Article Text

Abstract
Functional heartburn is a common disorder and appears to be composed of several distinct subgroups. Identifying the different subgroups based on clinical history only is not achievable at present. The mechanisms responsible for pain, clinical characteristics, and the optimal therapeutic approach remain poorly understood. Response to potent antireflux treatment is relatively limited. Current and future treatment strategies for functional heartburn patients who have failed standard dose proton pump inhibitors (PPIs) include increased PPI dose in some, as well as addition of pain modulators in others.
- gastro-oesophageal reflux disease
- functional heartburn
- non-erosive reflux disease
- proton pump inhibitors
- GORD, gastro-oesophageal reflux disease
- NERD, non-erosive reflux disease
- PPI, proton pump inhibitor
- TLOSR, transient lower oesophageal sphincter relaxation
- PET, positron emission tomography
- FMRI, functional magnetic resonance imaging
Statistics from Altmetric.com
- gastro-oesophageal reflux disease
- functional heartburn
- non-erosive reflux disease
- proton pump inhibitors
- GORD, gastro-oesophageal reflux disease
- NERD, non-erosive reflux disease
- PPI, proton pump inhibitor
- TLOSR, transient lower oesophageal sphincter relaxation
- PET, positron emission tomography
- FMRI, functional magnetic resonance imaging
SUMMARY
Despite significant advances in our knowledge of the mechanisms leading to gastro-oesophageal reflux, our understanding of the factors responsible for the symptoms associated with gastro-oesophageal reflux disease (GORD) remains limited. Subjects with non-erosive reflux disease (NERD) account for up to 70% of GORD patients in the community and serve as a striking example of our ignorance of the mechanisms underlying symptom generation in GORD. It is essential to recognise the diversity of patients presently grouped under the “umbrella” of NERD in order to understand its pathogenesis. Functional heartburn is an important subgroup of NERD that includes patients with oesophageal acid exposure within the physiological range in addition to normal endoscopy. The mechanisms responsible for pain, clinical characteristics, and the optimal therapeutic approach remain poorly understood. However, recent studies suggest that functional heartburn accounts for up to 50% of NERD patients and is an important contributor to the unpredictable response to antireflux therapy that has been observed in NERD patients. Due to the size of this patient subgroup and the complexity of the underlying mechanisms of their symptoms, further studies will be necessary in order to develop effective therapeutic modalities, which will probably not be limited to acid suppression.
INTRODUCTION
Symptoms are the primary reason for patients to seek medical attention. Most clinic visits are due to symptoms and physicians spend much of their professional life dealing with symptoms.1 In the last century medical research has focused mainly on disease processes rather than symptoms.2 This focus has transformed medicine from a descriptive field to one that explains mechanisms of disease.1 In fact, in the last century students in medical schools have been introduced to the prevailing motto that successful treatment of diseases is achievable only by addressing the underlying mechanism. However, this change in attitude towards diseases came at a high cost: our understanding of symptoms of many medical disorders remains extremely poor. Furthermore, we have raised generations of physicians that are sceptical of symptoms when objective confirmation cannot be found.1,3,4
The emphasis on disease processes rather than symptoms has not spared the study of GORD. Despite significant progress in our understanding of the mechanisms that lead to gastro-oesophageal reflux, we have made very little progress in understanding symptoms. Recognition of transient lower oesophageal sphincter relaxation (TLOSR) as the main cause for physiological and pathological acid reflux is a typical example.5,6 While responsible for most acid reflux events, in reality TLOSRs are rarely associated with symptoms as most acid reflux events that occur in GORD patients or in healthy subjects are never perceived7 (fig 1).

Various underlying mechanisms have been recognised as causing acid reflux events. However, patients with gastro-oesophageal reflux disease (GORD) do not perceive most acid reflux events. The “missing link” represents mechanisms which are currently unknown that are essential for typical GORD symptoms to evolve in response to acid reflux. TLOSR, transient lower oesophageal sphincter relaxation; LOS, lower oesophageal sphincter.
Remarkably, the exact causes responsible for GORD symptoms continue to elude us. Part of the problem is our obsessive focus on the oesophageal mucosal injury produced by excessive acid reflux rather than on symptoms per se. For decades, almost all the therapeutic trials in GORD have concentrated almost exclusively on oesophageal healing rates and on symptomatic responses in patients with erosive oesophagitis only. Very few therapeutic trials have been conducted in patients with NERD, and even less on symptom generation in this subset of patients.
