Article Text

Abstract
Colorectal cancer screening has vast potential. Beyond considerations for cost and diagnostic accuracy, the effectiveness of any colorectal screening strategy will be dependent on the degree of patient acceptance. Magnetic resonance (MR) colonography has been shown to be accurate regarding the detection of clinically relevant colonic polyps exceeding 10 mm in size, with reported sensitivity and specificity values exceeding 95%. To further increase patient acceptance, strategies for fecal tagging have recently been developed. By modulating the signal of fecal material to be identical to the signal characteristics of the enema applied to distend the colon, fecal tagging in conjunction with MR colonography obviates the need for bowel cleansing. The review will describe the techniques underlying MR colonography and describe early clinical experience with fecal tagging techniques.
- colorectal cancer
- screening
- MR colonography
- CRC, colorectal cancer
- MR, magnetic resonance
- CT, computed tomography
- VC, virtual colonography
- MRC, magnetic resonance colonography
Statistics from Altmetric.com
- CRC, colorectal cancer
- MR, magnetic resonance
- CT, computed tomography
- VC, virtual colonography
- MRC, magnetic resonance colonography
Colorectal cancer (CRC) remains the second leading cause of cancer death for both women and men1 with more than 130 000 newly diagnosed cases and 50 000 deaths each year in the United States alone.2 Most colon cancers develop from non-malignant colonic adenomas or polyps over a comparatively long time period ranging between 24–60 months.3 Cancer screening programmes targeting precancerous colonic polyps with subsequent endoscopic polypectomy are suitable to reduce colorectal cancer mortality by more than 80%.4 Thus, colorectal screening for polyps may be considered one of the most promising preventive measures in medicine.
Despite the availability of screening options, CRC remains a considerable cause of morbidity and mortality. This fact underscores the lack of a suitable modality for colorectal polyp screening resulting in poor patient participation.5,6 Any successful strategy must overcome poor patient acceptance, which is marring current techniques.
While there are various psychological factors inhibiting the acceptance of cancer screening programmes in general, efforts targeting the colon have been particularly problematical. Non-invasive cancer screening programmes such as the testing of occult fecal blood are associated with both low sensitivity and specificity values regarding the detection of precancerous as well as cancerous lesions.7 Endoscopic screening programmes are characterised by high sensitivity and specificity but lack sufficient acceptance by the target populations.8,9 Among the causes, one issue relates to the discomfort associated with the preparation for the procedure (that is, bowel cleansing and dietary restriction in preparation for colonoscopy). In addition, anticipation of a endoscopic study of the colon is frequently associated with unpleasant expectations focusing on procedure related pain and discomfort as well as the risk of complications such as perforations. These expectations result in poor patient participation even if colonoscopy is offered free of charge.10 Other causes inhibiting the use of colonoscopy for widespread screening relate to the inability to examine the entire colon in a considerable number of patients.11,12 This has motivated the development and evaluation of alternative strategies to assess the colon, including virtual colonography.
VIRTUAL COLONOGRAPHY
Virtual colonography (VC) is based on either magnetic resonance (MR) or computed tomography (CT) 3D datasets. Based on cross sectional images, this type of examination offers several advantages over conventional colonoscopy, the most significant of which relates to the lack of procedural pain and discomfort. Angtuaco et al demonstrated that more than 60% of potential patients preferred VC over conventional colonoscopy when both methods were offered.13 Non-invasiveness and no need for sedation were the main reasons for the preference of virtual colonography.
In contrast with a conventional colonoscopic analysis, VC is not limited to endoscopic viewing. Rather the 3D datasets can be scrolled in a traditional 2D mode on a workstation in any desired plane. This type of multiplanar reformation analysis depicts the colonic lumen as well as the colonic wall relative to the surrounding abdominal morphology. Lesions can thus be located more accurately. Even in the presence of stenotic tumours, the entire colon can be assessed, which often is not possible in conventional endoscopy. A further advantage of VC based on either CT or MR datasets relates to the simultaneous assessment of other abdominal organs. In the case of patients with suspected colorectal tumour, imaging of the liver must be considered a welcome addition.
