Article Text

Abstract
Aim: To explore attitudes to influenza immunisation and rates of uptake among staff working in acute hospitals in the UK.
Method: A cross-sectional survey of 11 670 healthcare workers in six UK hospitals was carried out using a postal questionnaire.
Results: Among 6302 responders (54% of those mailed), 19% had taken up influenza immunisation during winter 2002/3. Vaccination was well tolerated, with a low prevalence of side effects (13%) and associated time off work (2%). The majority of subjects who accepted vaccination (66%) were most strongly influenced by the personal benefits of protection against influenza. Prevention of sickness absence and protection of patients were the prime motivation for only 10% and 7% of subjects, respectively. Among 3967 who declined vaccination, the most common primary demotivators were concern about safety (31%) and efficacy (29%). 22% were most strongly deterred by lack of time to attend for vaccination. Free text answers indicated that 37% declined because of a perceived low ratio of personal benefits to adverse effects. Subjects said they would be persuaded to take up vaccination in future by easier access (36%), more information about personal benefit and risk (34%) and more information about effects on staff absence (24%).
Conclusions: These findings indicate that the uptake of influenza immunisation among UK healthcare workers remains low. There is some scope for increasing uptake by improving accessibility and encouragement from professional peers. However, the results suggest that perception of small personal benefit in relation to risk mitigates, importantly, against higher uptake of routine annual influenza vaccination. Thus, resource might better be allocated to ensuring efficient management in epidemic years. The effect of publicity about pandemic influenza on risk perception and vaccine uptake among healthcare workers during winter 2005/6 warrants further study.
- OHDs, occupational health departments
- PAMs, professions allied to medicine
- PR, prevalence ratio
Statistics from Altmetric.com
Since the late 1960s annual influenza immunisation has been recommended for people in the UK general population who are at high risk of serious illness from influenza. In 2000, UK national policy was extended to include those aged ⩾65 years,1 and since then vaccine uptake in vulnerable groups has been high.2 In 2000 the Chief Medical Officer also recommended that influenza vaccine should be offered annually to all healthcare workers, irrespective of age or personal medical indications. However, in contrast to the successful public health campaign, uptake among healthy National Health Service (NHS) employees has been low.3–7
If low vaccine acceptance among healthcare workers is to be addressed, it is important to understand the beliefs that influence uptake. However, most studies of influenza immunisation in UK healthcare workers pre-date the Chief Medical Officer’s guidance, or were undertaken soon after the change in policy. Since then, NHS occupational health departments (OHDs) have promoted influenza immunisation intensively, and it is possible that the barriers to uptake have changed. Moreover, most previous work on reasons for non-uptake is derived from small studies,4,6,7 which might be influenced by regional factors (eg, cultural influences on illness behaviour, the tendency to take sickness absence and the opinions of local professional peer leaders). Therefore, to guide national policy on influenza immunisation in healthcare workers, we undertook a large multicentre cross-sectional survey of attitudes in acute NHS hospitals.
METHOD
Through collaboration with the Association of NHS Occupational Physicians, six acute hospitals in the UK were recruited. These centres were selected because they had achieved good rates of uptake of influenza vaccine among staff in previous years, but were otherwise similar to other UK hospitals. We also ensured a wide geographical spread, including hospitals in England, Scotland and Northern Ireland.
Personnel records were used to identify all nurses working on acute medical care and elderly care wards, intensive care units and accident and emergency departments; all doctors; professions allied to medicine (PAMs) (radiographers, physiotherapists, occupational therapists and dieticians); laboratory technicians; porters. During 2003, 11 670 subjects were sent a postal questionnaire asking about current and previous uptake of influenza vaccination, reasons for uptake in those who received immunisation, and both barriers to uptake and inducements to accept vaccination in those who had declined. A single reminder was sent by internal post after 1 month. The study was approved by the Multi Centre Research Ethics Committee for Scotland and by local research ethics committees.