Another aspect of the problem is the lack of association between symptom severity or frequency and the presence or absence of oesophageal inflammation.8 Furthermore, there is no association between symptom severity and the extent of oesophageal mucosal injury. Using data pooled from 16 independently conducted clinical treatment trials, Carlsson et al examined the prevalence of heartburn symptoms in patients with or without erosive oesophagitis.9 Their meta-analysis convincingly showed that moderate to severe heartburn was as prevalent among patients with grade 1 (mucosal erythema) or grade 2 (non-circumferential erosions), with a respective prevalence of 71.7% and 75.8%, as patients with grade 3 (circumferential erosions) and grade 4 (oesophageal ulceration) where the prevalence of heartburn was 74.4% and 64.2%, respectively.9 Other symptoms, such as acid regurgitation, were also equally prevalent among patients with little or no mucosal injury and those with erosive oesophagitis .
In recent years, more attention has been directed towards patients with NERD. This stems from several pivotal therapeutic GORD trials that were conducted in patients recruited in the community rather than tertiary practices. Two important findings emerged from these studies: firstly, most community patients with heartburn have no oesophageal mucosal injury. Secondly, and this is a priori somewhat surprising, patients with typical GORD symptoms but a normal oesophageal mucosa demonstrate lower rates of symptom improvement with potent antireflux treatment than patients with erosive oesophagitis.10 These findings require us to reassess our understanding of the mechanisms that lead to symptom generation in GORD, particularly in patients with normal oesophageal mucosa.
DEFINITIONS
Classic GORD symptoms (heartburn and acid regurgitation) in the presence of a normal oesophageal mucosa have been used to define NERD, also called endoscopy negative reflux disease.11 This type of classification assumes that all patients that present with heartburn have some degree of GORD, regardless of whether oesophageal inflammation or excessive oesophageal acid exposure is present.10 Recently, an alternative definition has been proposed for NERD. NERD would be diagnosed in the presence of typical GORD symptoms (heartburn and acid regurgitation) caused by intra-oesophageal acid, in the absence of oesophageal mucosal injury at endoscopy.12 This definition implies that GORD symptoms require acid, but that their cause resides not in the severity or frequency of the acid exposure, but rather in its perception. It also excludes those patients with classic heartburn due to non-acid related stimuli.
