Article Text

Abstract
Objectives Colonoscopy is central to colorectal cancer (CRC) screening. Success of CRC screening is dependent on colonoscopy quality. The NHS Bowel Cancer Screening Programme (BCSP) offers biennial faecal occult blood (FOB) testing to 60–74 year olds and colonoscopy to those with positive FOB tests. All colonoscopists in the screening programme are required to meet predetermined standards before starting screening and are subject to ongoing quality assurance. In this study, the authors examine the quality of colonoscopy in the NHS BCSP and describe new and established measures to assess and maintain quality.
Design The NHS BCSP database collects detailed data on all screening colonoscopies. Prospectively collected data from the first 3 years of the programme (August 2006 to August 2009) were analysed. Colonoscopy quality indicators (adenoma detection rate (ADR), polyp detection rate, colonoscopy withdrawal time, caecal intubation rate, rectal retroversion rate, polyp retrieval rate, mean sedation doses, patient comfort scores, bowel preparation quality and adverse event incidence) were calculated along with measures of total adenoma detection.
Results 2 269 983 individuals returned FOB tests leading to 36 460 colonoscopies. Mean unadjusted caecal intubation rate was 95.2%, and mean withdrawal time for normal procedures was 9.2 min. The mean ADR per colonoscopist was 46.5%. The mean number of adenomas per procedure (MAP) was 0.91; the mean number of adenomas per positive procedure (MAP+) was 1.94. Perforation occurred after 0.09% of procedures. There were no procedure-related deaths.
Conclusions The NHS BCSP provides high-quality colonoscopy, as demonstrated by high caecal intubation rate, ADR and comfort scores, and low adverse event rates. Quality is achieved by ensuring BCSP colonoscopists meet a high standard before starting screening and through ongoing quality assurance. Measuring total adenoma detection (MAP and MAP+) as adjuncts to ADR may further enhance quality assurance.
- Colonoscopy
- screening
- adverse events
- colorectal cancer
- quality
- screening
- colonic polyps
- colonoscopy
- colorectal adenomas
- therapeutic endoscopy
- colonic adenomas
- chromoendoscopy
- IBD clinical
- colorectal cancer screening
- inflammatory bowel disease
- colorectal carcinoma
- helicobacter therapy
- iron deficiency
- epidemiology
Statistics from Altmetric.com
- Colonoscopy
- screening
- adverse events
- colorectal cancer
- quality
- screening
- colonic polyps
- colonoscopy
- colorectal adenomas
- therapeutic endoscopy
- colonic adenomas
- chromoendoscopy
- IBD clinical
- colorectal cancer screening
- inflammatory bowel disease
- colorectal carcinoma
- helicobacter therapy
- iron deficiency
- epidemiology
Significance of this study
What is already known about this subject?
Concerns have previously been raised regarding the quality of colonoscopy in England.
A number of strategies over the last 10 years have aimed to improve the quality of colonoscopy.
Adenoma detection rate (ADR) is widely used as the key indicator of colonoscopic quality.
What are the new findings?
A large national screening programme can deliver high standards of colonoscopy quality and safety.
Variation in colonoscopic performance exists within the programme.
ADR is an important marker of colonoscopic practice; however, measures of total numbers of adenomas detected (mean adenomas per procedure (MAP) and mean adenomas per positive procedure (MAP+)) provide additional information.
How might it impact upon clinical practice in the foreseeable future?
Quality of colonoscopy should be assessed in three domains: technical quality, patient safety and patient experience.
Assessment of MAP and MAP+ in addition to ADR provides additional information about colonoscopy performance.
Colonoscopy adverse events should be stratified according to severity for quality assurance purposes.
These data can be used to inform patient consent and procedure-related risk.
Investigation of the factors accounting for variations in colonoscopic practice is required to minimise these variations in the future.
