Article Text

Abstract
Background Patients with high Rockall scores have increased risk of ulcer rebleeding after 3-day esomeprazole infusions.
Objective To investigate whether double oral esomeprazole given after a 3-day esomeprazole infusion decreases ulcer rebleeding for patients with high Rockall scores.
Design We prospectively enrolled 293 patients with peptic ulcer bleeding who had achieved endoscopic haemostasis. After a 3-day esomeprazole infusion, patients with Rockall scores ≥6 were randomised into the oral double-dose group (n=93) or the oral standard-dose group (n=94) to receive 11 days of oral esomeprazole 40 mg twice daily or once daily, respectively. The patients with Rockall scores <6 served as controls (n=89); they received 11 days of oral esomeprazole 40 mg once daily. Thereafter, all patients received oral esomeprazole 40 mg once daily for two more weeks until the end of the 28-day study period. The primary end point was peptic ulcer rebleeding.
Results Among patients with Rockall scores ≥6, the oral double-dose group had a higher cumulative rebleeding-free proportion than the oral standard-dose group (p=0.02, log-rank test). The proportion of patients free from recurrent bleeding during the 4th–28th day in the oral double-dose group remained lower than that of the group with Rockall scores <6 (p=0.03, log-rank test). Among patients with Rockall scores ≥6, the rebleeding rate was lower in the oral double-dose group than in the oral standard-dose group (4th–28th day: 10.8% vs 28.7%, p=0.002).
Conclusions Double oral esomeprazole at 40 mg twice daily after esomeprazole infusion reduced recurrent peptic ulcer bleeding in high-risk patients with Rockall scores ≥6.
Trial registration number NCT01591083.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
-
A high Rockall score indicates an increased risk of recurrent peptic ulcer bleeding.
-
Recurrent peptic ulcer bleeding remains common in patients with comorbidities despite 3-day proton pump inhibitor infusion but may be reduced by prolonging the duration of the infusion.
-
The standard oral proton pump inhibitor given once daily may be unable to control acid secretion over a 24 h period.
What are the new findings?
-
The rebleeding risk between the 4th and 28th day in patients with Rockall scores ≥6 was reduced when patients received a double oral esomeprazole dose as 40 mg twice daily after 3 days of esomeprazole infusion.
-
Among patients with peptic ulcer bleeding and major indications of recent haemorrhage, the length of hospitalisation and number of units of blood transfused were lower in those with Rockall scores <6 than in those with Rockall scores ≥6.
How might it impact on clinical practice in the foreseeable future?
-
The study confirms that the Rockall score is a good risk predictor of peptic ulcer rebleeding and guides the indication of oral double-dose proton pump inhibitors after infusion to reduce peptic ulcer rebleeding in high-risk patients.
Introduction
Peptic ulcer bleeding is a common and deadly disease and rebleeding is an independent risk factor leading to death.1–4 Rockall et al validated a risk score to evaluate the severity and outcome of peptic ulcer bleeding; they suggested that patients with Rockall scores ≥6 have higher recurrent ulcer bleeding and mortality rates than patients with scores <6.5–8 The appearance of stigmata of recent haemorrhage indicates possible recurrence of peptic ulcer bleeding, for which the likelihood decreases over the course of 3–6 days.9–11 Thus, rebleeding commonly develops within 3 days of the initial bleeding episode,12–14 and intravenous infusion with a proton pump inhibitor is therefore regularly scheduled for 3 days to improve rebleeding control. In addition to the endoscopic evidence illustrating the stigmata of recent haemorrhage, patients with comorbidities have a higher risk of rebleeding.3 ,15–21 Furthermore, recurrent episodes of bleeding can occur up to 14 days after the first bleeding episode in patients with such comorbid conditions.18–21 Several studies have shown limited effectiveness for 3-day proton pump inhibitor infusion followed by a standard oral, once-daily dose for control of rebleeding in patients with comorbidities.8 ,17 ,18 This lack of control might be due to incomplete suppression of gastric acid secretion for 24 h by the oral proton pump inhibitor when taken once daily during this critical post-haemorrhage period.22 ,23
Several studies have shown that increasing the dose of oral proton pump inhibitors is as effective as intravenous therapy in raising the intragastric pH to reduce rebleeding.24–27 Thus, it is clinically relevant to determine the effect of higher doses of oral proton pump inhibitors to prevent rebleeding,28 especially in high-risk patients, such as those with comorbidities or high Rockall scores.