NERD constitutes a heterogeneous group of patients. One of the subgroups includes those patients that have been termed as functional heartburn. The “Rome II” committee for functional oesophageal disorders defined functional heartburn as an episodic retrosternal burning in the absence of pathological gastro-oesophageal reflux, pathology based motility disorders, or structural explanations.13 This definition is vague and clearly does not provide any clues to the different underlying mechanisms that may lead to heartburn in these patients. When it comes to understanding symptoms in GORD and specifically in patients with functional heartburn, a traditional “intraluminal” view is insufficient. Other factors including central and peripheral neural mechanisms should be taken into consideration in order to understand the basis of the symptoms experienced by these patients.
EPIDEMIOLOGY
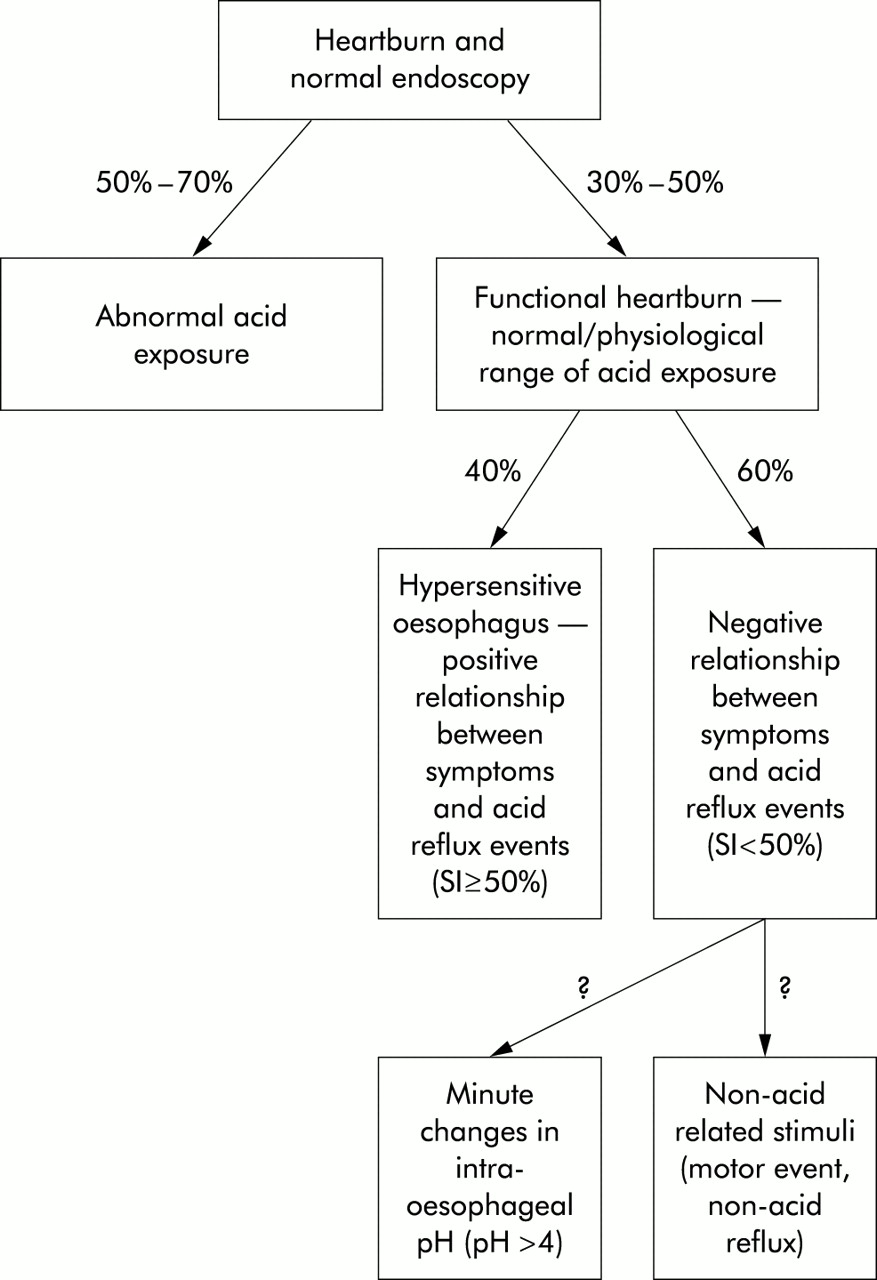
It is unclear how common functional heartburn is, in large part because most patients with heartburn do not seek medical attention.14 Several recent population based studies demonstrated that up to 70% of participants reporting heartburn have no evidence of mucosal injury at endoscopy.15,16 These results are in contrast with a previous report that suggested that approximately half of patients presenting to a tertiary referral centre with heartburn for the first time had a normal endoscopy.17,18 Among patients with NERD, between 30% and 50% have normal 24 hour oesophageal pH monitoring, defined by duration of acid exposure (pH <4) over a period of 24 hours, and thus meet the diagnostic criteria set for functional heartburn.15,19–21 In a recent study, Martinez et al evaluated 71 NERD patients and demonstrated that in 50% that underwent pH testing normal distal oesophageal acid exposure was present.22
“It is likely that females tend to seek more medical attention than males, resulting in the false impression that NERD and functional heartburn are primarily female disorders”
Demographic studies in patients with NERD revealed a younger, non-obese, and predominately female group.8 Yet we have to recall that most patients with GORD as well as those with functional heartburn never seek medical attention and thus these reports may be biased. Presently, very little is known about the medical seeking behaviour of patients with functional heartburn. However, as with other functional bowel disorders it is likely that females tend to seek more medical attention than males, resulting in the false impression that NERD and functional heartburn are primarily female disorders.23
SUBCLASSIFICATION OF FUNCTIONAL HEARTBURN
When assessing the underlying mechanisms for GORD symptoms in patients with functional heartburn it appears that this is also a heterogeneous group of patients. The presence of classic heartburn symptoms in the absence of oesophageal mucosal injury and abnormal acid exposure may suggest that some patients are sensitive to physiological amounts of acid that most normal subjects experience but do not perceive. Another subset of patients demonstrates the presence of non-acid intra-oesophageal stimuli that trigger typical heartburn.24 Potentially, there are other distinct subgroups grouped within the functional heartburn group, but data on these are relatively scant.