Despite the availability of multiple studies reporting its high diagnostic accuracy,14,15 the future of CT colonography as a screening method for colorectal cancer is uncertain: patients are exposed to considerable doses of ionising radiation.16,17 This is compounded by the fact that two datasets, one in the prone and a second one in the supine position, need to be collected. As a screening examination of the colon should be repeated at regular intervals (every three to five years), the radiation issue may even evolve into a public health concern. Therefore, it seems reasonable to focus on MRI for colorectal screening strategies. The technique is not associated with any exposure to ionising radiation and lacks any other known harmful side effects. Furthermore, contrast agents applied in conjunction with MRI examinations are characterised by a more favourable safety profile than CT contrast agents as they lack any nephrotoxicity and are associated with far fewer anaphylactic reactions.18,19
VIRTUAL MR COLONOGRAPHY: TECHNIQUE
Currently two techniques are being evaluated for MR colonography (MRC). Based on the signal within the colonic lumen, they can be differentiated as “bright lumen” and “dark lumen” MRC.
Bright lumen MRC
Similar to contrast enhanced 3D MR angiography, MRC is based on the principles of ultra fast, T1 weighted 3D GRE acquisitions collected within the confines of a single breath hold.20 This requires the use of an MR scanner equipped with high performance gradients. To permit homogenous signal transmission and reception over the entire colon with high CNR values, a combination of phased array surface coils should be used. The size of the coil must permit coverage of the entire colon.
As colonic lesions often cannot be differentiated from stool, the patient has to undergo bowel cleansing in a manner similar to that required for conventional colonoscopy. Before the examination the patient should be screened for contraindications to MRI such as severe claustrophobia, presence of metallic implants in critical regions such as the eyes, spinal chord or brain, or cardiac pacemakers. The presence of hip prostheses, which normally is not regarded a contraindication to MRI, impedes a complete analysis of the rectum and sigmoid colon. Therefore, patients with hip prosthesis should also not be examined by MRC.
After placement of a rectal enema tube, the colon is filled with the patient in the prone position using 1000 to 2000 ml of a water based enema, spiked with paramagnetic contrast (1:100). The enema is administered using 100 cm–150 cm of hydrostatic pressure (fig 1). To reduce bowel motion and alleviate colonic spasm, the use of intravenously administered spasmolytic agents (for example, scopolamine or glucagon) before and during the bowel filling is helpful. In contrast with conventional colonoscopy sedative or analgesic agents do not have to be applied. To ensure safe and optimal bowel filling and distension, the filling process is monitored with a non-slice select 2D acquisition, collecting one image every three seconds (fig 2). Once the enema has reached the caecum, a 3D dataset of the abdomen encompassing the entire colon is collected. To compensate for the presence of residual air exhibiting “filling defects” similar to polyps within the colonic lumen, 3D datasets are collected in both the prone and supine patient positions. Hereafter the enema bag is placed on the floor for facilitated emptying of the colon and the patient is removed from the scanner.

For filling of the colon with 1000–2000 ml of a water based enema, the patient is placed in the prone position. The enema is administered using 100–150 cm of hydrostatic pressure.