We investigated the effectiveness of a double dose of esomeprazole 40 mg twice daily in reducing the recurrence of peptic ulcer bleeding after 3 days of intravenous esomeprazole infusion in high-risk patients. We also evaluated the usefulness of the Rockall score as a predictor of the risk of peptic ulcer rebleeding.
Patients and methods
Study design
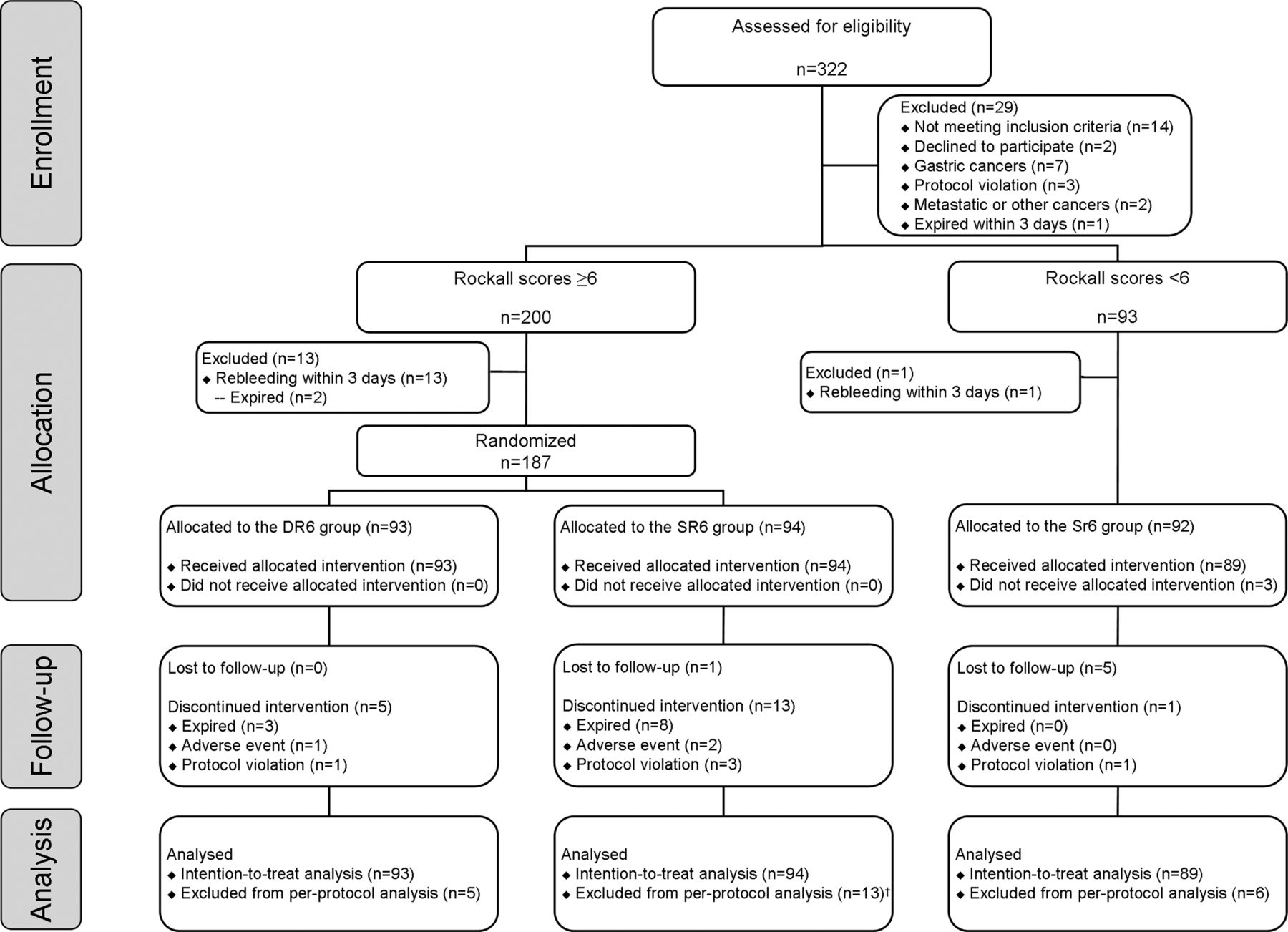
This study was conducted at the inpatient wards of National Cheng Kung University Hospital, a tertiary healthcare centre in Tainan, Taiwan. The research and ethics committee of the hospital approved the study design (trial registration identifier: NCT01591083, ClincalTrials.gov) and all participants gave written informed consent before enrolment. A schematic flow chart of the study protocol is shown in figure 1. The recommendations of the CONSORT statement for the quality of reports of a prospective, parallel-group, randomised trial were followed in this study.

