Article Text

Abstract
Background and aims Portal vein thrombosis (PVT) negatively impacts the prognosis in patients with cirrhosis. The aim of our study was to evaluate the effects of transjugular intrahepatic portosystemic shunt (TIPS) placement in patients with cirrhosis complicated by PVT.
Methods Seventy consecutive cirrhotic patients with non-tumoural PVT treated with TIPS for portal hypertension complications from January 2003 to February 2010 in a tertiary-care centre were followed until last clinical evaluation, liver transplantation, or death.
Results TIPS was successfully placed without major procedure-related complications. After TIPS, the portal venous system was completely recanalised in 57% of patients, a marked decrease in thrombosis was observed in 30%, and no improvement was seen in 13%. 95% of patients with complete recanalisation after TIPS maintained a patent portal vein. Predictors of complete recanalisation were a less severe and extensive PVT, de novo diagnosis of PVT, and absence of gastro-oesophageal varices. At follow-up, 1 patient had recurrence of bleeding, and 2 had spontaneous bacterial peritonitis. The rate of TIPS dysfunction at 12 and 24 months was 38% and 85% for bare stent and 21% and 29% for covered stent (p=0.001), respectively. Occurrence of encephalopathy at 12 and 24 months was 27% and 32%, respectively. Fifteen patients underwent liver transplantation. Survival at 1, 12 and 24 months was 99%, 89% and 81%, respectively.
Conclusion Long-term outcome of non-tumoural PVT in patients with cirrhosis treated with TIPS placement is excellent. Prospective randomised studies should investigate whether TIPS placement is the best therapeutic option in patients with cirrhosis who develops non-tumoural PVT.
- Cirrhosis
- thrombosis
- TIPS
- anticoagulation
- thrombolysis
- hepatobiliary radiology
- imaging
- liver transplantation
- portal hypertension
Statistics from Altmetric.com
- Cirrhosis
- thrombosis
- TIPS
- anticoagulation
- thrombolysis
- hepatobiliary radiology
- imaging
- liver transplantation
- portal hypertension
Significance of this study
What is already known about this subject?
Several small series have shown that in patients with cirrhosis and portal vein thrombosis (PVT), the placement of a transjugular intrahepatic portosystemic shunt (TIPS) is technically feasible and may have beneficial effects on PVT.
What are the new findings?
This study clearly shows that TIPS placement is effective for treatment of non-tumoural and non-cavernous PVT in patients with cirrhosis.
The recanalisation after TIPS, in the absence of thrombolytic or anticoagulation therapy, occurs over a period of time, ranging from a few months to more than a year.
Less severe and extensive PVT, diagnosis of de novo PVT, and absence of varices are independent predictors of complete recanalisation after TIPS placement.
In patients with cirrhosis complicated by PVT, TIPS is not associated with an increased risk of procedure-related complications, stent occlusion or mortality.
How might it impact on clinical practice in the foreseeable future?
TIPS is a rational option in the management of patients with cirrhosis complicated by non-tumoural and non-cavernous PVT. This may be especially valuable, particularly in patients eligible for liver transplantation in whom extension of the thrombosis may increase the risks associated with surgery.
Prospective randomised studies should investigate whether TIPS is a better option than anticoagulation, or whether it should be reserved for anticoagulation failures/contraindications.
Introduction
The prevalence of portal vein thrombosis (PVT) in patients with cirrhosis ranges from 1% to 25%.1–5 Potential factors contributing to the risk of PVT include the slow portal blood flow velocity characteristic of portal hypertension, and concomitant thrombophilic disorders that may be associated.6–8 PVT negatively impacts the prognosis of these patients because of a further increase in portal hypertension, with increased risk of complications, decreased liver perfusion, and worsening of liver function.9 10 In addition, the progression to complete and extensive thrombosis may exclude patients from transplantation or require complex surgical techniques associated with high risk of morbidity and mortality.11 12
The question of optimal treatment for non-tumoural PVT in patients with cirrhosis has not been addressed in any consensus publication, including the most recent practice guidelines.13 Anticoagulant therapy may prevent the extension of a recent PVT and, in some cases, allows for complete recanalisation.5 However, there is some concern over the use of anticoagulation in patients with advanced liver disease because of the risk of gastrointestinal bleeding and immune thrombocytopenia, but also because the anticoagulation, by increasing the internationalised normalised ratio (INR), interferes with the use of the model for end-stage liver disease (MELD) score for prioritising patients for liver transplantation. Several small series have shown that transjugular intrahepatic portosystemic shunt (TIPS) is not only technically feasible, but perhaps also beneficial for treating PVT in patients with cirrhosis,14–21 though long-term outcome is poorly defined.