The first subgroup, variously termed hypersensitive or acid sensitive oesophagus, includes patients that despite having an oesophageal acid exposure within the physiological range demonstrate a close temporal relationship between symptoms and acid reflux events. These patients display a similar mean per cent heartburn episodes at pH <4 (70%) as patients with NERD and abnormal pH testing (73–85%).22,25 A recent study has estimated that 40% of patients with functional heartburn may fall into this category.22 These patients demonstrate a favourable response to antireflux treatment but only when high doses of proton pump inhibitors (PPIs) are used.26
In contrast, in another subset of patients there is a very low correlation between the occurrence of heartburn and acid reflux. Weiner et al have shown that NERD patients are less likely to exhibit a strong association between heartburn symptoms and acid reflux events than patients with erosive oesophagitis.25 Half of these patients had a symptom index that was less than 50%. These data suggest that heartburn in those patients is either due to non-acid related stimuli or factors other than luminal stimuli. In a similar group of patients, Martinez et al reported that the mean symptom index was 12.7%, the mean number of acid reflux events 27.5 (compared with 70.7 in the hypersensitive oesophagus group and 154 in NERD patients with an abnormal pH test), and that as much as 40% of symptoms occurred at pH >6.22
“NERD patients are less likely to exhibit a strong association between heartburn symptoms and acid reflux events than patients with erosive oesophagitis”
It is highly likely that there are other subgroups within the functional heartburn group. Some patients demonstrate an increased sensitivity to minute changes in oesophageal pH, even if it does not fall below a pH of 4.12 These patients demonstrate lack of relationship between symptoms and acid (pH <4) reflux events. Therefore, some patients may be mistakenly considered as having heartburn due to non-acid related stimuli while in fact exhibiting increased sensitivity to small increases in oesophageal acid exposure.
Another important factor confounding the categorisation of patients into groups such as NERD and functional heartburn stems from the fact that in some instances symptoms and mucosal injury may have been altered by prior medical therapy, or dietary or lifestyle adjustments. As these symptoms are often chronic, not only will physicians have been previously consulted, in many instances patients themselves will have treated their symptoms in a number of variously effective manners. The potentially confounding effect of these manoeuvres is poorly understood and not always factored in many studies.
In fig 2 we propose a classification of the various subgroups of patients with heartburn symptoms and normal endoscopy and their estimated respective prevalence.22 Further studies are likely to expose the full diversity of that large group of patients that is currently categorised as functional heartburn.

Proposed classification of patients with typical heartburn and normal upper endoscopy as well as subclassification of patients with functional heartburn. It is likely that the diversity of patients is broader and there are other potential subgroups that are currently poorly recognised. Non-erosive reflux disease was replaced by the term heartburn and normal endoscopy due to the evidence that some patients under this category have classic heartburn due to non-acid related intra-oesophageal events.
ROLE OF PERIPHERAL AND CENTRAL NEURAL FACTORS IN THE PATHOGENESIS OF OESOPHAGEAL SYMPTOMS
Perception of intra-oesophageal stimuli
As previously mentioned, patients with GORD do not perceive most acid reflux events. Many patients and healthy subjects demonstrate multiple acid reflux events on pH testing but often report few, if any, heartburn episodes. It has been estimated that no more than 5% of all acid reflux events (pH <4) produce symptoms, either in patients with or without oesophageal mucosal injury.22 This intriguing observation raises the obvious question of what in a specific acid reflux event leads to its conscious perception. It is not clear if a specific acid reflux event is the determining factor in triggering symptoms or rather the actual hydrogen ion concentration [H+] of the refluxate, the summation of several short reflux events, or an increased number and/or duration of acid reflux events.
“The most common trigger for GORD symptoms is a meal”
The most common trigger for GORD symptoms is a meal; in particular if the meal is high in fat. However, the mechanism by which fat exacerbates symptoms in patients with GORD remains controversial. In a recent study, Meyer et al found that fat infusion into the duodenum of subjects with GORD significantly shortened latency to onset of heartburn and intensified the perception of acid induced heartburn.26 The mechanisms by which luminal fat and potentially other nutrients may modulate the perception of oesophageal stimuli remains unclear but may involve cholecystokinin or other gut neurotransmitters, hormones, and enzymes. While many of these peptides may exert a local action leading to symptoms, it is also conceivable that their action may also involve central neural pathways. It is even possible that other substances in the refluxate (pepsin, bile) or volume per se are the direct cause of symptoms.