Introduction
Screening for colorectal cancer (CRC) is undertaken in many countries worldwide. One widely used strategy is biennial faecal occult blood (FOB) testing followed by colonoscopy for those with a positive FOB test.1 The main aim of CRC screening is to reduce mortality by early detection and treatment of cancer. A secondary aim is to detect and remove adenomas in order to prevent progression to cancer. Adenoma detection is known to vary widely both between and within screening programmes.2–6 Much of this variation may be explained by factors relating to quality of the colonoscopy. The importance of ensuring high-quality colonoscopy within screening programmes has been emphasised in a number of recent studies and guidelines.7–9
Adenoma detection rate (ADR) is a widely used indicator of colonoscopy quality10; it is a marker of both the technical quality of the procedure and the efficacy of the screening strategy. Other domains of quality assessment including safety and patient experience are also crucial. A UK audit of colonoscopy published in 2004 raised concerns about the quality of colonoscopy in the UK, showing caecal intubation in only 76.9% of 9223 procedures and an overall perforation rate of 1:769.11 Measures have been introduced in the UK over the last decade to improve the quality of colonoscopy. These include a national endoscopy training programme, defined parameters for endoscopy training coordinated by the Joint Advisory Group on Gastrointestinal Endoscopy and national endoscopy standards (defined by the Global Rating Score). Clear standards and accreditation of colonoscopists for bowel cancer screening were developed.
In this study we use quality indicators to examine the quality of colonoscopy delivered within the NHS Bowel Cancer Screening programme (BCSP).
Methods
Screening programme
The NHS BCSP started in England in August 2006. During the study period, adults aged between 60 and 69 years were offered FOB testing on a biennial basis using a non-rehydrated guaiac-based test. Adults over 70 years were able to opt-in to the programme on a voluntary basis. The upper age limit for invited screening was extended to 74 years in January 2010. Individuals with a positive FOB test were offered colonoscopy.
FOB screening is coordinated by five ‘hubs’ around England; eligible people are identified from general practice registers. FOB test kits are sent by mail with instructions to be returned within 3 months. A non-rehydrated guaiac-based FOB test (Hema-screen; Immunostics Inc, Ocean, New Jersey, USA) is used. Colonoscopy is recommended for either an ‘abnormal’ FOB test (five or six positive windows) or after repeat FOB testing (if the initial test has one to four positive windows and subsequent testing is positive). Those with positive FOB tests are offered an appointment with a nurse, at which the screening process is explained and colonoscopy is offered. If the person accepts the offer of colonoscopy, they are offered an appointment for colonoscopy within 2 weeks. Individuals give pre-procedure consent and are given explicit instructions on use of bowel preparation. Bowel preparation is performed in accordance with local guidelines, which may vary between screening centres and hospital sites. Colonoscopy and subsequent management is coordinated by 54 screening centres around the country which work with the screening hubs in a ‘hub and spoke’ structure.
Before starting to practise in the BCSP, all colonoscopists are required to have performed at least 1000 colonoscopies in their career with a caecal intubation rate (CIR) above 90% and an ADR above 20% in the preceding 12 months. In addition, sedation levels have to be in keeping with National Patient Safety Agency recommendations and British Society of Gastroenterology guidelines, and complication rate has to be reported and deemed acceptable.12 13 Completion of an accreditation examination at an independent unit is undertaken; this consists of a multiple choice question examination and performance of two colonoscopies observed by two independent and trained examiners using objective directly observed colonoscopic procedural skills assessment criteria.14 Accredited colonoscopists are subject to ongoing audit of colonoscopic performance.
For the purposes of quality assurance within the screening programme, extent of colonoscopy, quality of bowel preparation, patient comfort, colonoscope withdrawal time, and rectal retroversion are recorded at the time of colonoscopy by a dedicated screening nurse present in the endoscopy room for the entire procedure. All polyps removed in the study period were sent for histopathological examination by an accredited BCSP pathologist and laboratory.
All demographic, colonoscopic and histopathological data were recorded by the screening centre on a national database (Bowel Cancer Screening System (BCSS)). Adverse events were recorded on the BCSS, reported to the national office of the BCSP, and verified by direct contact with each screening centre.
Study procedures
Specific searches of the national database (BCSS) were designed to provide data to calculate each quality indicator. Missing data, where possible, were recovered from screening centres and included in the calculation of quality indicators. Data quality in the database was generally good for the data required for this study, with over 98% completeness in the majority of fields. Audits comparing BCSS data with locally held records were performed, demonstrating satisfactory accuracy. Entries in the database which appeared clinically implausible, as adjudicated by panel decision, were excluded from further analysis (table 1).
Limits for considering data implausible
The prevalent round of screening was defined as the first 2 years after the start of screening at each centre. Any screening colonoscopies performed after 2 years were considered to be in the first incident round. Approval of this work as service evaluation was obtained from a regional ethics committee.
Quality indicators
Ten quality indicators were identified and defined for the purpose of evaluating colonoscopy in the NHS BCSP. These indicators, their definitions and level of accountability are shown in table 2.