The aim of this study was to evaluate the short- and long-term effects of TIPS placement in patients with cirrhosis complicated by non-tumoural PVT.
Patient and methods
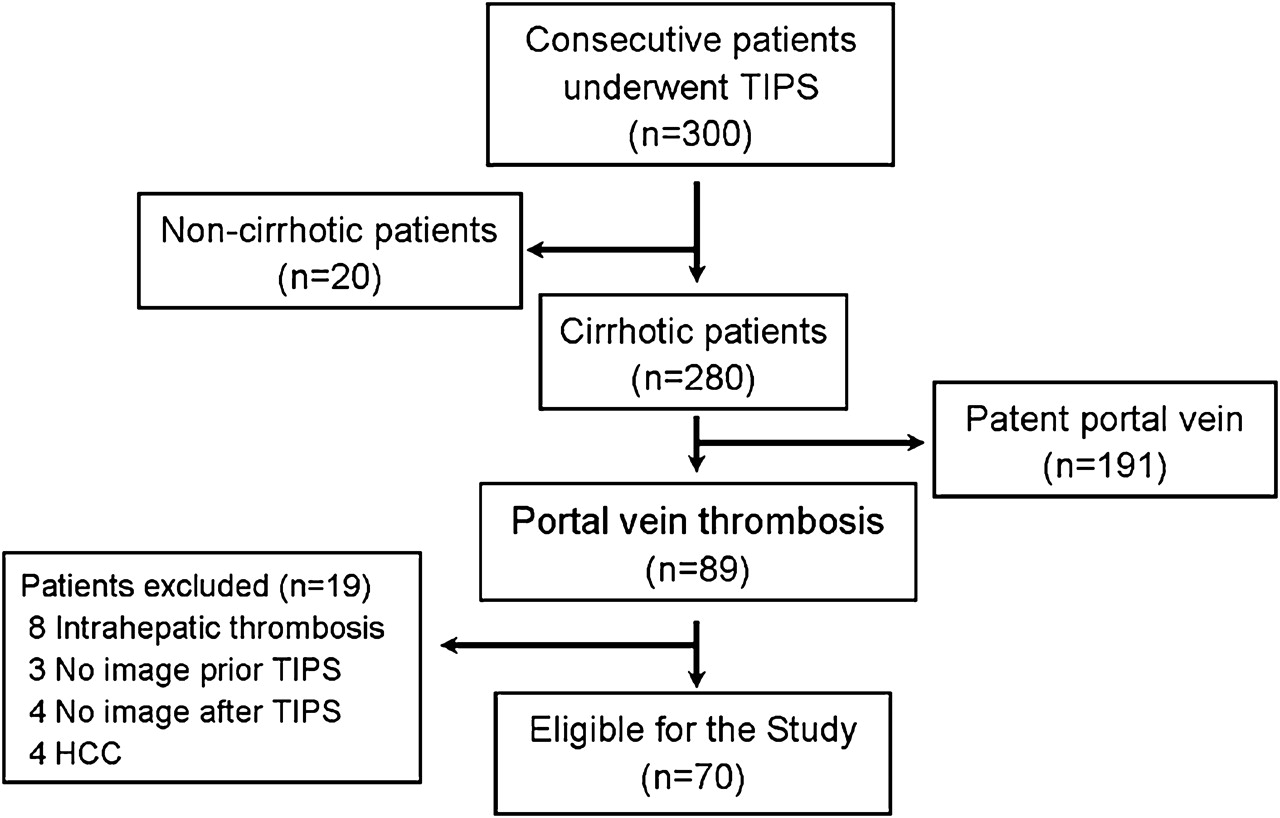
Between January 2003 and February 2010, 300 consecutive patients underwent TIPS placement for portal hypertensive complications at our institute. Of these 300 patients, 280 had cirrhosis, and 89 (30%) had associated PVT prior to TIPS. Nineteen patients were excluded because the thrombosis was limited to the right and/or left portal vein branches (n=8), or because they have hepatocellular carcinoma (HCC, n=4) or they did not undergo imaging study prior (n=3) or after TIPS (n=4) (figure 1). Finally, a total of 70 patients were included in this study. In all patients, the diagnosis of PVT, as well as the estimation of extent and severity of thrombosis prior to and after TIPS placement, was performed with contrast-enhanced multidetector CT and/or magnetic resonance angiography (MRA). Liver cirrhosis was diagnosed by liver biopsy or by unequivocal clinical, laboratory and imaging findings. The exclusion criteria for TIPS placement were hepatic encephalopathy, multinodular HCC, tumorous PVT, cardiopulmonary co-morbidity, active infection, or organic renal disease. During the period of the study, 51 patients with cirrhosis and cavernous transformation with no detectable portal remnant were also excluded. The study was approved by our institute's Internal Review Board, and written informed consent was obtained for every procedure from all patients.