Several studies have recently speculated that central and peripheral neural mechanisms modulate oesophageal perception (fig 3).10,12 Psychological comorbidity (anxiety, stress, depression, etc.) can modulate oesophageal perception and cause patients to perceive low intensity oesophageal stimuli as being painful.27 These psychological factors seem to be associated with patients paying an excessive attention (hypervigilance) to intra-oesophageal events and thus perceiving or interpreting these oesophageal events as being painful.28 Stress has been implicated by 64% of GORD patients as an important cause for symptom exacerbation.29 However, several studies have failed to demonstrate an increase in acid reflux during stressful stimuli.30–32 Nevertheless, interventions aimed at reducing stress (hypnosis and muscle relaxation) have produced subjective improvement in reflux symptoms ratings.32,33 In a study assessing the effect of psychologically induced stress on symptom perception in GORD patients, stress reduced perception thresholds and enhanced the perception of acid during infusion, regardless of the degree of oesophageal mucosal injury.34

{kind=link}
{kind=link}
{kind=link}
Proposed conceptual model for symptom generation in patients with non-erosive reflux disease. This model suggests that central (through brain-gut interactions) and peripheral mechanisms are essential for intra-oesophageal stimuli (either physiological or pathological) to reach the conscious level and thus be perceived.
A recent study demonstrated that increased basal sympathetic activity and lower vagal activity, as measured by power spectral analysis of heart rate variability, are associated with increased sensitivity to intra-oesophageal acid perfusion in patients with non-cardiac chest pain compared with healthy matched controls.35
These data support the concept of humoral, neural, and psychological factors being associated with an increased susceptibility to symptoms such as heartburn but do not provide at this point a satisfactory mechanistic explanation. However, recent advances in our understanding of the mucosal and oesophageal neural response to reflux begin to address this deficiency, and are outlined in the oesophageal innervation section
IS ACID THE SOLE CULPRIT?
There are mounting data to suggest that the axiom no acid no heartburn is obsolete. Non-acid intra-oesophageal stimuli may also lead to the development of heartburn. Oesophageal balloon distension induces heartburn symptoms in a large subset of normal subjects and reproduces typical heartburn in half of GORD patients.36 Furthermore, high frequency intraluminal ultrasonography has demonstrated a close correlation between heartburn episodes and abnormally long durations of longitudinal muscle contractions in the oesophagus.37 These muscle contractions and consequent heartburn episodes can certainly occur in the absence of acid reflux. Thus both of these studies suggest that mechanical stimuli and motor events may be perceived as heartburn by some patients, even in the absence of actual acid reflux.
“There are mounting data to suggest that the axiom no acid no heartburn is obsolete”
Bile reflux has been suggested as a possible cause for heartburn symptoms in patients with NERD but no study to date has specifically evaluated the role of bile acid in symptom generation in this group. Assessment of bilirubin pigment spectrophotometrically, a proxy indicator for bile reflux, revealed a close correlation between a combination of both acid and duodenogastro-oesophageal reflux and severity of GORD, as determined by the presence of oesophageal mucosal injury and GORD complications.38 However, symptoms were not specifically examined in this study. The combined reflux was documented in only 50% of NERD patients compared with 79% in erosive oesophagitis and 95% in Barrett’s oesophagus. Others have shown that the mean fasting gastric bile acid concentration in patients with NERD is not significantly elevated compared with healthy controls.12 Future studies are needed to further determine if bile acid is a contributing factor for symptoms in patients with NERD and specifically in those with functional heartburn.
Recent studies using simultaneous intra-oesophageal impedance and pH measurement demonstrated non-acid gastro-oesophageal reflux (pure liquid or mixture of gas and liquid) that was similarly frequent in patients with GORD and normal controls.39 However, more acidic reflux occurred in symptomatic patients with GORD. Vela et al, with a similar technique, observed that during treatment of GORD patients with a PPI, postprandial reflux became predominately non-acidic.40 Although less than acidic reflux, non-acidic reflux was also associated with classic GORD symptoms. It has yet to be determined if the content or volume is responsible for GORD symptoms in the studied subjects. Additionally, as with acid reflux, most of non-acid reflux events are not perceived. However, assessment of patients with functional heartburn by using this new technique may prove valuable in the future in understanding symptom perception.