The schematic flow chart of the study design. †One patient died because of recurrent bleeding, thus the patient was not excluded from the per-protocol analysis.
Eligible participants included patients aged ≥18 years who had undergone gastroscopy for melena, haematochezia or haematemesis due to bleeding peptic ulcers with major stigmata of recent haemorrhage. The major stigmata of recent haemorrhage were classified as Forrest class Ia, Ib, IIa and IIb.29 All the stigmata given one or a combination of endoscopic therapies, including local injection of diluted epinephrine 1:10 000, bipolar heated probe, argon plasma coagulation, band ligation or haemoclip therapy. Patients who were treated by local injection of diluted epinephrine only, at their first endoscopy underwent a second endoscopy 2 or 3 days later to confirm that the stigmata of recent haemorrhage had resolved or to perform dual gastroscopic therapy; otherwise, patients were not enrolled.
Patients were excluded if they had tumour bleeding or ulcer bleeding due to the presence of a Dieulafoy lesion or mechanical factors (ie, gastrostomy tube induction), warfarin use, proton pump inhibitor use within 1 week before enrolment, failure to establish haemostasis under gastroscopy, hypersensitivity to esomeprazole or any component of the formulation or had previously participated in the study. Because of concern for patient safety with certain drug–drug interactions, the protocol was amended in accordance with the US Food and Drug Administration and patients who took clopidogrel have been excluded since October 2012.30
Each enrolled patient received an 80 mg loading dose of intravenous esomeprazole (Nexium, AstraZeneca AB, Södertälje, Sweden) immediately after achieving haemostasis by gastroscopy. Patients then received a 3-day continuous high-dose (8 mg/h) esomeprazole infusion.31 After gastroscopy to confirm enrolment eligibility, all patients were assessed using the Rockall risk scoring system.5 ,6 Patients with Rockall scores ≥6 who did not have rebleeding within 72 h were randomised into the oral double-dose (DR6) group or the oral standard-dose (SR6) group following simple randomisation procedures with a 1:1 allocation ratio according to a random-number table. The allocation sequence of the random-number table was concealed until the researchers had randomised the patients. Those patients with Rockall scores <6 were enrolled as a parallel non-randomised reference group—the Sr6 group. Patients in the DR6 and SR6 groups received 40 mg oral esomeprazole twice daily or once daily for 11 days, respectively. Patients in the Sr6 group who did not have rebleeding within 72 h, were given oral esomeprazole 40 mg once daily for 11 days. Two further weeks of oral esomeprazole 40 mg once daily were given to all patients until the end of the 28-day study period. One investigator generated the random allocation sequence and enrolled the participants and a different investigator assigned participants to interventions. The endoscopists and staff who checked haemoglobin levels, haemodynamic status, melena, haematochezia or the aspirates through a nasogastric tube were blinded to the study group allocation.
All enrolled patients were included in the intention-to-treat (ITT) analysis, but patients who were lost to follow-up, discontinued intervention because of adverse events, had a protocol violation or died were excluded from the per-protocol (PP) analysis of the primary end point. For patients who received antiplatelet therapy for prophylaxis of established cardiovascular or cerebrovascular diseases, the treatment was discontinued for 3 days after gastroscopy. The antiplatelet therapy was resumed with clopidogrel 75 mg/day or aspirin 100 mg/day on the 4th day. After the 28-day follow-up, patients with Helicobacter pylori infection were given triple therapy, including 500 mg clarithromycin, 1 g amoxicillin and 40 mg esomeprazole twice daily for 1 week.32 ,33 This regimen was designed to prevent bias from the different proton pump inhibitor dosages resulting in differences in rebleeding rates. Ulcer size was estimated with biopsy forceps, with fully opened cups being 6 mm in diameter (FB-25K-1, Olympus, Tokyo, Japan).