Patients treated with transjugular intrahepatic portosystemic shunt (TIPS) between January 2003 and February 2010 in a tertiary-care centre. HCC, hepatocellular carcinoma.
TIPS procedure
All TIPS were performed with a right internal jugular vein approach, using a standard technique. Access to the right or left portal vein branch was achieved with a combination of ultrasound and fluoroscopic guidance. A hydrophilic guidewire was used to negotiate entrance into the main portal vein. Once the occlusion was crossed, a dilatation of the intrahepatic tract was performed with an 8 mm Blue Max balloon catheter (Boston Scientific, Natick, Massachusetts, USA). We used Wallstent endoprostheses (Boston Scientific) until May 2006, and subsequently e-PTFE covered stents (Viatorr®; W.L. Gore & Associates, Flagstaff, Arizona, USA). The stent was deployed so as to ensure the distal end would not compromise future surgical procedures, such as liver transplantation. Embolisation of collaterals was only considered when filling of large portosystemic vessels was observed at post-TIPS portography. In patients with severe PVT (>75% of lumen occupancy at the cross-sectional imaging), an 8–10 mm dilating balloon catheter was employed for partial recanalisation (mechanical thrombolysis) after stent deployment.
None of the patients received local or systemic thrombolytic or anticoagulation therapy at the time of the procedure and/or at follow-up. TIPS revision was performed whenever clinical or Doppler ultrasound data suggested stent dysfunction (occlusion or stenosis). Doppler ultrasound criteria for TIPS dysfunction were portal flow velocity lower than 30 cm/s, change in the direction of flow in the intrahepatic portal branches from fugal to petal, intrastent flow velocity lower than 60 or higher than 190 cm/s, or intrastent flow velocity gradient greater than 50%.22 If TIPS dysfunction was confirmed by an increase in the portal–caval pressure gradient (PPG) to above 12 mm Hg, angioplasty and/or restenting was performed in order to decrease PPG below 12 mm Hg.
Imaging studies
Patients were imaged using multidetector computed tomography (MDCT; Light Speed 16 and VCT 64; GE Medical Systems, Milwaukee, Wisconsin, USA) or 1.5 T MRA with high-performance gradients (Signa HDx Echospeed; GE Medical Systems). The study protocol included the acquisition of unenhanced images of the entire liver, followed by acquisition of triple-phase contrast-material-enhanced images during the hepatic arterial phase, portal venous phase and equilibrium phase. Contrast-enhanced MDCT images were obtained with a dose of 1.8 ml/kg body weight of non-ionic iodinated contrast material (iopramide 370 mg I/ml, Ultravist; Bayer-Shering Pharma, Berlin, Germany), as previously reported.23 Contrast-enhanced MRA images were obtained with a dose of 0.025 ml/kg of Gd-BOPTA (gadobenate dimeglumine, Multihance; Bracco, Milan, Italy) injected at a flow rate of 2 ml/s, followed by a flush of 20 ml of saline, and using a T1-weighted 3-D gradient-recolled echo (GRE) sequence, 5 mm slice thickness and 2 mm of intersection gap.