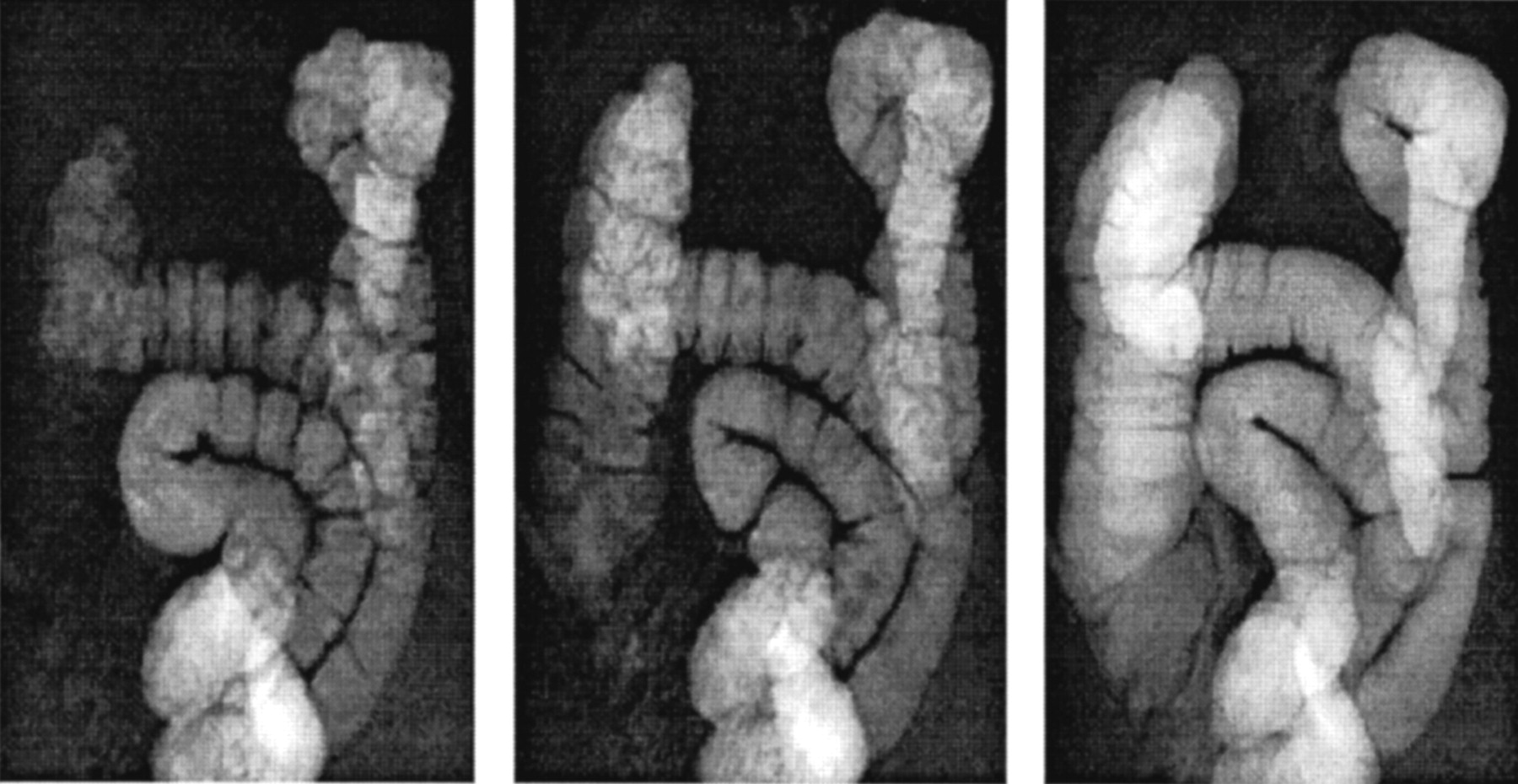
Colonic filling is monitored with a non-slice select 2D acquisition collecting one image every three seconds. The last image on the right demonstrates that enema has reached the caecum.
The acquired 3D MR datasets consist of coronal sections, ranging in thickness between 1.5 mm and 2 mm. The sequence is based on the use of short repetition (TR 1.6 ms–3.8 ms) and echo times (0.6 ms–1.6 ms). The achievable minimum TR should be shorter than 5 ms; otherwise, the acquisition of a 3D dataset cannot be collected within the confines of a single breathhold. In conjunction with a field of view of 400×400 mm and an imaging matrix of 460×512, the spatial resolution includes an interpolated voxel size of about 1 mm×1 mm×1.6 mm.
On the 3D GRE datasets only the colonic lumen containing the enema is bright whereas all other tissues remain low in signal intensity. The resulting contrast between the colonic lumen and surrounding structures is the basis for subsequent virtual colonographic viewing (fig 3). The MRC protocol can be further amplified by the acquisition of 2D gradient echo datasets after the intravenous application of a gadolinium containing contrast compound. This permits a more comprehensive assessment of parenchymal abdominal organs and increases the ability to detect hepatic metastases.
The high contrast between the contrast filled colonic lumen and surrounding structures (on the left) is the basis for subsequent virtual colonic viewing (on the right).