The range of comorbidities evaluated by the Rockall scores included disseminated malignant diseases, liver disease (liver cirrhosis, Child–Pugh A, B or C), renal disease (end-stage renal disease, chronic kidney disease or acute kidney injury with estimated glomerular filtration rates <30 mL/min (a score of 3 for comorbidity) or between 30 mL/min and 60 mL/min (a score of 2 for comorbidity)) and heart disease (congestive heart failure, New York Heart Association Function I to IV or coronary artery disease). Other serious comorbidities included lung disease (chronic obstructive pulmonary disease, pulmonary tuberculosis, pneumonia or empyema), rheumatoid arthritis, sepsis, new-onset cerebrovascular accident or recent history of any major surgery (on the thorax, abdomen, central nervous system, long bones or spinal bones) requiring general anaesthesia within 14 days before bleeding.3 ,5 ,34
Outcome measures
All patients were monitored for 28 days after gastroscopy. The primary end point was the recurrence of bleeding from a peptic ulcer during the study period. Recurrent bleeding was defined as (1) continuous melena, haematochezia or the presence of recurrent bloody aspirates through a nasogastric tube and (2) relapse of haemodynamic instability, including systolic blood pressure <90 mm Hg, heart rate >120 bpm or a drop in haemoglobin concentration of >20 g/L. Haemoglobin levels were checked on days 0, 3 and 14. For each patient with either suspected or active rebleeding, gastroscopy was performed to confirm any blood or coffee-ground-like materials in the stomach, or the persistence of stigmata indicating recent haemorrhage. The gastroscopy also determined whether the source of rebleeding was a peptic ulcer or some other non-ulcer bleeding source, such as varices.
The secondary measurements included (1) major adverse events requiring transarterial embolisation or emergency surgery; (2) length of hospitalisation for or after the first bleeding episode and after peptic ulcer rebleeding; (3) number of units of blood transfused during the 28-day period after admission to the emergency room or after the presence of gastrointestinal bleeding signs during admission; (4) all-cause mortality, which was defined as any cause of death after gastroscopy during the 28-day study period, including death in hospital or after discharge from hospital. Recurrent bleeding-related mortality was defined as patient deaths due to (1) uncontrolled bleeding; (2) death within 48 h after endoscopy, transarterial embolisation for bleeding vessels or surgery for uncontrolled bleeding or (3) complications of these treatments.35
Statistical analysis
The estimated rebleeding rate between the 4th and 28th day in patients of the SR6 group was about 35% based on previous studies.8 ,18 ,20 ,21 We wanted to be able to detect a reduction by 50% in the incidence of rebleeding in the DR6 group compared with the SR6 group. With a two-sided α value of 0.05 and power of 80% (β=0.20), the total number of patients required was 185. The study was closed when the DR6 group and the SR6 group reached at least 93 patients, respectively. The estimated incidence of rebleeding during the first 72 h after esomeprazole infusion was 6–8%,31 ,36 thus, 200 patients with Rockall scores ≥6 were needed in the study. Two interim analyses of efficacy were performed when 50% and 80% of patients had been enrolled. We set up a statistical boundary and stopped if the p value of the primary end point was <0.01. Finally, we used a nominal 0.05 rate of the p value. Data related to baseline characteristics and end points were evaluated using the Student t test, Pearson's χ2 test or Fisher's exact test and the Mann–Whitney U test. In the survival analysis, the log-rank test was used to compare the Kaplan–Meier curves among the three study groups. All tests were two-tailed and p values <0.05 indicated significant differences.
Results
Demographic features and patient follow-up
Between August 2011 and July 2013, 322 patients with peptic ulcer bleeding were consecutively assessed for eligibility to take part in the study (figure 1). Twenty-nine patients were excluded: 14 did not meet the inclusion criteria, two declined to participate, seven had gastric cancer bleeding, three had protocol violations, two had duodenal metastatic cancer or neuroendocrine tumour bleeding and one died within 3 days. Among the 200 patients with Rockall scores ≥6, 13 had rebleeding within 3 days. The remaining 187 patients were randomised into either the DR6 group (n=93) or the SR6 group (n=94). Among patients with Rockall scores <6, one patient had rebleeding within 3 days and three patients did not receive the allocated intervention. Finally, 89 patients with Rockall scores <6 were recruited as the Sr6 group.
There were significant differences in the mean age, ulcer size and haemoglobin levels, the proportion of patients with shock on arrival, ulcer location, American Society of Anaesthesiologists (ASA) physical status classification, H pylori infection, antiplatelet agent use, prolonged prothrombin time (PT) ≥4 s and initial albumin <30 g/L between patients with Rockall scores <6 and those with Rockall scores ≥6 (p<0.05, table 1). Additionally, more patients with Rockall scores <6 received gastroscopic combination therapies at the first endoscopy than those with Rockall scores ≥6 (83.9% vs 73.5%, p=0.03). Only 4.3% (4/93) patients with Rockall scores <6 received an epinephrine injection only at the first endoscopy, and none needed further gastroscopic therapy at the second endoscopy. Twenty-nine patients with Rockall scores ≥6 who received an epinephrine injection only at the first endoscopy underwent a second endoscopy within 3 days, which showed that 20.7% (6/29) were in need of further gastroscopic combination therapies to achieve good haemostasis (table 1). The average epinephrine dose was 10 mL (range 8–15 mL) of diluted epinephrine 1:10 000.
