES was not associated with any of the tested variables, such as age, sex or symptom.6 Thus, the severity of MRI lesions, including ADC values, may be an important parameter in determining long-term prognosis, but this needs to be evaluated prospectively. From these studies, it is justified to propose that the severity of oedema could be an important risk factor for poor prognosis, with cause and biochemical parameters of PRES potentially representing the other influential factors.
Regarding the clinical scoring of PRES, the modified Rankin scale(mRS) score is the most widely used outcome measure of the degree of disability or dependence in patients with stroke in general. Regarding PRES, the clinical outcome has been assessed as degree of disability or death by using mRS score in many articles, or alternatively a modified mRS-like scale specifically dedicated to PRES in others.7 Some investigators have used the mRS score as a prognostic index during the clinical follow-up of patients with acute illness at 1-month and 3-month intervals after discharge. Alternatively, the Glasgow Outcome Scale score on day 90 (67 days after onset of severe PRES) has also been adopted as a primary evaluation criterion by some researchers, which may better reflect both mortality and morbidity, especially in critically ill patients or fatal cases. A modified mRS-like scale dedicated to the clinical reversibility versus persistence of the presenting neurological symptom has also been proposed, which has preliminarily shown utility in reflecting the long-term outcomes in PRES and has been correlated with the MRI severity of oedema.7
PRES was also selected as a kind of acute toxic effect by Ponte di Legno toxicity working group in 14 consensus definitions for childhood acute lymphoblastic leukaemia treatment (ALLT) using the Delphi method over three face-to-face plenary meetings. Although PRES is a clinicoradiological entity that is frequently reported during the first months of ALLT, only one protocol addresses it in details, and seven do not address it at all. The protocols applying US National Cancer Institute about Common Terminology Criteria for Adverse Events grading used for any encephalopathy also are unavailable for PRES. Except for postponing intrathecal treatment until symptoms resolve, none of any modifications about antileukaemic treatment are recommended in any of the protocols. In the overall assessment of outcome of ALLT, these expert opinion-based definitions will allow reliable comparisons of frequencies and severities of acute toxic effects across treatment protocols, and facilitate international research on cause, guidelines for treatment adaptation, preventive strategies and development of consensus algorithms for reporting on ALLT.
So far, the factors such as serum markers or cerebral spinal fluid (CSF) findings of PRES have not been identified as useful in the risk stratification of patients nor as a measure of prognostic relevance. First, the elevation of lactate dehydrogenase (LDH) has been associated with a generalised state of endothelial activation in patients with PRES and is more frequently encountered in eclampsia or pre-eclampsia and cancer chemotherapy. Based on the similarities between such a provasoconstrictive milieu and our current understanding of the underlying pathophysiology, we propose that LDH may serve as a potentially sensitive biomarker of endothelial dysfunction in PRES patients in whom more specific imaging markers are not retrospectively available.32 Second, in clinical care elevated C reactive protein (CRP) as a key inflammatory marker has been reported to be consistently associated with death, poor clinical outcome and increased cardiovascular event risk in cerebrovascular diseases. Siebert et al reported altered mental state, subarachnoid haemorrhage as well as the higher levels of CRP and altered coagulation were more frequently seen in patients who died in hospital, suggesting prospective studies are warranted to establish predictors of fatality in such patients.52 CRP is an acute phase reactant in response to acute inflammatory stimuli and has been demonstrated to have direct effects on cerebral microvascular endothelial cells. However, elevated CRP levels might also affect or aggravate brain oedema with increased disruption of BBB due to inflammation-associated endothelial damage in PRES. This might also lead to more severe PRES symptoms that are associated with poor outcome. It is not clear whether PRES as a condition itself might influence the level of CRP. Further investigations, especially dedicated multicentre researches, are needed to explore the causal relationships between CRP levels, inflammation, BBB dysfunction and outcomes of PRES. Third, serum albumin is a main contributor to colloid osmotic pressure (COP), decrease of serum albumin levels would result in retention of intravascular fluid by reducing perfusion pressure. Vasogenic oedema can be aggravated by a marked decrease of COP. Pirker et al reported that vasogenic oedema in PRES was much more frequent in patients with decreased levels of serum albumin, whereas cytotoxic components occurred more frequently in patients with normal levels. Gao et al found that cytotoxic oedema or ischaemia was often seen in larger areas or to a higher extent of vasogenic oedema, which is probably related to local decreased perfusion and arteriolopathy.56 Both Gao and Pirker observed decreased serum albumin in up to 85% of PRES patients with miscellaneous aetiology. Serum albumin may be a potential contributor to the development of oedema in PRES, but it is not a decisive factor for oedema type. Last but not least, pathological changes in CSF are also non-specific in PRES. In CSF, elevated levels of albumin and an elevated CSF/serum albumin quotient as a manifestation of BBB disruption have been reported in a series of 87 patients, whereas pleocytosis was rare. This is in line with a retrospective review of 73 patients with PRES undergoing lumbar puncture. Mild albuminocytological dissociation was found in all patients with median protein levels of 58 mg/dL. However, until now no specific serum findings have been observed in patients with PRES. The role of clinical and biochemical parameters in predicting the prognosis of patients with PRES warrants further verification. Identifying the predictors of functional outcome for this clinical–radiological syndrome is still a huge challenge for us.