Colonoscopy quality indicators
Where quality indicators were calculated as an average per colonoscopist or screening centre, only those having performed over 50 procedures were included in analysis.
In general screening terms, the ADR can be referred to as the positive predictive value for adenoma(s)—that is, the proportion (%) of people undergoing colonoscopy with one or more adenomas. To avoid double-counting of adenomas, only first screening colonoscopies were included in the analysis. Measures of neoplasia detection, other than ADR, may provide additional information for quality assessment of colonoscopy. Other measures include polyp detection rate (PDR, number of colonoscopies at which one or more polyps (regardless of removal or histological subtype) were found divided by the total number of colonoscopies), mean adenomas per procedure (MAP, total number of adenomas detected divided by the number of procedures) and mean adenomas per positive procedure (MAP+, total number of adenomas detected divided by the number of procedures in which one or more adenomas were detected). The role of PDR, MAP and MAP+ in assessing the quality of colonoscopy is less clear than that of ADR; we therefore calculated PDR, MAP and MAP+ for each colonoscopist and compared the measures with ADR using tests of correlation.
Colonoscopy withdrawal time (CWT) was recorded (to the nearest whole minute) by a nurse at the time of colonoscopy. Only complete, negative procedures were included in analysis to remove the impact of therapeutic manoeuvres on the procedure duration. Mean negative complete withdrawal time (nc-CWT) was calculated per colonoscopist.
Caecal intubation was recorded at the time of colonoscopy and based on the colonoscopist's assessment of extent of intubation using anatomical landmarks. Unadjusted caecal intubation rate (uCIR) was calculated on an intention to reach the caecum basis: no adjustment for pathology, strictures or bowel preparation quality was made. Obtaining photographic evidence of caecal intubation is stipulated in the BCSP, but was not reviewed for the purposes of this study. In order to be considered satisfactory indicators of colonoscopy quality, technical factors such as uCIR, CWT, RRR and PRR should correlate with ADR. The relationships between ADR and these factors were assessed.
Adverse events were defined as those that prevented completion of the planned procedure (excluding technical failure or poor preparation) or resulted in admission to hospital, prolongation of existing hospital stay, another interventional procedure or subsequent medical consultation.15 Adverse events were classified in terms of severity according to a stratification tool defined by the BCSP Quality Assurance Guidelines for Colonoscopy (online appendix 1).15 This tool is based on a report from the ASGE workshop on colonoscopy-related adverse events.16 In order to capture all adverse events, patients were encouraged to contact their local screening centre if any problems arose after discharge. In addition, a questionnaire that specifically requested information on any adverse events experienced was sent to all patients 30 days after their procedure. Records of colonoscopy-related adverse events were obtained from two sources (interrogation of the BCSS database and analysis of the log of adverse events reported to the national office). These were validated against locally held records of adverse events at each screening centre, which were examined in a national survey of adverse events.
Statistical analysis
Continuous variables are presented as mean (range). Categorical variables are presented as a proportion (%). Where categorical variables are summarised for the whole sample, a mean proportion (%) and a range of individual proportions are presented (eg, ADR for all colonoscopists (%), lowest ADR per colonoscopist—highest ADR per colonoscopist). Univariable analysis was undertaken using the two sample tests of proportions. Correlation of normally distributed continuous variables was assessed using Pearson's correlation coefficient (r). Correlation of non-parametric variables was assessed with the Spearman rank correlation coefficient (ρ). A p value of less than 0.05 was considered to be significant. All reported p values are two sided. All analyses were performed with Stata (V.10).
Results
Colonoscopy quality indicators
Between August 2006 and August 2009, 2 269 983 individuals completed FOB testing. Uptake of FOB testing was 52.9%, and 2.02% of FOB tests were positive. A total of 36 460 colonoscopies and 1708 sigmoidoscopies were performed by 177 different colonoscopists at 50 screening centres. The mean age of patients undergoing colonoscopy was 66.0 years (range 60–92); 61.6% were male. A total of 3848 cancers were detected at colonoscopy, with a positive predictive value of colonoscopy (after positive FOB testing) for cancer of 10.6%.
Summary data for each of the quality indicators attributable to the colonoscopist are shown in table 3. The denominator is different for each indicator because of different definitions of eligible procedures and differences in missing or implausible data between each variable.