Bright lumen MRC can be completed within 20 minutes, including the time for patient positioning, image planning, and data acquisition. The 3D datasets are subsequently processed using commercially available software and hardware. A complete analysis of an MRC examination still requires 15 minutes of interactive image viewing on a high performance work station. In a first step MRC images should be interpreted in the multiplanar reformation mode scrolling through the prone 3D dataset in all three orthogonal planes. In regions containing larger pockets of residual air, the assessment needs to be supplemented by views of the supine dataset. In a second step the data should be assessed based on virtual endoscopic renderings displaying the inside of the colonic lumen. A virtual endoscopic fly through allows the observer to concentrate on the colon facilitating the depiction of small structures protruding into the colonic lumen. Furthermore, the three dimensional depth perception permits the assessment of haustral fold morphology, thereby increasing the observer’s ability to distinguish polyps from haustra. To assure complete visualisation of both sides of haustral folds, the virtual fly through should be performed in an antegrade as well as retrograde direction (fig 4).

A single coronal section of a 3D dataset demonstrates a small filling defect in the sigmoid colon. Virtual endoscopic viewing confirms the presence of a polyp.
Dark lumen MRC
The detection of colorectal lesions with “bright lumen” MRC relies on the visualisation of filling defects. Differential considerations for such a filling defect beyond polyps include air bubbles as well as residual fecal material. To permit differentiation datasets are collected in both the prone and supine patient position: air and fecal material move, while polyps remain stationary. While effective in most instances, the technique can introduce errors. Thus, polyps with a long stalk may move sufficiently to impress as a moving air bubble or more probably residual stool, while stool adherent to the colonic wall may not move at all and thus falsely impress as a polyp. In addition to obviating the need for a second, time consuming 3D data acquisition “dark lumen” MRC facilitates the identification of polyps.
“Dark lumen” MRC focuses on the colonic wall. It is based on contrast generated between a brightly enhancing colonic wall and a homogeneously dark colonic lumen.21 The technique differs from “bright lumen” MRC in the following manner:
-
Instead of agadolinium containing enema only tap water is rectally applied rendering low signal on heavily T1 weighted 3D GRE acquisitions.
-
The colonic filling process is monitored with a fluoroscopic T2w sequence, rather than a T1w sequence.
-
To obtain a bright colonic wall paramagnetic contrast is applied intravenously. 3D datasets are collected before the application and after a 75 second delay.
-
As residual air exhibits no signal in the colonic lumen, the examination needs to be performed only in the prone patient position.
Compared with “bright lumen” MRC that has been extensively evaluated in the past, “dark lumen” MRC harbours considerable advantages including reduced examination and post-processing times, as only one 3D dataset needs to be collected. Furthermore, the “dark lumen” technique copes with the problem of residual stool in a simple manner: if the lesion enhances it is a polyp, if it does not enhance it represents stool (figs 5, 6). Suspicious appearing lesions are analysed by comparing signal intensities on the pre-contrast and post-contrast images. If analysis were limited to the post-contrast dataset, bright stool could be misinterpreted as a polyp. Comparison with the pre-contrast images records the lack of contrast enhancement, which assures the correct diagnosis.