Data were analysed using STATA software, and log–logistic regression models (generalised linear models for the binomial family) were used to explore the relationships of various outcomes with beliefs about and experience of influenza immunisation according to personal characteristics. Associations were expressed as prevalence ratios (PRs) with 95% CI.
RESULTS
In all, 6302 replies were received from six centres, giving an overall response rate of 54% (range 44–65% by centre). Out of these, 83% of responders were aged between 25 and 54 years and 99% had worked in the healthcare industry for at least 1 year. The largest professional group was nurses (30%), followed by doctors (27%) and PAMs (26%).
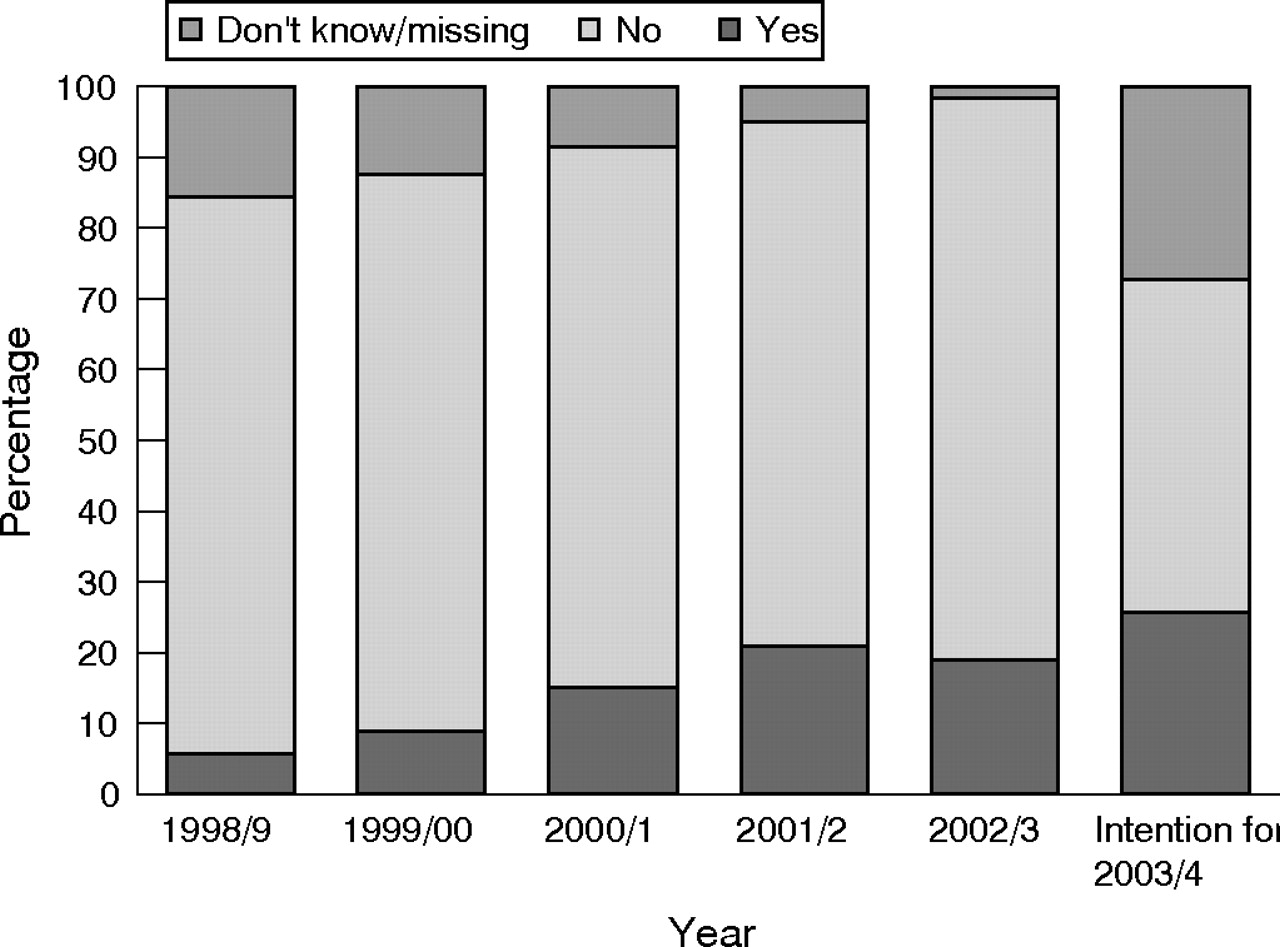
Figure 1 shows the uptake of influenza vaccination during 1998–2002 and the number who intended to accept vaccine during the forthcoming winter (2003/4). The annual uptake rate increased steadily from 6% in 1998/99 to 19% in 2002/3 and, by stated intention, would increase again during the 2003/4 influenza season. Among 6207 healthcare workers who reported their current (2002/3) immunisation status, uptake increased significantly with increasing age (PR 2.2 in the oldest compared with the youngest age category, 95% CI 1.8 to 2.8), and was significantly higher in current or ex-smokers than in those who had never smoked (PR 1.2, 95% CI 1.1 to 1.3). Clinical professionals (nurses, doctors and PAMs) were significantly less likely to be immunised than laboratory staff and others (PRs 0.8, 0.8 and 0.7, respectively). There was little variation by centre (range 15–22%), but one centre (centre 6) achieved a significantly lower uptake rate (15%).
{kind=link}
Vaccine uptake by year among 6302 healthcare workers.
Among 1203 healthcare workers who were immunised against influenza in 2002/03, 784 (70%) obtained their vaccine through an OHD and 237 (21%) through their general practitioner. Of those who were immunised, 155 (13%) reported side effects after vaccination, including 24 (2% of those immunised) who took time off the work because of their symptoms. Among 14 subjects who reported the duration of sickness absence associated with side effects, a total of 50 working days were lost.