Summary data for colonoscopist-attributable quality indicators
Adenoma detection rate
ADR per colonoscopist ranged from 21.9% to 59.8% with a mean of 46.5% (median 47.2%). ADR is a key metric for measuring quality of colonoscopy and may be used to compare two or more colonoscopists. It is therefore important to consider major confounding factors such as gender, age and screening round. It is known that adenomas are more common in men, and incidence increases with age.17 18 In our study, the mean ADR per colonoscopist was 52.9% in men and 36.5% in women (p<0.001). ADR was therefore standardised by gender (GS-ADR) to allow for variation in the proportion of men and women in the case-mix of a particular colonoscopist. For the majority of colonoscopists, these two measures (ADR and GS-ADR) were closely matched (mean difference between ADR and GS-ADR was −0.02, SD 0.93). Older patients in the screening population undergoing colonoscopy were more likely to have one or more adenomas. The ADR was 44.0% in patients <65 years of age compared with 48.2% in those age 65 or older (p<0.001). However, there was little variation in the average age of patients undergoing colonoscopy between colonoscopists (mean age 65.8 years, SD=0.6, range 64.2–67.9). The mean difference between the ADR and the age-standardised (AS-ADR) for all colonoscopists was 0.13 (SD 1.73). In addition, ADR and GS-ADR correlate strongly (r=0.99, p<0.001), as do ADR and AS-ADR (r=0.96, p<0.001). The crude ADR was therefore an adequate measure for the data presented here.
Analysis of ADR in colonoscopies occurring in the prevalent round (P-ADR) and in the first incident round (I1-ADR) was performed. The P-ADR in 28 607 prevalent round colonoscopies was 46.2% compared with 46.3% in 2882 incident round colonoscopies (p=0.90). Therefore no standardisation of ADR by screening round was required.
ADR per colonoscopist correlates positively with caecal intubation rate (ρ=0.203, p=0.013), mean nc-CWT (ρ=0.236, p=0.004) (figure 1), rectal retroversion rate (ρ=0.193, p=0.019) and polyp retrieval rate (ρ=0.241, p=0.003). No correlation between ADR and bowel preparation quality (per colonoscopist, ρ=0.086, p=0.300) or comfort score (ρ= −0.004, p=0.958) is seen; both these measures were subjectively assessed.

Scatterplots of negative complete colonoscopy withdrawal time (nc-CWT) and caecal intubation rate (CIR) against adenoma detection rate (ADR) per colonoscopist.