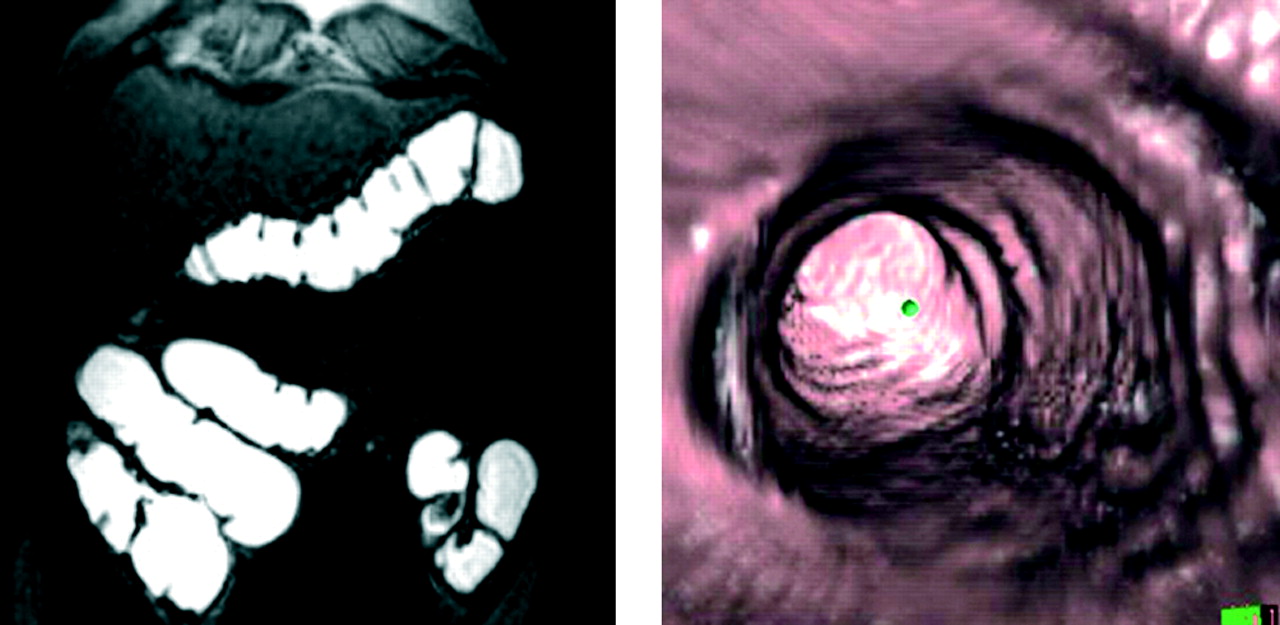
Dark lumen MR colonography focuses on the colonic wall. After filling of the colonic lumen with warm tap water a 3D gradient echo dataset is collected over 20 seconds in apnea 75 seconds after the intravenous administration of paramagnetic contrast. At this time there is avid enhancement of the colonic wall as well as of colorectal masses arising from it. In this case a large 15 mm polyp is identified arising from the sigmoid colon. The polyp is seen to clearly on the coronal source image (top left), the sagittal reformation (top right), the axial reformation (bottom left), and the virtual endoscopic view (bottom right).

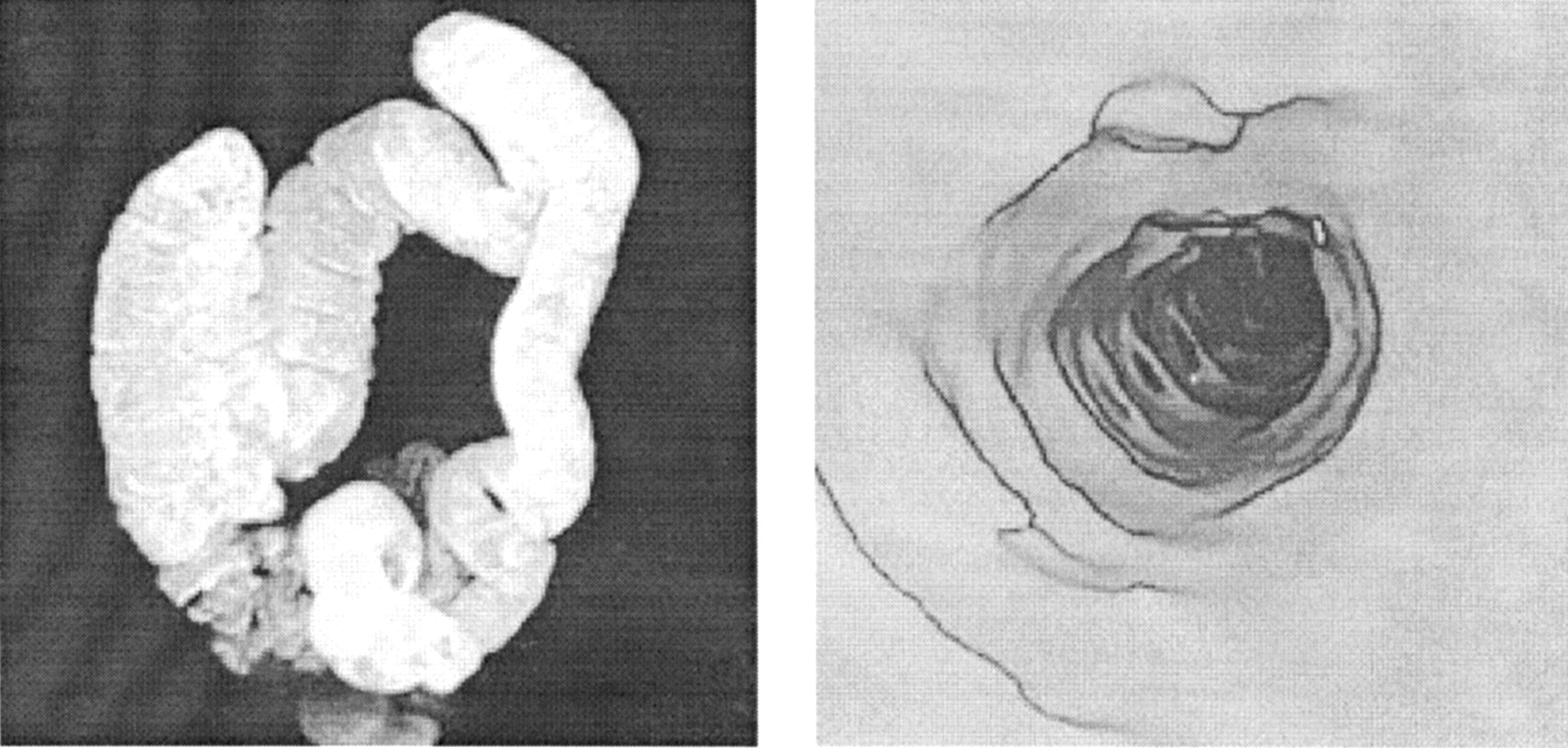
Single coronal section of a dark lumen MR colonography 3D dataset, which was acquired over 20 seconds in apnea 75 seconds after the intravenous administration of paramagnetic contrast. A small 7 mm polyp is identified arising from the sigmoid colon. The polyp is seen clearly on the coronal source image (left) as well as on the virtual endoscopic view (right).
Enhancement of colorectal masses following the intravenous administration of contrast has been reported in conjunction with MRC22 and CT colonography.23 The use of intravenously administered contrast material significantly improves reader confidence in the assessment of bowel wall conspicuity and the ability to depict medium sized polyps in suboptimally prepared colons. The enhancement observed within polyps exceeds the increase determined within the colonic wall. This may aid in differentiating even very small polyps from thickened haustral folds.
A further advantage of “dark lumen” MRC relates to the fact that it permits direct analysis of the bowel wall. This might facilitate the evaluation of inflammatory changes in patients with inflammatory bowel disease (fig 7). Increased contrast uptake and bowel wall thickening, as recorded on contrast enhanced T1 weighted images has already been shown to correlate well with the degree of inflammation in the small bowel.24 Hence, the “dark lumen” approach may indeed amplify the list of indications for MRC in the future to also encompass inflammatory bowel disease.