Comparison of baseline characteristics of patients with Rockall scores ≥6 and those with Rockall scores <6
A higher recurrent bleeding rate within 72 h in patients with Rockall scores ≥6
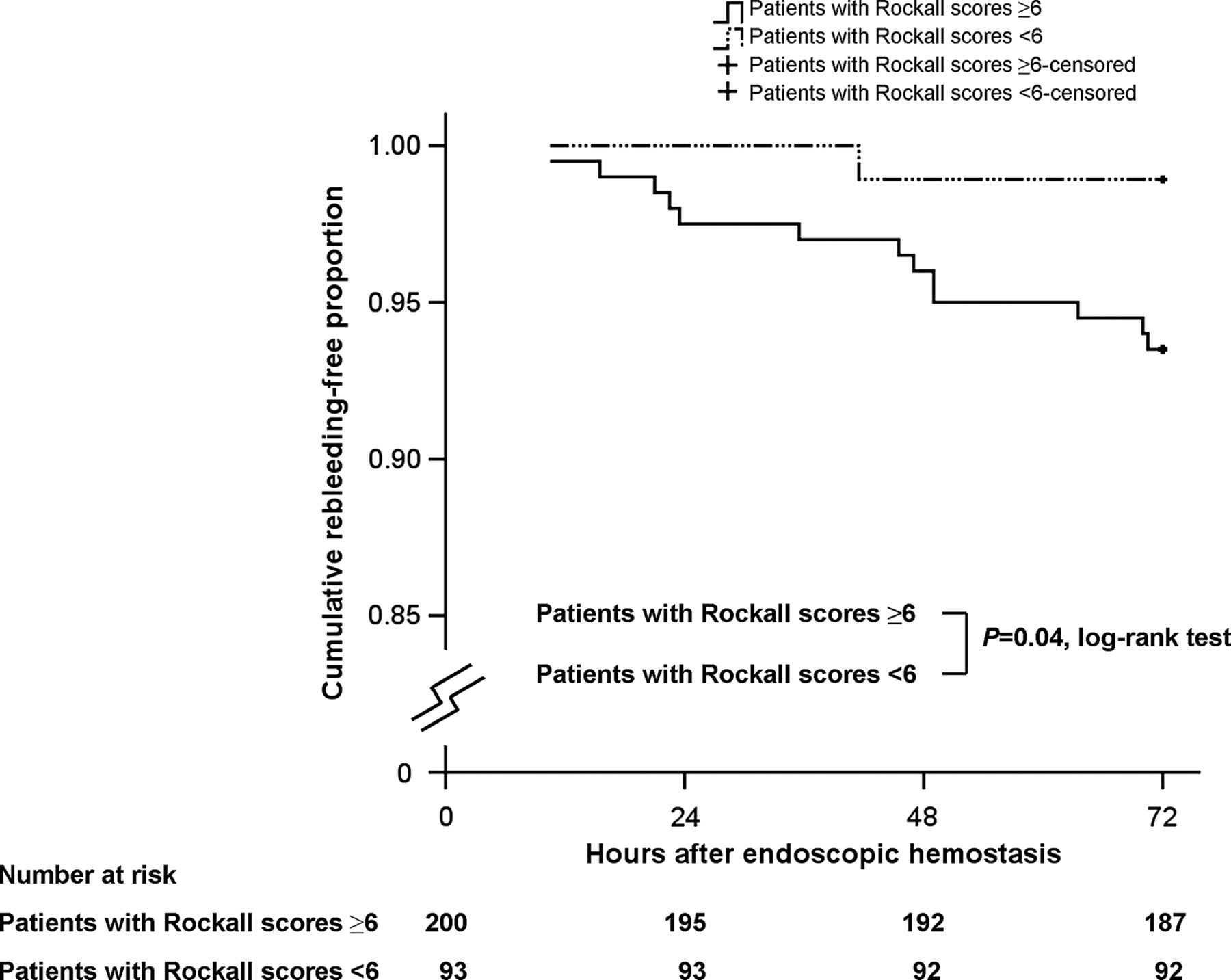
Fourteen patients had rebleeding within 72 h, including 13 with Rockall scores ≥6 and one with Rockall score <6. The follow-up endoscopy showed Forrest class Ib in seven patients, IIa in three patients, IIb in three patients and IIc in one patient. Twelve of the 14 patients received gastroscopic therapies; the remaining two patients had abundant blood clots which would interfere with the endoscopic visualisation. The rebleeding rate during the 3-day esomeprazole infusion was higher in patients with Rockall scores ≥6 than in those with Rockall scores <6 (6.5% (13/200) versus 1.1% (1/93), relative risk (95% CI), 6.05 (0.80 to 45.53), p=0.04). Figure 2 shows that the proportion of patients free from rebleeding during the first 72 h was lower in patients with Rockall scores ≥6 than in those with Rockall scores <6 (p=0.04).