MAP and ADR were shown to be positively correlated (table 4), this is largely because 53.0% of people with one or more adenomas have only one adenoma. MAP+ correlates less well with ADR, as it is possible for a colonoscopist to have a MAP+ near or above the mean with a low ADR. The relationships between ADR, MAP and MAP+ are shown in figure 2.
Other measures of neoplasia detection at colonoscopy and their relationship with ADR
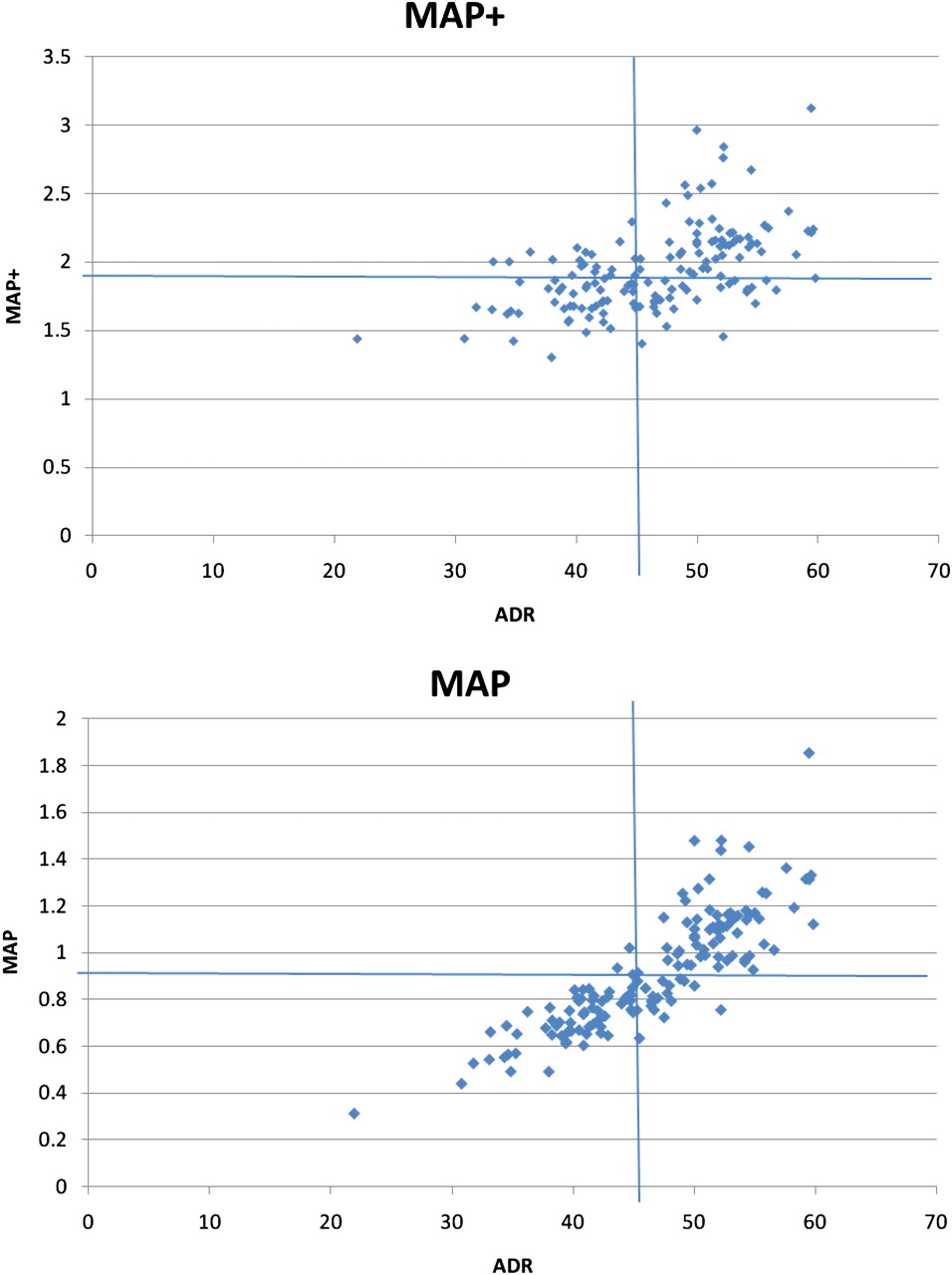
Scatterplots of mean number of adenomas per procedure (MAP) and mean number of adenomas per positive procedure (MAP+) against adenoma detection rate (ADR) per colonoscopist. Horizontal and vertical lines on the chart represent the respective means of the measures for the population.
Sedation practice, antispasmodic use, patient comfort and bowel preparation quality
Mean doses of the most commonly used benzodiazepine and opiate medications are shown in table 5 sub-grouped into under 70 years and 70 and over age groups. The mean percentage per colonoscopist of patients receiving no sedation was 14.1% (range 0–63.0%).
Mean sedative doses
Among colonoscopists who performed unsedated colonoscopy less often than the mean, 89.0% of procedures were associated with no, minimal or mild discomfort. This figure was 89.6% for colonoscopists who performed unsedated colonoscopy more commonly (p=0.62). Mean ADRs were the same in both groups (46.5%, p=0.97).
Entonox (nitrous oxide and air; BOC, UK) was used at least once, either alone or in combination with other medications, by 32 of 149 (21.5%) colonoscopists who had performed 50 or more procedures. Among these colonoscopists, 10.0% of procedures were performed with Entonox but no intravenous sedation (range 0.1–47.5%). Propofol was used at least once by 14/149 colonoscopists, accounting for 0.75% of procedures (range 0.1–2%). Use of reversal agent was rare, with flumazenil or naloxone used in 0.15% and 0.66% of procedures, respectively.
Hyoscine n-butyl bromide (Buscopan), used as an intravenous antispasmodic to aid visualisation of colonic mucosa, was used in more than 80% of procedures by 31 of 149 colonoscopists (20.8%). The mean proportion of procedures per colonoscopist in which Buscopan was used was 32.7% (range 0–98.1%).
Nurse-assessed patient comfort scores during colonoscopy were as follows: 64.3% (range 23.9–100%) of patients had no or minimal discomfort during colonoscopy; 24.9% (0–59.5%) reported mild discomfort; 9.6% (0–31.1%) reported moderate discomfort; and 1·3% (0–10.4%) reported severe discomfort.
The mean proportion of procedures in which the bowel preparation was excellent or adequate was 94.2% (range 81.5–100%).