Maximum intensity projection (MIP) display of a 3D MR colonography dataset collected after gadolinium based fecal tagging (left). After filling the colon with a gadolinium containing enema, the tagged stool is no longer seen because its signal intensity is similar to that of the applied rectal gadolinium/water enema. The intraluminal signal intensity is sufficiently homogeneous to permit virtual colonoscopic viewing (right).
Finally, the intravenous application of paramagnetic contrast permits a more comprehensive assessment of parenchymal abdominal organs contained within the field of view. By combining pre-contrast and post-contrast T1 weighted imaging, the liver can be accurately evaluated regarding the presence and type of concomitant disease. Dark lumen MRC also offers new perspectives regarding optimisation of bowel distension. Although the administration of water as a rectal enema does not adversely affect patient comfort in most cases, a modified strategy could be based on the application of gases like carbon dioxide.25 The gas is signalless and would thus easily permit delineation of the contrast enhanced colonic wall and masses.
DIAGNOSTIC PERFORMANCE OF MRC
The diagnostic performance of bright lumen MRC was assessed in several studies26,27 using conventional colonoscopy as the standard of reference. While most mass lesions smaller than 5 mm in size were missed,13 almost all lesions exceeding 10 mm were correctly identified (table 1). In a study by Pappalardo et al28 MRC even detected a higher total number of polyps exceeding 10 mm in size than conventional colonoscopy. MRC identified additional polyps in regions of the colon not reached by colonoscopy.