Image interpretation
Radiological images were analysed by three faculty-level radiologists with extensive experience in liver imaging. All images were evaluated on an LCD 21-inch display with spatial resolution of 2×5 MP (Barco, Brussels, Belgium) by means of a picture archiving and communications system (PACS, Centricity version 3.03; GE Medical Systems). For the purpose of this study, the following segments of the portal-vein system were examined: main portal vein (MPV), superior mesenteric vein (SMV), and splenic vein (SV). Thrombosis was defined as the presence of solid material in the vascular lumen, and for every venous segment, thrombosis was estimated as the percentage of lumen occupancy measured on cross-sectional images. Severity of PVT was classified as grade I<25%; grade II=26–50%; grade III=51–75%; and grade IV=76–100% of lumen occupancy. MPV was evaluated in the entire tract, while MV and SV were evaluated in the tract after the confluence of the secondary branches. Maximum lumen occupancy was used for this analysis. PVT was defined as de novo if the thrombosis was not present at previous screenings with MDCT or MRA, and ex novo if it was already present at the first imaging available. The recanalisation after TIPS placement was considered complete if MDCT and/or MRA showed the complete absence of filling defects in the MPV, SMV and SV. Recanalisation was considered partial if it achieved a decrease in severity of PVT in at least one vein. The diameter of the MPV before its bifurcation, and the presence of both a patent coronary vein and spontaneous splenorenal shunt (SSRS), were also evaluated.
Follow-up and data collection
All patients were followed up in the outpatient clinic with clinical, biochemical and Doppler ultrasound evaluation, initially at 1 month after TIPS, then at 3 months, and every 6 months thereafter. MDCT and/or MRA were performed 1 to 6 months after TIPS placement according to the severity of PVT, and then every 6 months. The end points evaluated during follow-up included recanalisation of the portal venous system, incidence of recurrent thrombosis, TIPS dysfunction, new admissions for liver decompensation (gastrointestinal bleeding, ascites, spontaneous bacterial peritonitis (SBP), encephalopathy, hepatocellular carcinoma), transplantation and death. The date of enrolment in the study was considered that of the first imaging procedure showing PVT (date of diagnosis). Patients were followed from the date of diagnosis until last clinical evaluation, liver transplantation, or death.
Statistical analyses
Quantitative variables are expressed as mean±SE and/or range, and qualitative variables as absolute and relative frequencies. Comparisons between groups of quantitative and qualitative variables were done with the Wilcoxon, ANOVA and χ2 tests, respectively. Recanalisation of the portal venous system, TIPS dysfunction, admissions for liver decompensation, and overall survival rates were assessed for all patients with the Kaplan–Meier method and compared with the Log-rank test. Independent predictors for recanalisation were assessed using a multivariate Cox proportional hazards model. All tests were two-sided, and a p value of <0.05 was considered statistically significant. Data handling and analyses were done with SPSS version 12.0 software.
Results
Patient characteristics at diagnosis of PVT
The cohort consisted of 70 patients (23 women and 47 men) with a mean age at the time of admission of 55±8 years (range 34–70 years). The aetiology of cirrhosis was related to hepatitis C virus infection in 53% of the patients, hepatitis B virus infection in 9%, alcohol abuse in 10%, other causes in 7%, and was cryptogenetic in 21%. The severity of liver disease was estimated according to the Child–Pugh class (A=24%; B=60%; C=16%), Child–Pugh score (mean±SD: 7.9±1.7; range: 5–12), and MELD scoring system (11.6±4.3; 11–22). Upper gastrointestinal endoscopy for evaluation of varices was performed in all patients: three had no varices (F0), 10 had small varices (F1), 34 had medium varices (F2), and 23 had large varices (F3). Fifty-eight patients had experienced gastrointestinal bleeding. Thirty-seven patients were listed in the liver transplant registry. Primary indications for TIPS insertion were prevention of recurrent episodes of gastro-oesophageal variceal bleeding in patients who had failed endoscopic and/or medical therapy (n=48), and refractory ascites or refractory hydrothorax (n=18). Four patients underwent TIPS on the basis of PVT alone, in order to recanalise the portal vein and maintain transplant waiting list status. The patients' characteristics at diagnosis are summarised in table 1.