Adverse events
All centres completed a detailed record of all adverse events. Table 6 shows the incidence of complications in the NHS BCSP. Adverse events were stratified according to their severity. Forty-nine major or intermediate severity bleeds occurred (0.13%); this excludes minor bleeds not requiring transfusion, intervention or prolonged admission (less than three nights). Thirty-five perforations occurred (0.09%). Ten other adverse events requiring admission for three or more nights or surgical intervention occurred (0.03%). These included two episodes of obstruction secondary to cancer, two splenic injuries requiring surgery, one stroke, two adverse reactions to bowel preparation, and three prolonged admissions due to pain. No deaths occurred as a result of screening colonoscopy.
Incidence of adverse events, classified according to the Bowel Cancer Screening Programme Quality Assurance Guidelines stratification tool
Discussion
This study demonstrates high-quality colonoscopy in the NHS BCSP. These data show that colonoscopy in a national screening programme can be delivered to a high standard while ensuring patient comfort and safety. These standards are achieved despite the BCSP being one of the largest CRC screening programmes in the world.1
The most widely used metric for assessing colonoscopy quality is ADR. Our study showed a mean ADR of 46.5%. This figure reflects the above average risk of detecting adenomas in people with a positive FOB test in the target age group. The ADR reported here is higher than in the pilot study of bowel cancer screening in the UK (37.1%, p<0.001).19 This difference may be explained by a number of factors including the age range of the screened population and progress in technical aspects of colonoscopy such as bowel preparation quality, improved equipment and advances in colonoscopic technique. The mean CWT for normal procedures and unadjusted CIR in our study are further evidence of the high technical quality of BCSP colonoscopy and compare favourably with other reports from large screening programmes.20 These data demonstrate an improvement in the quality of UK colonoscopy when compared with the 2004 national audit in which the unadjusted CIR was 76.9%.11 This improvement in colonoscopy quality in England supports the measures used by the Joint Advisory Group on Gastrointestinal Endoscopy and the BCSP in promoting and enhancing colonoscopy quality. A national audit of colonoscopy practice in England including non-screening colonoscopy is currently being undertaken, which will provide an up-to-date opportunity to compare performance indicators for screening and non-screening colonoscopy.21
Despite the overall high quality of colonoscopy demonstrated by this study, there is still considerable variation in ADR between colonoscopists. ADR per colonoscopist ranged from 21.9% to 59.8%, an almost threefold difference between the highest and lowest detecting colonoscopists. This variation persists when ADR is standardised for age and gender and is not due to sample size variation, as colonoscopists with less than 50 procedures were excluded. It is of interest that this variation exists in spite of the quality standards that colonoscopists must reach before starting screening colonoscopy. Variation is also seen in other technical quality indicators (nc-CWT, uCIR, RRR, PRR). Significant correlations between these measures and ADR were demonstrated. Further work is being undertaken to examine the relationship between markers of colonoscopic practice and adenoma detection in individual patients. Ongoing quality assurance work within the screening programme is needed to minimise variations in colonoscopic performance.
It is not known at present which processes will be most effective in minimising these variations, or indeed if it is possible for all colonoscopists to reach optimal standards.
We have shown that routine reporting of age, gender or screening round standardised ADR is not necessary; however, these methods remain useful for quality assurance purposes to investigate the effect of these variables if an individual colonoscopist is noted to have particularly low or high ADR. For instance, a colonoscopist who has had a larger proportion of women than the mean in their case-mix may have a lower non-standardised ADR.
We have examined the role of MAP and MAP+ in addition to ADR for assessing technical aspects of colonoscopy quality. ADR has an inherent limitation in that it does not measure the total number of adenomas detected. MAP and MAP+ are more aligned with the ethos of colonoscopy in the BCSP which, in addition to detecting cancer, is to detect and remove all adenomas. MAP and MAP+ may provide additional information about the performance of colonoscopists. The mean MAP for the population suggests that zero, one or two adenomas are found by most colonoscopies. The scatterplot of MAP against ADR in figure 2 identifies a group of colonoscopists who have an ADR around the mean but with a broad range of MAP. This shows that some colonoscopists are able to find more adenomas per patient than others, due to either underlying variation in adenoma prevalence or operator-based technical (or non-technical) skills of the colonoscopists themselves. MAP+ is not useful if the ADR is low; however, it provides extra information where ADR is high. The group of colonoscopists with a MAP+ over 2.5 and an ADR over 50.0% appear to be capable not only of detecting adenomas in high numbers of patients, but also of detecting multiple adenomas in these patients. We recommend that the BCSP routinely reports MAP and MAP+ in addition to ADR to give screening colonoscopists additional insight into their performance.