OESOPHAGEAL INNERVATION
The oesophagus, in common with the rest of the viscera, receives dual sensory innervation, traditionally referred to as parasympathetic and sympathetic, but more properly based on the actual nerves, vagal and spinal.41 The vagal afferent neurones compose 80% of the vagal trunk and have cell bodies in the nodose ganglia.42 Vagal afferents whose receptive fields are located in the oesophageal smooth muscle layer are sensitive to mechanical distension while polymodal (responding to multiple modalities of stimuli) vagal afferents with receptive fields in the mucosa are sensitive to a variety of chemical or mechanical intraluminal stimuli that under normal circumstances are not associated with conscious perception.43 In general, vagal afferents do not play a direct role in visceral pain transmission at the level of the gut, except for certain types of vagal afferents that appear to have a pain modulatory effect.44 Recent reports suggest that vagal afferents also may play a role in perception of oesophageal distension.44,45 In contrast, spinal afferents, which have their cell bodies in the dorsal root ganglia, are primarily acting as nociceptors and are central to the perception of discomfort and pain.46 Spinal afferents with receptive fields in the muscle layer and serosa are primarily mechanosensitive. The intraepithelial nerve endings of spinal afferents are likely to be involved in mediating acid induced pain during topical exposure to intraluminal acid.36,47 Many of these afferents contain calcitonin gene related peptide and substance P, which are neurotransmitters that are important in mediating visceral nociception.42
“The mechanisms by which patients with GORD develop symptoms remain incompletely understood”
The mechanisms by which patients with GORD develop symptoms remain incompletely understood. It is postulated that sensitisation of oesophageal chemoreceptors either directly by exposure to acid reflux or indirectly through release of inflammatory mediators is responsible for symptom generation in GORD.36 Reducing acid exposure in patients with GORD appears to normalise the sensitivity to acid.48 However, the emergence of symptoms in patients with a normal oesophageal mucosa and thus without obvious inflammation remains perplexing, particularly among patients with functional heartburn where little or no reflux actually occurs.
Both animal models and human studies have demonstrated dilatation of intercellular spaces during or following oesophageal mucosal acid exposure.49,50 These mucosal findings were evident regardless of the presence or absence of oesophageal inflammation.50,51 It is assumed that these morphological changes result in an increase in paracellular permeability, allowing acid to reach sensory nerve endings located within the intercellular spaces.52 However, this altered permeability does not explain symptoms in NERD and in functional heartburn as most acid reflux events (>95%) that occur in these patients are never perceived and symptoms occur even in the absence of acid reflux, suggesting the importance of other factors in modulating oesophageal acid perception.
“Heartburn symptoms may represent activation of a common pathway in response to different intra-oesophageal stimuli”
Heartburn symptoms may represent activation of a common pathway in response to different intra-oesophageal stimuli. Hypersensitivity to physiological amounts of acid appears to be the underlying mechanism for heartburn in the hypersensitive oesophagus subgroup. This hypersensitivity to acid may stem from peripheral sensitisation of oesophageal afferents, leading to heightened responses to luminal stimuli or altered modulation of afferent neural function at the level of the spinal dorsal root or the central nervous system.53 What leads to the development of such hypersensitivity remains an area of controversy. In healthy subjects, Sarkar et al have recently demonstrated that infusion of 0.1 N hydrochloric acid into the distal oesophagus for 30 minutes increased the subsequent sensory responses to electrical stimulation in the non-exposed proximal oesophagus.54 In comparison, patients with non-cardiac chest pain already had lower resting oesophageal pain thresholds in the proximal oesophagus, which fell further and for a longer duration than in healthy subjects after acidification of the distal oesophagus. These patients also demonstrated a decrease in pain thresholds in the anterior chest wall. Therefore, this study showed the development of secondary allodynia (visceral hypersensitivity to innocuous stimulus in normal tissue that is in proximity to the site of tissue injury) in healthy subjects and non-cardiac chest pain patients. In the latter group this phenomenon is amplified and lasts longer. The resulting visceral and somatic hypersensitivity is likely due to central sensitisation. The increased excitability of spinal cord neurones appears to be the result of activation of nociceptive C fibres due to local tissue injury induced by acid infusion into the distal oesophagus. If extrapolated clinically, this study suggests that prior injury to the oesophageal mucosa may lead to the development of central sensitisation and visceral hyperalgesia in a subset of patients long after the local injury has healed.