Clinical characteristics of 70 patients with cirrhosis and portal vein thrombosis
With regard to occlusion sites, 18 (26%) patients had thrombosis of a single vessel, 34 (48%) had thrombosis of two vessels, and 18 (26%) had thrombi in all three vessels. Thrombosis compromising more than 50% of the lumen was found in 39 (56%) patients; in the remaining patients, lumen occupancy was less than 50%. Fifty-two (74%) of the patients had ex novo diagnosis of PVT, while 18 (26%) had de novo diagnosis. Patients with ex novo, compared with those with de novo diagnosis of PVT, had a greater number of vessels with thrombosis (more than one vessel: 87% vs 39%; p<0.001) and more severe SMV lumen occupancy (mean: 46% vs 10%; p<0.001). Two patients with ex novo diagnosis had cavernous transformation with detectable portal remnant. The characteristics of PVT are summarised in table 2.
Imaging findings at the inclusion in 70 patients with cirrhosis and portal vein thrombosis
Evaluation of the thrombophilic state was done in 38 patients (table 3). Excluding the data related to protein C, protein S and antithrombin deficiencies which in cirrhotic patients can be due to liver failure and not to congenital deficiencies, at least one prothrombotic factor was present in 17 (45%) patients, the most common being the MTHFR homozygosis deficiency. The rate of complete recanalisation of the portal vein was not significantly different among patients with and those without congenital prothrombotic factors (53% vs 48%, NS).
Prevalence of thrombofilic risk factors in 38 patients with cirrhosis and portal vein thrombosis
The mean interval from diagnosis of PVT to TIPS placement was 4.7 months (range: 0 to 66 months). Patients were followed up for a mean of 23.4 months (range, 1–78 months) after TIPS placement.
TIPS placement
TIPS were successfully inserted in all patients. Thirteen patients (19%) underwent bare stent (10 mm, n=12; 12 mm, n=1) placement, and 57 (81%) patients covered stent (8 mm, n=24; 10 mm, n=33) placement. A single stent was inserted in 66 patients, while in four patients an additional stent was necessary to cover the tract from the hepatic vein to the portal vein. Twenty-four patients underwent partial mechanical thrombolysis. The portal pressure gradient decreased from 20.8+5.8 to 8.5±4.1 mm Hg (p<0.001). One patient underwent embolisation of a huge coronary vein in order to increase the flow of blood into the MPV.