The adverse event rates in this study compare favourably with other published series, which report post-colonoscopy bleeding in 0.03–0.22% of procedures and perforation in 0.01–0.8% of procedures.19 22–24 The 2004 audit showed low complication levels, which have been maintained in this study. Given that 46.5% of procedures require at least one polypectomy and many involve removal of large and multiple polyps, the low levels of adverse events are notable.
No difference in ADR was seen between the prevalent and first incident screening rounds. This pattern was also seen in the pilot study of the screening programme.19 This is an important finding, as it helps predict future colonoscopic workload for the screening programme and also allows ADR to be used as a comparative quality indicator for colonoscopists who perform different proportions of prevalent and incident round procedures. Cancer detection rate, however, is known to be lower in subsequent incident rounds compared with the prevalent round.19 The fact that relatively small numbers of cancers are detected means that, while cancer detection rate is crucially important, it is not a sensitive measure of colonoscopy quality and tends to be dependent more on the underlying prevalence of CRC than technical skills attributable to the colonoscopist. For this reason, we have not reported cancer detection rate per colonoscopist in this study.
The guaiac-based FOB test screening protocol used by the BCSP is designed to achieve a yield for adenomas and advanced adenomas above that of the general population. This limits comparison of colonoscopy performance indicators reported in this study with other screening programmes using alternative screening modalities such as faecal immunochemical testing or flexible sigmoidoscopy, which may have different sensitivity and specificity for neoplasia detection.
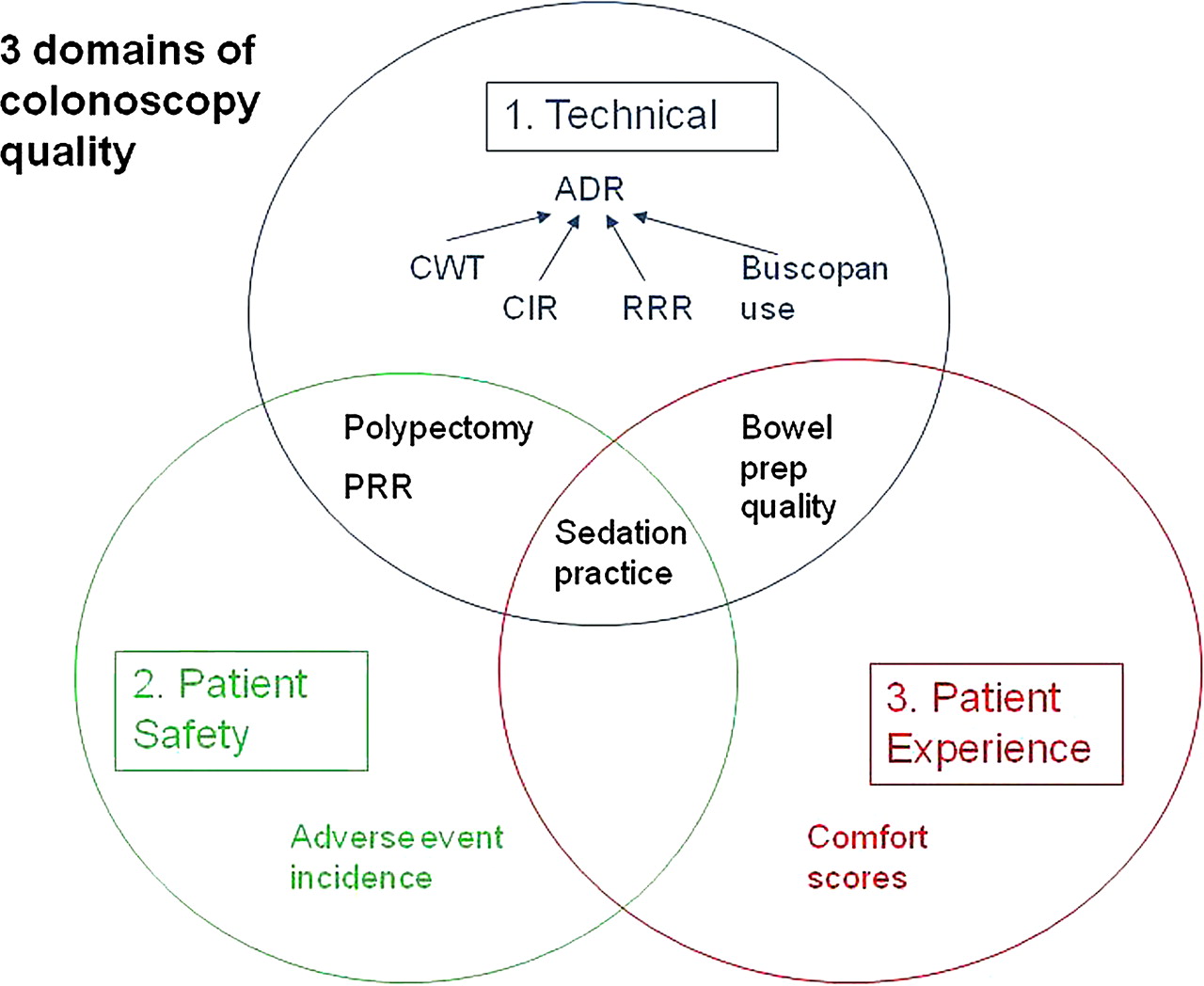
Any single quality indicator reported in this study would be insufficient in isolation to appraise the quality of colonoscopy. It is necessary to analyse a number of measures of quality, as summarised in the model in figure 3. The data presented in this study provide evidence to support the use of this model to assess quality of colonoscopy.