CORTICAL REPRESENTATION OF PERCEIVED OESOPHAGEAL ACID
To date, only a few studies have attempted to assess the cortical processing of oesophageal sensation in humans. Aziz et al examined the human brain loci involved in the processing of oesophageal sensation using positron emission tomography (PET) and distal oesophageal balloon distention in eight healthy volunteers.55 Non-painful stimuli elicited bilateral activation along the central sulcus, insular cortex, as well as the frontal and parietal operculum. Painful stimuli resulted in intense activation of the same areas and additional activation of the right anterior insular cortex and the anterior cingulate gyrus. The former is important in affective processing while the latter is important in pain processing and generating an affective and cognitive response to pain.56–58 In another study, Kern et al evaluated activation of cerebral cortical responses to oesophageal mucosal acid exposure using functional magnetic resonance imaging (FMRI).59 Ten healthy subjects underwent intra-oesophageal perfusion of 0.1 N hydrochloric acid over 10 minutes. None of the study subjects reported GORD symptoms during acid perfusion. Cerebral cortical activity was concentrated in the posterior cingulate, and the parietal and anteromesial frontal lobes. The superior frontal lobe regions activated in this study corresponded to Brodmann’s areas 32, the insula, operculum, and the anterior cingulate. Further studies are needed to assess cerebral cortical activation in symptomatic GORD patients undergoing oesophageal acid perfusion. In addition, it would be of great interest to determine if there are differences in central processing of an intra-oesophageal stimulus between GORD patients and those with NERD or functional heartburn. It is also important to begin to examine the role of psychophysiological states such as stress, anxiety, and depression, and their effects on central nuclei involved with perception of oesophageal stimuli. To move forward, we will have to go from purely topographical and phenomenological studies to more mechanistic studies designed to address the pathways and neurotransmitters involved in these symptoms. While the technology is there, including PET and FMRI, it is essential that the right questions be asked for the necessary progress to take place.
DIAGNOSIS
At present, there are no predictive factors that can be elicited from history and thus can help us determine whether patients with GORD symptoms have functional heartburn. In general, there is no correlation between the severity of GORD symptoms and the presence or absence of oesophageal inflammation.8 Thus the diagnosis of functional heartburn requires upper endoscopy to confirm the absence of mucosal damage. However, endoscopy provides no information regarding the other subgroups of NERD even if biopsies are obtained from the distal oesophagus. In one study, biopsies were obtained at 2 cm and 5 cm above the oesophagogastric junction in patients with NERD and a positive pH test, in patients with functional heartburn, and in normal subjects.60 Oesophageal biopsies had a sensitivity of 46% in detecting morphological abnormalities compatible with acid damage in the oesophageal mucosa (elongated papillae, increased thickness of the basal zone, and inflammatory cells infiltrate) of NERD patients with an abnormal pH test. In patients with functional heartburn, the sensitivity of biopsies ranged between 0% at 2 cm and 9% at 5 cm (for elongated papillae and increased basal thickness). This study suggests that patients with functional heartburn will demonstrate very little, if any, morphological changes consistent with GORD.
In addition to an unremarkable upper endoscopy, detection of oesophageal acid exposure within the physiological range in the distal oesophagus is necessary for diagnosing functional heartburn. Presently, the latter can be achieved only by ambulatory 24 hour oesophageal pH monitoring. However, many authorities suggest that invasive diagnostic modalities, such as pH testing, should be reserved only for patients with classic GORD symptoms who have failed standard dose PPI therapy.
“Establishment of a diagnosis such as functional heartburn is important in patients who fail standard dose PPIs”
Establishment of a diagnosis such as functional heartburn is important in patients who fail standard dose PPIs. NERD patients that are likely to fail PPI therapy commonly originate from the functional heartburn group. Lind et al demonstrated that approximately half of patients with functional heartburn failed daily omeprazole 20 mg.15 Evaluation by ambulatory 24 hour oesophageal pH monitoring has been recommended in those patients that continue to have typical GORD symptoms on a standard dose PPI.61 Studies evaluating the extent of oesophageal acid exposure in patients with functional heartburn are still lacking, but in patients with NERD who failed standard dose PPI the likelihood that the pH test will demonstrate values within the normal range exceeds 60%.62 Although the exact ratio is unknown, most of these patients are likely to have functional heartburn. However, in the reality of clinical practice compounded by lack of general availability of the pH test, many functional heartburn patients who fail standard dose PPI will be offered double dose therapy. This therapeutic approach may not lack merit because many patients with a hypersensitive oesophagus will respond to higher doses of PPI.63
CURRENT AND FUTURE TREATMENT
Very few studies have rigorously assessed treatment options in patients with functional heartburn. In NERD patients, the symptoms response rate after four weeks of standard dose PPI therapy ranges between 46% and 57%.15,64 This surprisingly low response rate is almost 10–30% less than what has been observed in patients with erosive oesophagitis receiving a similar dose.65 The functional heartburn group is likely the main reason for the limited clinical response to PPI therapy in NERD patients. More than 45% of patients with functional heartburn reported insufficient control of heartburn after four weeks of treatment with omeprazole 20 mg once daily.15 Interestingly, in the same study, the authors demonstrated that in patients with NERD receiving omeprazole 20 mg daily, the higher the acid exposure in the distal oesophagus the greater the symptom response. Thus duration of distal oesophageal acid exposure appears to be a reliable predictive factor for response to PPI therapy.