Table 1 shows the relationship of reported side effects and time off work after immunisation with age, professional group and smoking history. Nurses were significantly more likely to report vaccine-related side effects than the other professional groups (PR 2 compared with laboratory staff and others, 95% CI 1.2 to 3.3). Doctors were less likely than others to take time off work because of vaccine-related symptoms, but this was not statistically significant (PR 0.6 compared with laboratory staff and others, 95% CI 0.1 to 3.2).
Association of reported vaccine-related side effects and consequent time off work with personal characteristics in 1203 immunised healthcare workers
Among 1156 healthcare workers who reported the single strongest influence on their decision to be immunised, the most common motivating factor was prevention of influenza infection (760, 66%). A further 193 (17%) were most strongly encouraged by advice from a doctor, 117 (10%) wanted to help colleagues by not being off work with influenza and 82 (7%) wanted to protect patients from influenza.
Among 3967 subjects who declined vaccination and reported the single most important influence, the most frequent primary demotivators were concerns about side effects (1211 (31%)) and a belief that the vaccine would not prevent influenza infection (1104 (28%)). A total of 875 (22%) cited lack of time to attend for vaccination.
Table 2 shows the primary reasons for refusing vaccine by professional groups. Nurses were significantly more likely to be dissuaded by concern about side effects (PR 1.2 compared with laboratory staff and others, 95% CI 1 to 1.4). Doctors were significantly more likely to be dissuaded by lack of time or limited knowledge about availability of the vaccine (PR 2.2).
Association between strongest reason for declining influenza vaccination and professional group
To explore the potential for response bias, the analyses shown in fig 1 and tables 1 and 2 were repeated for each individual centre. The pattern of results was not substantially different between the centres with the highest and lowest response rates.