Outcome after TIPS placement
Recanalisation of the portal venous system
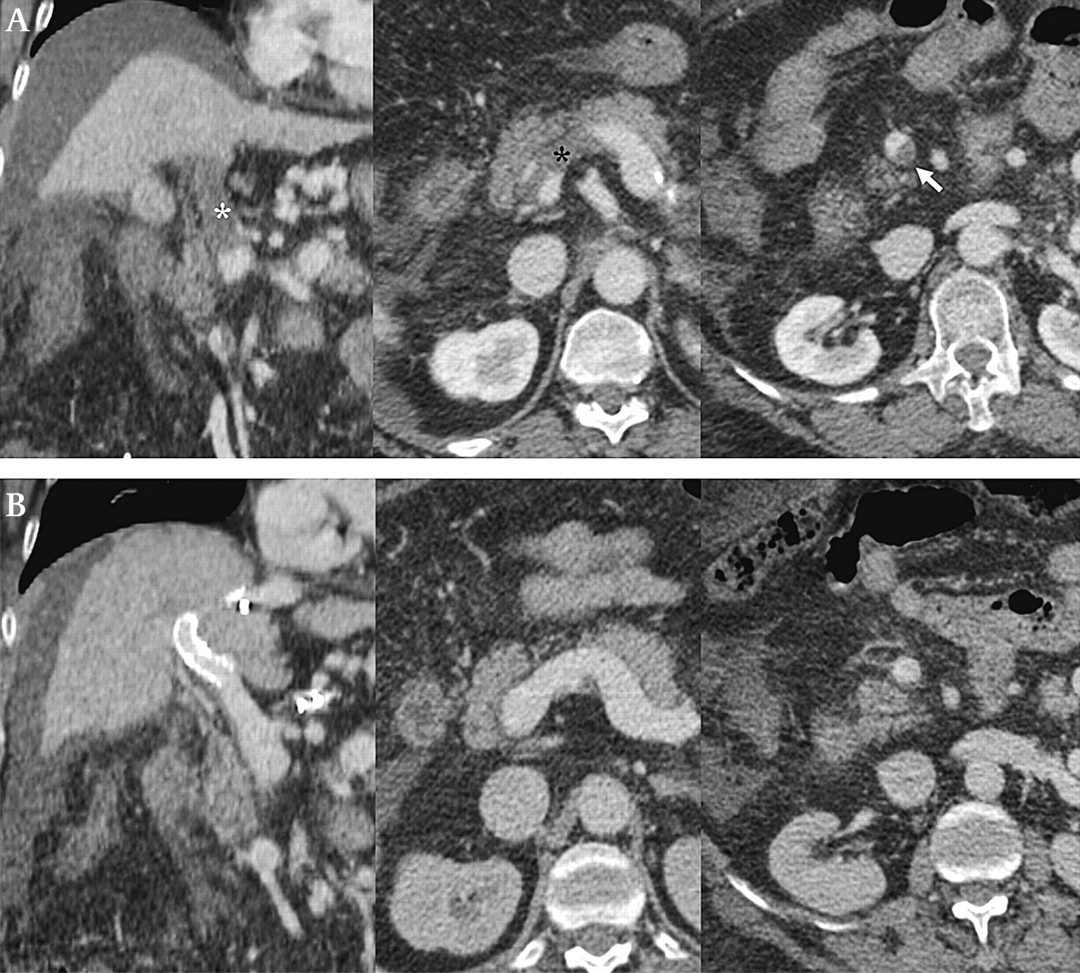
After TIPS implantation the portal venous system was completely recanalised in 40 (57%) patients, and a marked decrease in thrombosis was observed in 21 (30%), while no improvement was observed in nine (13%) (table 4, figure 2).
Changes in portal vein thrombosis after TIPS implantation
{kind=link}
{kind=link}
(A) MDCT shows severe and extensive PVT with lumen occupancy of the MPV of 100% (white star), SMV 50% (white arrow) and splenic vein 100% (black star). (B) 36 days after TIPS placement, MDCT shows complete recanalisation. MDCT, multidetector computed tomography; MPV, main portal vein; PVT, portal vein thrombosis; SMV, superior mesenteric vein; SV, splenic vein; TIPS, transjugular intrahepatic portosystemic shunt.
In 40 patients with complete recanalisation of the portal venous system, the rate of recanalisation at 6, 12 and 24 months was 53%, 70% and 99%, respectively. Thirty-eight (95%) patients with complete recanalisation after TIPS placement maintained a patent portal vein at a mean follow-up of 20.7 months. Two (5%) patients experienced recurrence of thrombosis, one at 6 months, and the other at 26 months of follow-up. One of these two patients had four associated prothrombotic disorders, while none had TIPS dysfunction. In 21 patients with partial recanalisation of the PVT, the mean decrease in lumen occupancy of the MPV, SMV and SV was 36%, 37% and 17%, respectively. In 12 (57%) of these patients, there was a decrease in the number of venous segments with thrombosis. In all series, the rate of complete recanalisation of the portal venous system at 6, 12 and 24 months was 36%, 51% and 81%, respectively.
Multivariate analysis showed that independent predictors for complete recanalisation after TIPS placement were thrombosis of a single vein at inclusion (HR 2.45, 95% CI 1.17 to 5.14), PVT severity of grade I (HR 2.97, 95% CI 1.18 to 7.50), de novo diagnosis of PVT (HR 2.97, 95% CI 1.18 to 7.50), and absence of gastro-oesophageal varices (HR 14.99, 95% CI 2.81 to 79.81). Ascites, variceal bleeding, number of thrombotic risk factors, time from diagnosis of PVT to TIPS placement, INR, platelet count, and stent diameter, were not significantly different at univariate and multivariate analysis.