In patients with functional heartburn who failed standard dose PPI, the hypersensitive oesophagus subgroup may potentially respond to higher doses of PPI. Further suppression of gastric acid and thus minimisation of oesophageal acid exposure may eventually result in symptom improvement or possibly complete symptom relief. While using omeprazole 40 mg daily over a period of 14 days, Schenk et al demonstrated a 37% symptom response rate in patients with functional heartburn.19 In another study, omeprazole 40 mg in the morning and 20 mg in the evening were administered for a period of seven days to patients with functional heartburn.21 More than 40% of patients reported a greater than 50% reduction in symptom intensity. Watson et al performed a double blind, crossover, placebo controlled trial of omeprazole 20 mg twice daily over four weeks in the treatment of patients with functional heartburn.63 The drug improved symptoms in 61% of subjects. As expected, almost all responders also had a positive correlation between their symptoms and acid reflux events. This study, although lacking long term follow up, further cements the notion that the hypersensitive oesophagus subgroup will likely respond to higher doses of PPI. It has yet to be elucidated how high one can raise the PPI dose and still improve symptoms or increase the number of responders.
Pain modulators have not been systematically studied in patients with functional heartburn but may ultimately become an essential component of the therapeutic armamentarium for this disorder. The pain modulators may be effective on their own in certain subsets of patients with functional heartburn, or in combination with a PPI in others. Low doses of tricyclic antidepressants, trazodone, or selective serotonin reuptake inhibitors have been shown to reduce pain in other functional oesophageal disorders, such as non-cardiac chest pain.66,67 The 5-HT3 antagonists may also have a certain pain modulatory effect, probably by altering initiation, transmission, or processing of extrinsic sensory information from the gastrointestinal tract.68 The effect of 5-HT4 agonists on visceral perception has yet to be examined in humans. Tegaserod, a partial 5-HT4 agonist, may prove to be efficacious in patients with functional heartburn by reducing acid reflux events and potentially modulating oesophageal pain perception69 but clinical studies are needed to support these possibilities. Other agents with visceral analgesic effect, currently under investigation, may eventually become important additions to our treatment of functional bowel disorders as well as functional heartburn. These include κ agonists, neurokinin receptor antagonists (NK1 and NK2), as well as N-methyl-d-aspartate receptor antagonists.54
“The role of antireflux surgery in functional heartburn has not been assessed”
The role of antireflux surgery in functional heartburn has not been assessed. Studies that evaluated the efficacy of antireflux surgery in patients with NERD specifically excluded those with normal pH testing.70 It is currently believed that functional heartburn patients will not benefit from this type of therapeutic intervention.
In summary, patients with functional heartburn should be approached as patients with NERD and treated with antireflux medications. Due to the need for profound acid suppression in this group of patients, PPIs should be considered relatively early in their care. Failure to respond to standard dose of PPI will require doubling the dose. If patients continue to report heartburn symptoms while receiving PPI twice daily (am—before breakfast, and pm—before dinner), then adding or switching to pain modulators may be appropriate.
In conclusion, functional heartburn is a common disorder and appears to be composed of several distinct subgroups. Presently, identifying the different subgroups based on clinical history only is not achievable. Response to potent antireflux treatment is relatively limited. Current and future treatment strategies for functional heartburn patients who have failed standard dose PPI include increased PPI dose in some as well as addition of pain modulators in others.
Acknowledgments
This paper is a modified and updated version of a short paper orginally published in Spanish in a book entitled “Gastroenterología, Hepatología y Nutrición Basadas en Evidencias”, Masson, Mexico, 2002. This book contains handouts submitted to the 2001 annual course of the Instituto Nacional de Ciencias Médidac y Nutrición Salvador Zubiran, Mexico City, Mexico.