The Kaplan–Meier curves show that the cumulative recurrent bleeding-free proportion during the 3-day esomeprazole infusion after endoscopic haemostasis was lower in patients with Rockall scores ≥6 than in patients with Rockall scores <6 (p=0.04, log-rank test).
Similar baseline characteristics between the DR6 and SR6 group
There were no differences in the demographic, clinical or endoscopic features, Forrest classification, gastroscopic therapy and the Rockall scores between the DR6 and SR6 groups (p>0.05, table 2). Moreover, there was no difference in the proportion of patients who received gastroscopic combination therapies (78.5% vs 69.1%, p=0.25), or an epinephrine injection only at the first endoscopy, between these groups (12.9% vs 14.9%, p=0.69).
Comparison of baseline characteristics of patients in the DR6 and SR6 groups
Six patients were lost to follow-up (one in the SR6 group and five in the Sr6 group). The adverse events were self-limited in three patients (one in the DR6 group with itchy skin and two in the SR6 group with itchy skin and mild abdominal pain). Protocol violations were reported for five patients (two in the SR6 group received prolonged intravenous esomeprazole infusion because of the clinical need for nothing by mouth, three patients were changed to take other proton pump inhibitors because of patients’ wishes) and were excluded from the PP analysis of the primary end point.
An oral double-dose of esomeprazole improves the recurrent bleeding rates between the 4th and 28th day in patients with Rockall scores ≥6
Nineteen patients had rebleeding between the 4th and 28th day, including five in the DR6 group (follow-up endoscopy showed one patient each with Forrest class Ia, Ib and IIb, respectively, and two patients with class IIc) and 14 patients in the SR6 group (class Ia in three patients, Ib in four patients, IIa in five patients, IIb in one patient and IIc in one patient). Sixteen of 19 patients needed gastroscopic therapies.
In table 3, the cumulative rebleeding rates were lower in the DR6 group than in the SR6 group either by ITT analysis (4th–14th day: 9.7% vs 23.4%; p=0.01; 4th–28th day: 10.8% vs 28.7%; p=0.002) or by PP analysis (4th–14th day: 5.6% vs 15.3%, p=0.04; 4th–28th day: 5.7% vs 17.3%, p=0.02). Additionally, the cumulative rebleeding rates were lower in the Sr6 group than in the SR6 group either by ITT analysis (4th–14th day: 4.5% vs 23.4%, p<0.001; 4th–28th day: 6.7% vs 28.7%, p<0.001) or by PP analysis (4th–14th day: 0% vs 15.3%, p<0.001; 4th–28th day: 0% vs 17.3%, p<0.001). Also in table 3, the adjusted relative risks for Forrest classification showed that the rebleeding risks were lower in the DR6 group than in the SR6 group by ITT analysis (4th–14th day: 0.41 (95% CI 0.18 to 0.93), p=0.025; 4th–28th day: 0.45 (95% CI 0.22 to 0.92), p=0.024). Additionally, the adjusted relative risks for Forrest classification showed that the rebleeding risks were higher in the SR6 group than in the Sr6 group by ITT analysis (4th–14th day: 8.25 (95% CI 1.97 to 34.54), p<0.001; 4th–28th day: 4.81 (95% CI 1.72 to 13.47), p=0.001).
Cumulative recurrent bleeding rates between the 4th and 14th day and between the 4th and 28th day by intention-to-treat and per-protocol analyses
The rebleeding rates were not significantly different between the DR6 and Sr6 groups by ITT analysis (4th–14th day: 9.7% vs 4.5%, p=0.18; 4th–28th day: 10.8% vs 6.7%, p=0.34). However, the rebleeding rates were marginally higher in the DR6 group than in the Sr6 group by PP analysis (4th–14th day: 5.6% vs 0%; 4th–28th day: 5.7% vs 0%, both p=0.06).