Through a free text field, 1816 subjects provided additional reasons for refusing immunisation during 2002/3. Answers indicated that 341 (9% of all decliners) might be amenable to accepting influenza immunisation in the future, if given information about influenza vaccine and easier access. Conversely, answers given by 1475 (37% of all decliners) indicated that they were not likely to change their intention to refuse. Among these “resistant decliners”, the majority of responses suggested rationalisation of a low risk of infection and/or a low risk of serious clinical outcome against a significant risk of side effects and/or low vaccine efficacy. Concern about impaired efficacy from viral antigenic shift, was expressed by 76 (2% of all decliners). A further 104 (3% of all decliners) had fundamental objections to immunisation, and 62 (2% of all decliners) had long-term medical contraindications.
All subjects were asked about the factors that would persuade them to accept immunisation in future. Table 3 shows the frequency of those factors by professional groups. Protected time or easier access (36%) and more information about side effects (34%) were the most common factors. More information about the effect on winter workload or staff absence was an important influence for 24%. Doctors were significantly more likely to be encouraged by protected time or easier access (PR 1.4 compared with laboratory staff and others, 95% CI 1.2 to 1.6), and less likely to be persuaded by more information about side effects and efficacy. Nurses and PAMs were more likely to be persuaded by additional information about side effects (PR for nurses 1.2, 95% CI 1.1 to 1.4, PR for PAMs 1.2, 95% CI 1 to 1.3 compared with laboratory staff and others) and the potential effect on winter workload or staff absence (PRs 1.5 and 1.3, respectively). Among all responders, 1445 (23%) declined immunisation in 2002/3 but indicated that easier access would encourage uptake. Subjects reported additional persuasive factors, including the occurrence of an influenza epidemic, advancing age, increased susceptibility to influenza or risk of a serious outcome, experiencing an episode of influenza, more convincing evidence of benefit and improved efficacy or safety. Only 23 subjects (0.4% of all responders) said they would be persuaded by more evidence that immunising the staff would protect their patients.
Factors that would encourage uptake of influenza vaccine by professional group
DISCUSSION
As far as we know, this is the largest published survey of attitudes to influenza immunisation among healthcare workers in the UK. We have confirmed reports from smaller studies that the uptake is poor,3–7 particularly in comparison with health professionals in the USA.8,9,10,11 However, this survey postdated a change in policy to immunise healthy NHS staff, and explored residual barriers to uptake after intensive promotion by NHS occupational health departments.
A particular strength of the study was the inclusion of subjects from a broad geographical area. The main limitation was a relatively low response rate (54%). It is possible that people who accepted immunisation were more likely to reply, leading us to overestimate uptake. Conversely, if those who objected strongly were more likely to reply, we may have overestimated the incidence of side effects and negative beliefs. However, biased response is unlikely to have had a systematic effect on the associations noted. The pattern of results by centre indicated that response bias is unlikely to have affected our conclusions greatly.
We showed a steady increase in the uptake of influenza vaccine by healthcare and support workers during 1998–2002. This might be due, in part, to limited recall for previous years, as indicated by an increasing proportion of missing responses with increasing duration of recall (fig 1). However, this is unlikely to explain all the increase noted. Participating hospitals had a previous history of good uptake. They promoted influenza immunisation heavily, and had special arrangements to improve accessibility, including delivery on wards and sessions for night staff. Moreover, promotion campaigns emphasised excellent efficacy and safety. The high proportion of subjects who were vaccinated by OHDs (70%) is encouraging. However, the modest improvement in uptake to 19% in 2002/3 is disappointing. This is in keeping with the small improvement in national uptake in hospitals from 14% in 2002/3 to 16% in 2004/5 (Department of Health, UK, unpublished).
The incidence of vaccine-related side effects (13%) is comparable to previous studies in adults.12 It is interesting that doctors were much less likely to take time off work owing to side effects of immunisation, despite having an incidence of symptoms similar to other professional groups.