Direct observational data on growth rates indicated that polyps smaller than 10 mm remain stable over three years and are not prone to malignant degeneration.29 Hence, bright lumen MRC may be considered almost as reliable as conventional colonoscopy regarding the assessment of colonic lesions at risk for malignant degeneration. Nevertheless, attempts are under way to increase the spatial resolution of the underlying 3D datasets and thereby improve the diagnostic accuracy of MRC for lesions ranging between 5 mm and 10 mm in size. Technique refinements include the use of even shorter repetition times in conjunction with zero filling routines and the implementation of parallel imaging routines.30
Fecal tagging
MRC still requires bowel cleansing in a manner similar to conventional colonoscopy. As 75% of patients undergoing bowel preparation complain about symptoms ranging from “feeling unwell” to “inability to sleep”,31 patient acceptance is affected negatively. To assure high patient acceptance of MRC, bowel cleansing needs to be eliminated. This can be accomplished with fecal tagging—a concept based on modulating the signal intensity of fecal material by adding contrast compounds to regular meals.
Fitting the two approaches to MRC (bright lumen and dark lumen), there are also two theoretical approaches to fecal tagging. Its principle was demonstrated on the basis of a bright rectal enema distending the colonic lumen containing brightly tagged stool in conjunction with bright lumen MRC.32 By adding a T1 shortening Gd based MR contrast agent to regular meals before the MR examination, harmonisation of signal properties between fecal material and the Gd based enema was achieved. The oral administration of a paramagnetic MR contrast agent (Gd-DOTA) has been shown to be safe. The combination of fecal tagging with a paramagnetic contrast agent and colonic filling results in a homogenous signal distribution throughout the colon (fig 7). In these examinations virtual MRC permits an unobstructed view through the colon because the tagged stool is virtually indistinguishable from the administered enema. Although encouraging results concerning acceptance and image interpretation were obtained, the clinical implementation of bright lumen fecal tagging was hindered by the high cost of the Gd based paramagnetic contrast agent.
A second strategy for fecal tagging is based on rendering the colonic lumen dark.33 For fecal tagging, a highly concentrated, barium sulphate containing contrast agent (Micropaque; Guerbet, Sulzbach, Germany; 1 g barium sulphate/ml) is administered in a volume of 200 ml with each of four main meals beginning 36 hours before MRC. Patients are instructed to avoid the intake of all fibre rich foodstuff and nourishments with high concentration of manganese such as chocolate or fruits during this period, as manganese leads to an increased signal intensity in T1w sequences. “Barium based” fecal tagging is combined with dark lumen MRC: the colon is distended with a rectally applied water enema and paramagnetic contrast is administered intravenously to render the colonic wall and adherent colorectal mass lesions bright.
Barium sulphate is a well known diagnostic contrast agent, still in common use as an oral agent for oesophageal, gastric, and small bowel radiography. Compared with Gd based contrast compounds, it is far less costly and characterised by an even better safety profile. Anaphylactoid reactions or other adverse side effects are virtually unknown. The agent is not absorbed and mixes well with stool. Thus, barium includes all characteristics as an ideal oral tagging agent for MRC.
The barium based approach to fecal tagging has been successfully assessed.33 The signal reducing effects upon stool has been documented in volunteer studies. By ingesting barium before the MR examination, stool is rendered virtually indistinguishable from the administered water enema on heavily T1w 3D GRE images (fig 8). The MR examination without prior ingestion of barium reveals signal rich stool that cannot readily be differentiated from the brightly enhancing colonic wall (fig 8).

Images of two volunteers undergoing MR colonography based on the rectal administration of a barium enema in conjunction with the intravenous administration of paramagnetic contrast. One volunteer did (right) and one volunteer did not (left) ingest barium for fecal tagging. In both cases the colonic wall is bright after the after application of paramagnetic contrast. Fecal material in the volunteer who had not received barium for fecal tagging is bright and can thus not be differentiated from the brightly enhancing wall. The presence of colonic polyps cannot be excluded with certainty. The colonic lumen of the volunteer who had ingested the barium tagging agent on the other hand is homogenously dark, thereby permitting a full analysis of the colon.