In figure 3, the Kaplan–Meier curves show that the proportion of patients free from rebleeding during the 4th–28th day was higher in the DR6 group than in the SR6 group (p=0.02, log-rank test). The proportion of patients free from rebleeding during the 4th–28th day remained higher in the Sr6 group than the other two groups (p<0.05, log-rank test).

{kind=link}
{kind=link}
{kind=link}
The Kaplan–Meier curves show that the cumulative recurrent bleeding-free proportion from the 4th to the 28th day after endoscopic haemostasis was higher in the DR6 group than in the SR6 group (p=0.02, log-rank test) and higher in the Sr6 group than in either the DR6 or the SR6 group (p=0.03 and p<0.001, log-rank test, respectively). DR6, oral double-dose group with Rockall scores ≥6; SR6, oral standard-dose group with Rockall scores ≥6; Sr6, oral standard-dose group with Rockall scores <6.
Differences in the secondary end points among study groups
Table 4 shows that the length of hospitalisation and the number of units of blood transfused were lower in the Sr6 group than in both DR6 and SR6 groups (p<0.001). Thirteen patients died, including three in the DR6 group (owing to sudden cardiac death, pneumonia with respiratory failure and rectal cancer with multiple metastases, respectively); eight patients died in the SR6 group (owing to uncontrolled recurrent bleeding, sudden cardiac death, pancreatic cancer in terminal status, lung cancer with sepsis, multiple lung metastases, septic shock and pneumonia (two patients), respectively) and two patients with Rockall scores ≥6 with recurrent bleeding died within 72 h (owing to uncontrolled peptic ulcer bleeding and perirenal abscess with respiratory failure, respectively). Therefore, all-cause mortality rates were lower in the Sr6 group than in the SR6 group (0% vs 8.5%, p<0.01). Moreover, all-cause mortality rates were also lower, but not significantly, in the DR6 group than in the SR6 group (3.2% vs 8.5%, p=0.13).
Analysis of the secondary outcomes
Discussion
This study demonstrated that the recurrence of peptic ulcer bleeding is higher in patients with Rockall scores ≥6 than in those with Rockall scores <6 during 3-day intravenous high-dose esomeprazole infusion after endoscopic haemostasis. Moreover, the study showed that double oral esomeprazole 40 mg twice daily after 3 days of esomeprazole infusion reduced recurrent bleeding for patients with Rockall scores ≥6 between the 4th and 28th day.
Endoscopic treatment plus a 3-day intravenous proton pump inhibitor infusion is the standard protocol for treatment of peptic ulcer bleeding.28 However, there were insufficient data to validate the efficacy of such standard treatment in high-risk patients, such as those with Rockall scores ≥6.7 ,8 The results show that the rebleeding rate during the first 72 h was higher in patients with Rockall scores ≥6 than those with scores <6 (6.5% vs 1.1%, p=0.04). Our results suggest that Rockall scores serve as a prognostic scoring system,5 ,6 and also as predictors of peptic ulcer rebleeding during 3-day proton pump inhibitor infusion. Non-steroidal anti-inflammatory drug non-H pylori ulcers have increased in recent decades. Patients with these ulcers are often older and sicker with higher risks of rebleeding and mortality.37 Improvements in healthcare are needed owing to ageing of populations worldwide, and the Rockall scoring system is important for the study of peptic ulcer bleeding.
Sung et al31 showed that high-dose intravenous esomeprazole, followed by oral esomeprazole once daily, significantly reduced the rebleeding rate of peptic ulcer diseases to close to 7.7%. Nevertheless, most of their patients were not in a high-risk group with Rockall scores ≥6. The mean age, the proportion of patients with ASA classification and shock were similar in the study of Sung et al and in our Sr6 group. Thus, the rebleeding rates (7.7% vs 6.7%) and the mortality rates (0.8% vs 0%) were similar in Sung's study and our Sr6 group. However, the mean age, the proportion of patients with ASA classification III and IV and shock were higher in our SR6 group than in Sung's study, and the rebleeding rate (28.7%) and the mortality rate (8.5%) were higher in our SR6 group than in their study. One recent study disclosed that patients with peptic ulcer bleeding and ASA classification III and IV have 3.32- and 7.24-fold risks of mortality,4 which may explain why our SR6 group had a high mortality rate. Based on an oral double-dose design (DR6 group), a comparatively low rebleeding rate of 10.8% by ITT analysis and mortality rate of 3.2% was found for patients with Rockall scores ≥6 (table 3).