Among healthcare workers who declined immunisation, most (60%) reported fear of side effects or lack of conviction about efficacy as the primary reasons. In contrast, only 22% said that lack of time was the greatest barrier. The overwhelming impression from our qualitative data is that health professionals perceive a very low risk from influenza in non-epidemic years. This is in keeping with a smaller study in which good perceived health was found to be a barrier to influenza immunisation among healthcare workers.13 Despite having been informed about the low risk of side effects, many were discouraged by reports of adverse reactions from colleagues or relatives. Thus, in the context of routine annual immunisation, the balance of two small risks (serious infection vs adverse effects) has been rationalised in favour of non-uptake.
The primary justification for immunising healthcare workers is for their own protection against influenza infection. However, simply providing more information about individual risks and benefits is not likely to change their behaviour, because their risk assessment is based on reasonable evidence. On the other hand, healthcare workers seemed receptive to reconsider if the balance of personal risks and benefit changed substantially. Anecdotally, uptake among NHS staff during winter 2005/6 improved owing to the threat of pandemic influenza. This warrants further study. However, even if confirmed, this effect on attitudes is likely to decay with time if a pandemic does not occur. Consequently, resources may be better spent on developing systems for managing an epidemic, rather than on further intensive measures to improve annual immunisation.
A second justification for immunisation against seasonal influenza is the protection of patients. Despite evidence that immunising the staff reduces mortality in older patients,14 only 7% of healthcare workers in this study cited protection of patients as the primary motivator for immunisation. More research to enhance the existing evidence of benefit to patients might enable greater emphasis in justifying immunisation to healthy staff.
A third justification for annual influenza immunisation in healthcare workers is the prevention of sickness absence and associated service pressure in winter. Only 10% of our sample cited this as the primary motivator for immunisation. In view of the paucity of evidence in this area, it is important to continue to study the role of immunisation in managing sickness absence as part of winter pressure planning in the NHS.
In conclusion, personal protection was the primary motivator for taking up influenza vaccine among this group of UK healthcare workers, and a low perceived risk of illness and/or fear of side effects were the main deterrents. Further efforts to give information about personal risks and benefits of immunisation and to enhance accessibility are likely to have only a modest effect on annual uptake. Therefore, it might be more cost effective to focus on alternative strategies during epidemic years. More information is needed about the effect of pandemic threat on uptake, the effect of influenza immunisation on sickness absence in healthcare staff, the protection of patients and the overall cost effectiveness of routine annual immunisation of healthy clinical professionals as part of winter pressure planning.
Main messages
-
Despite promotion campaigns and improved accessibility to influenza immunisation (including delivery at ward level), annual uptake rates in acute sector healthcare workers remain low.
-
The incidence of side effects from immunisation (13%) and associated absence from work (2%) was low.
-
Key health professionals perceive a very low risk of infection with influenza, and feel that this does not outweigh the low risk of vaccine-related side effects.
-
Healthcare workers said that they would be persuaded to accept vaccination in the event of epidemic activity or a favourable change in the balance of personal benefit and risk in favour of vaccination.
Policy implications
-
There is scope for further improvement in education about personal benefit/risk and access to influenza vaccine for key healthcare workers. However, these strategies are unlikely to increase annual uptake rates above approximately 40%, and are likely to be costly.
-
The protection of patients and reduction of staff absence might persuade National Health Service staff to accept vaccination. However, more information on these aspects and on the overall cost–benefit of promoting routine annual influenza vaccination in healthy clinical professionals is needed.
-
Until more evidence is available, resources may be better spent on preparing for an epidemic or pandemic, than on further intensifying attempts to increase annual vaccine uptake.
Acknowledgments
We thank Vanessa Cox who managed the computing and Dr C Joseph at the Health Protection Agency Centre for Infections who supplied unpublished statistics with permission from the Department of Health.
REFERENCES
Footnotes
-
Published Online First 19 December 2006
-
Funding: This study was funded by the Department of Health.
-
Competing interests: None.