Future directions
Findings on cerebral perfusion in patients with PRES are conflicting, since both hyperperfusion and hypoperfusion have been reported in the literature as potential pathophysiological mechanisms for PRES. Designing a reliable animal model of the disorder would be a major step forward. The rat model of acute hypertensive state induced by continuous infusing of phenylephrine hydrochloride has been successfully developed by one of our study groups. The imaging distribution of vasogenic oedema can be detected in the rat model using 7.0T animal dedicated mircro-MRI. Meanwhile, our data suggested that cerebral vasogenic oedema, hyperperfusion and BBB leakage exist in acute hypertensive state, which support the hypothesis of autoregulatory dysfunction (unpublished data). Future imaging protocol should focus on angiographic imaging and perfusion imaging to characterise cerebral haemodynamics during PRES that may vary depending on aetiological aspects or disease severity. Furthermore, non-invasive continuous monitoring of the cerebrovascular autoregulation may aid in the optimal haemodynamic management and the definition of individual blood pressure targets maintaining a constant cerebral blood flow (CBF) within the limits of cerebral autoregulation.Functional MRI could also be of use in comparing between baseline and the onset of PRES in high-risk patients, which could help to shed light on both the causes of and sequelae of it. The clinical spectrum and pathophysiological changes underlying PRES continue to be redefined and should be the focus of prospective study. Pathophysiological studies are warranted to unravel the mechanisms leading to endothelial dysfunction and BBB hyperpermeability. Pathophysiological studies are scarce, and no randomised controlled trials on therapeutic interventions have been undertaken. Interventional trials would be necessary to confirm the value of controlling blood pressure and testing pathophysiologically guided therapies.
PRES generally has a favourable prognosis, but neurological sequelae and even fatalities can occur, particularly when the syndrome is complicated by intracranial haemorrhage or brain infarction. The disagreement between studies on whether the MRI severity correlates with clinical findings and the collective clinical experience clearly showing that PRES can cause permanent disability are some of the arguments that call for a new conceptual framing of this disorder.7 Prospective exploration is warranted to establish the imaging biomarker associated with unfavourable clinical outcomes of PRES. However, a substantial caveat is that the use of diagnostic criteria reliant on the presence of vasogenic oedema on brain imaging. Clinical-radiological reversibility might also have impeded the inclusion of atypical cases and erroneously formulated a limited version of the syndrome, which does not include the entire range of expected signs and symptoms. The establishment of the biomarker associated with unfavourable outcomes in PRES would be proven useful for clinicians of various disciplines involved in the care of patients with PRES patients.32 Currently, an international multicentre clinical trial is being implemented (Prognostic Observation of Posterior Reversible Encephalopathy Syndrome, NCT02665598) using unified inclusive diagnostic criteria, which will likely be of great value to explore its associations, atypical manifestations and prognosis.
Conclusion
In conclusion, a unified diagnostic algorithm should be sought to standardise the diagnosis of PRES and description of clinical outcomes, which will facilitate future research in exploring the role of neuroimaging in this disorder. No specific prognostic marker has been precisely identified, although there have been several preliminarily identified comorbidities and markers of outcomes. Typically, the prognosis of PRES is primarily determined by the underlying pathology, while outcome depends on the immediate removal or treatment of such. The roles of imaging findings, clinical symptoms and biochemical parameters in predicting prognosis of PRES certainly warrant further investigation, particularly prospectively.
References
Footnotes
BG and CL contributed equally.
Contributors BG and CL conceived the idea for the article and wrote the first draft. All authors revised the manuscript critically for important intellectual content and gave final approval of the version to be published. BG and CL contribute equally to the review and considered as the co-first author.
Funding BG reports research grant from National Natural Science Foundation of China (NSFC, Grant No. 81471645) and Shandong Provincial Key Research & Development Project (2015GSF118185).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note References 60 onwards can be found as an online supplementary reference file.
Correction notice Since this paper was first published online Shandong Provincial Key Research & Development Project has been added as a funder.