Complications and survival
One patient had migration of the stent in the MPV during the procedure, though this patient was transplanted 5 months later without any complications. No other major procedure-related complications were observed.
Eight weeks after TIPS placement, there was an increase in the MELD score (from 11.4 to 14.7, p<0.001) while the Child–Pugh score did not change significantly (from 8.0 to 8.5, p=0.16). In the long-term follow-up, one patient had recurrence of bleeding from gastric antral vascular ectasia, and two had SBP. The rate of encephalopathy at 12 and 24 months was 27% and 32%, respectively. The rate of TIPS dysfunction at 12 and 24 months was 38% and 85% for bare stent, and 21% and 29% for covered stent (p<0.001), respectively. The rate of admissions for liver decompensation at 12 and 24 months was 24% and 39%, respectively. No patient had clinical evidence of pulmonary embolism.
Survival rates at 1, 12 and 24 months were 99%, 89% and 81%, respectively. Ten patients died during follow-up as a result of progressive liver failure (n=8), or unrelated diseases (one arterial bleeding, one myocardial infarction). Fifteen patients underwent liver transplantation. Of the remaining 45 patients who are alive without a liver transplant, 15 remain on the transplant list, 28 have not been listed because of stable liver disease, and two dropped out at 3 weeks and 23 months of follow-up, respectively (table 5).
Follow-up data in 70 patients with cirrhosis and with portal vein thrombosis (PVT), who underwent transjugular intrahepatic portosystemic shunt
Discussion
In our study, 32% of the patients with cirrhosis had non-tumoural PVT. This number is higher than that reported in the literature (1–25%),1–7 which may be due to factors such as patient selection, inclusion of cases with non-occlusive PVT, and use of second-level techniques for the diagnosis of PVT. Actually, most of our patients had advanced liver disease, as evidenced by the fact that 76% were Child–Pugh B–C class, 83% at stage IV according to the clinical stage classification,24 and 53% were listed for liver transplantation. Previous studies have correlated the severity of cirrhosis with a higher risk of PVT, which may reflect the thrombophilic tendency shown in association with advanced cirrhosis.4 6–8 Our study clearly demonstrates that TIPS is effective for the treatment of PVT in patients with cirrhosis. Fifty-seven per cent of cases had complete resolution of thrombosis, 30% had reduction in lumen occupancy and/or extension of thrombosis, and only 13% remained unchanged. Among patients who had complete resolution, only two (5%) had recurrence of PVT during the follow-up, indicating that the marked increase in portal flow velocity induced by TIPS overcomes all other prothrombotic factors that may be present. We studied some of the more common prothrombotic factors in 38 patients and found that 45% of those patients with PVT had at least one concomitant congenital thrombofilic condition. Similar results have been reported by others.6 7 The fact that TIPS achieved and maintained a high rate of recanalisation despite the presence of this state of hypercoagulability strongly suggests that the decrease of portal flow is the most important determinant of portal vein thrombosis in cirrhosis. The results of our study are supported by a prospective cohort study demonstrating that a low portal blood flow velocity detected by Doppler ultrasound at the initial evaluation of cirrhotic patients is the only factor that independently predicts the occurrence of PVT over course of follow-up.6
This is not the first report showing the beneficial effects of TIPS on PVT in patients with cirrhosis, but is the largest series.14–21 In addition, the diagnosis of PVT was made by using MDCT and/or MRA rather than by ultrasound or identification in the operating room at the time of liver transplant. To the best of our knowledge, only one study has appraised changes on PVT prior to and after TIPS placement using MDCT and/or MRA, but included only nine patients with cirrhosis who were candidates for liver transplantation.21 MDCT and MRA are more sensitive than ultrasound for diagnosing non-occlusive PVT, accurately estimating the percentage of lumen occupancy, and assessing the extent of thrombosis in the portal venous system.25 Notably, in 52 of the 67 (78%) patients with thrombosis of the MPV, the thrombus was extended to the SMV and/or splenic vein. Finally, MDCT and MRA are not influenced by the expertise of individual operators, are less susceptible to false-positive errors in cases of stagnant portal blood flow, and concur in excluding with reasonable certainty the malignant nature of PVT.26
A multivariate analysis showed that the independent factors that best predicted the complete resolution of PVT after TIPS placement were a less severe and extensive PVT, the diagnosis of de novo PVT, and the absence of gastro-oesophageal varices. The patients in whom PVT was diagnosed in the course of serial imaging screening for HCC (de novo PVT) responded better than those in which the thrombosis was already evident at the first imaging study (ex novo PVT), perhaps because the latter included those patients with long standing thrombosis. The importance of the length of the follow-up after TIPS placement is that, for reasons still unknown, recanalisation occurs over an interval of time ranging from a few months to over a year.