Proton pump inhibitors provide the most potent acid suppression available, but a single, daily oral dose is often unable to suppress acid secretion over 24 h.38 ,39 With once-daily dosing, proton pump inhibitors inhibit only 70% of active pumps at steady state.40 ,41 For patients taking oral omeprazole 40 mg once daily, even doubling the dose might not keep the intragastric pH at ≥4.0 during the night time, because of diurnal rhythm.22 ,23 ,42 ,43 With a double-dose regimen, the dose given twice daily extends the mean residence time enabling them to inhibit restored pumps after initial proton pump inhibitor inactivation.44 ,45 Pharmacokinetic data show that oral twice-daily esomeprazole 40 mg provides greater acid suppression than oral 40 mg once-daily dosing.46 Therefore, we studied the oral double-dose regimen without monitoring the pH.
Responsiveness to proton pump inhibitors is variable. The Asian population has a smaller parietal mass and higher prevalence of a poor metaboliser of cytochrome P450, the CYP2C19 allele, than the Caucasian population.47 ,48 So as our study was conducted in an Asian population it is reasonable to expect a favourable outcome. Nevertheless, the oral twice-daily design of proton pump inhibitor use can decrease the variability among the different metabolisers of cytochrome P-450, the CYP2C19 allele.49 Therefore, our results suggest that use of oral double-dose esomeprazole is rational for high-risk patients generally. However, studies in different races, especially from Western countries, where populations have larger parietal cell mass and higher prevalence of extensive metabolisers of cytochrome P450, CYP2C19, are awaited.
For patients with comorbidities, prolonged omeprazole infusion of up to 7 days reduces recurrent ulcer bleeding.50 Nonetheless, it is time consuming and costly to extend hospitalisation for 7 days. Thus, we conducted a prospective randomised study of patients with high Rockall scores to determine the effectiveness of oral double-dose esomeprazole 40 mg given twice daily. The regimen reduced rebleeding and shortened the hospital stay to only 6 days.
Fewer patients with Rockall scores ≥6 received gastroscopic combination therapies at the first endoscopy than those with Rockall scores <6 (73.5% vs 83.9%, p=0.03). A possible reason might be that this study was carried out in a ‘real-world’ situation to deal with patients’ unstable haemodynamics (p=0.008), and the time available for gastroscopic combination therapies was limited. However, our study design, which used a second endoscopy routinely within the first 3 days to examine patients who had been treated by an epinephrine injection only, might have compensated for this limitation. Based on such a design, there should be no significant bias from the interference of gastroscopic therapy with outcomes of the study groups receiving different oral esomeprazole doses.
The study had some limitations. It excluded clopidogrel users, because our design, in which oral esomeprazole doses were doubled, raised concerns about increasing the risk of cardiovascular events. The scale of the study was limited, showing a trend towards decreased mortality when an oral double-dose of esomeprazole was used, as compared with the oral standard-dose, among patients with Rockall scores ≥6 (3.2% vs 8.5%, p=0.13). The mortality rate in our oral double-dose group was similar to, and even lower, than the 4.2% reported by Lau et al,36 whose study was not restricted to patients with Rockall scores ≥6. A future large-scale study would be useful to validate the potential for decreasing mortality by use of oral double-dose esomeprazole. Our study was limited to a non-blinded design, which might have had some bias on outcome measures. However, the criteria for rebleeding in our study were defined and measured as objectively as possible to decrease bias.
The rebleeding rates by both ITT and PP analyses were not significantly different between the DR6 and Sr6 groups. The marginally higher rates of rebleeding in the DR6 group suggested that more aggressive oral proton pump inhibitor use in such high-risk patients may be needed to achieve rebleeding control as well as in low-risk patients.
In conclusion oral twice-daily esomeprazole after 3-day intravenous esomeprazole infusion reduced the rebleeding rates of peptic ulcers in patients with Rockall scores ≥6. The study confirmed that Rockall scores may be used as risk predictors of peptic ulcer recurrent bleeding.
References
Footnotes
-
Contributors H-CC and B-SS conceived and designed the study. H-CC generated the random allocation sequence and enrolled participants and C-TW assigned participants to interventions. H-CC, W-LC, W-CC and W-YC followed up the patients in clinics and acquired data. H-CC analysed and interpreted all data and drafted the article. B-SS revised the article and gave final approval of the version to be published.
-
Funding This study was funded in part by research grants from the National Science Council of Taiwan (NSC 100-2314-B-006-026-MY3) and the National Cheng Kung University Hospital in Tainan, Taiwan (NCKUH-10104002).
-
Competing interests None.
-
Ethics approval Institutional review board, National Cheng Kung University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.