Recently, the barium based fecal tagging concept has been successfully evaluated in a pilot patient study. Fecal tagged MRC detected all polyps larger than 8 mm in a population of 24 patients with known or suspected colorectal tumours.34 Overall sensitivity of MRC amounted to 89.3% for the detection of colorectal masses, and specificity was 100%. Colorectal cancers (fig 9) and polyps (fig 10) were readily identified as such.

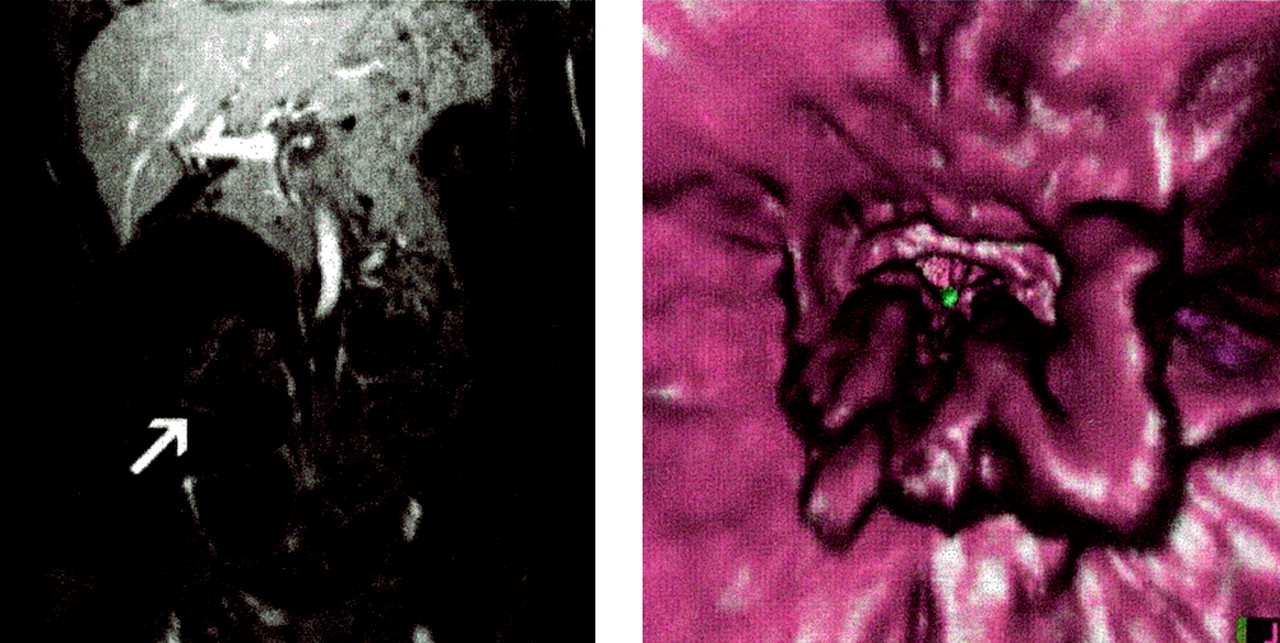
Coronal source image (right) and virtual endoscopic rendering thereof (left) of 3D gradient echo dataset collected after the administration of a barium enema and the intravenous injection of gadobenate dimeglumine. A contrast enhancing colonic carcinoma close to the right colonic flexure is identified both on the coronal section as well as on the virtual endoscopic view.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Axial reformatted image (right) and virtual endoscopic rendering (left) of a 3D gradient echo dataset collected after the administration of a barium enema and the intravenous injection of gadobenate dimeglumine. A contrast enhancing 10 mm polyp is identified in the sigmoid colon on both the single axial section as well as the virtual endoscopic rendering.
Although further work is required to confirm these excellent results, it seems that barium tagged MRC has vast potential to emerge as the examination strategy of choice for the early detection of polyps in asymtomatic subjects. The technique seems to combine excellent diagnostic accuracy with high patient acceptance based on a painless examination and no need for colonic cleansing.