In a previous series, in eight out of 19 patients who underwent TIPS insertion, the stent was extended across the thrombus into the MPV because the clot remained adherent, and the flow was poor after mechanical thrombolysis and local heparin.19 Our data suggest that a more conservative attitude is highly effective and probably safer, as stenting the MPV may complicate subsequent liver transplant surgery.
It is important to note that our good results with TIPS placement were achieved without using thrombolytic or anticoagulation therapy, either at the time of procedure, or during follow-up. Anticoagulant therapy has been used successfully for the treatment of PVT in patients without chronic liver disease,13 and it has recently been suggested for the treatment of non-tumoural PVT in patients with cirrhosis.5 27 However, immediately after TIPS, thrombolytic and anticoagulation therapy can be dangerous, as suggested by the fact that in a previous study one out of 12 patients with cirrhosis treated with anticoagulation after TIPS placement died of haemorrhagic complications 2 days after the procedure.19
In our series the technical success of TIPS insertion was 100%, with no procedure-related mortality. The only procedure-related complication was the migration of a stent in the MPV, though this had no clinically significant consequences, as the patient later underwent liver transplantation with no complications. Interestingly, there was no incidence of clinically evident pulmonary embolism after TIPS placement, but pulmonary angiography was not performed after TIPS placement and, therefore, we can not exclude asymptomatic episodes of pulmonary microembolism.
However, lesser technical success and higher rates of procedure-related complications and mortality in this population have been reported.14 19 20 28 These differences are probably attributable to the fact that other published series include more patients with cavernous transformation, while in our patients TIPS was not attempted in the case of portal cavernoma associated with fibrotic transformation of the MPV and/or its main branches.
In our experience, the risk of TIPS dysfunction, including thrombosis of the stent, and the risk of encephalopathy, was similar to that reported in patients without PVT.29–31 In addition, we had only one case of bleeding from gastric antral vascular ectasia, showing that the screening programme for early detection of TIPS dysfunction by Doppler ultrasound was effective. Fifteen patients underwent liver transplantation, and in none of these did the presence of TIPS or the residual thrombosis increase the technical difficulties of surgery or require non-conventional venous anastomosis.
This study has two main limitations. First, TIPS was performed because of clinical decompensation (prevention of rebleeding, refractory ascites or hydrothorax) in most patients and performed on the basis of PVT alone in only four patients. Nevertheless, this is the largest study in patients with cirrhosis and PVT and our results clearly show effectiveness and low risk of the procedure, suggesting that PVT could be a primary indication for TIPS placement. Second, the absence of control group, for instance anticoagulation or even abstention in patients with less severe thrombosis, does not provide an answer to the question of whether TIPS is best option in such patients, or whether it should be reserved for anticoagulation failures/contraindications or for patients with more severe PVT.
In conclusion, in patients with cirrhosis complicated by non-tumoural PVT, TIPS placement is a safe and effective therapeutic option, and is not associated with an increased risk of procedure-related complications, TIPS dysfunction, complications due to portal hypertension, or mortality. This may be especially valuable in patients eligible for liver transplantation in whom extension of the thrombosis may increase the risk of surgery. Prospective randomised studies should investigate whether TIPS placement is best therapeutic option in patients with cirrhosis who develop non-tumoural PVT.
Acknowledgments
The authors gratefully acknowledge the cooperation of Gaetano Florida in data collection, and documentation.
References
Footnotes
Competing interests None.
Ethics approval The study was approved by our institute's Internal Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.