{kind=link}
{kind=link}
{kind=link}
Three domains of colonoscopy quality assessment. ADR, adenoma detection rate; CIR, caecal intubation rate; CWT, colonoscopy withdrawal time; PRP, polyp retrieval rate; RRR, rectal retroversion rate.
An important strength of this study is its size, both in terms of the number of colonoscopies analysed and the nation-wide coverage of the programme. Many colonoscopy quality studies are either single centre or restricted to a small number of colonoscopists. These data show that a high level of colonoscopy quality can be achieved in a large programme. Nevertheless, our study has several limitations. First, data for all colonoscopies were not complete; however, complete datasets accounted for 98% of all data, and missing data did not cluster geographically or around individual colonoscopists. This level of missing data should have only a minor effect on the measured quality indicators. Quality of collected data is in itself a marker of quality of a screening programme, and feedback on data quality issues raised by this study will improve the future quality of the data collection process.25
Second, a number of the indicators relied on subjective assessments (patient comfort, bowel preparation quality) using non-validated scoring systems. This was necessitated by the absence of widely used, validated scoring systems for these measures. Common guidance on use of the scoring systems used for bowel preparation and patient comfort was given to all screening practitioners to standardise data collection. Incorporation of validated scoring systems for these measures into the BCSP colonoscopy quality assurance process is necessary.
Third, clinical outcome measures, such as interval cancers, were not measured. This study concentrated on measures of colonoscopy quality which can be recorded at or close to the time of colonoscopy. Further work is being undertaken to assess the incidence of interval lesions in the NHS BCSP.
To ensure ongoing high-quality colonoscopy in the BCSP, quality assurance guidelines have defined a number of auditable outcomes and quality standards.15 Auditable outcomes are defined as important indicators for which no clear standard exists (eg, the standard for perforation rate per colonoscopist is less than one per thousand colonoscopies). Quality standards are defined as an auditable outcome for which there is an evidence base that can support a minimum standard (table 7). These are designed to drive quality to higher standards while setting limits to identify suboptimal performance. The results presented here show that colonoscopic quality in the BCSP has exceeded these standards.
Minimum standards and targets for colonoscopy in the Bowel Cancer Screening Programme15
The incorporation of measures of total adenoma detection as targets in the quality assurance guidelines would emphasise the importance of these measures of quality. Based on the 90th centile of each measure, we would suggest a MAP of 1.20 and a MAP+ of 2.27 (provided that the ADR is satisfactory) as targets.
In summary, this large national study demonstrates high-quality colonoscopy in the NHS BCSP. The adverse event rate is low despite the need for therapy associated with high ADRs. Assessment of a range of quality indicators including measures of total adenoma detection is necessary to evaluate colonoscopy quality. Potential participants in screening programmes should be reassured that screening colonoscopy in the NHS BCSP is high quality, safe and well tolerated.
Acknowledgments
We gratefully acknowledge the contribution of all BCSP screening centres in England. We also thank data analysts, Kate Bruce and Neal Lilly. This paper was based on work commissioned by the national Bowel Cancer Screening Programme Evaluation Group. This paper was produced in conjunction with the Northern Region Endoscopy Group (NREG).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Competing interests None.
Ethics approval County Durham & Tees Valley 2 Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.