Article Text

Abstract
Objectives The aims of this study were to examine the pattern of changes over time in health status (HS) and quality of life (QoL) in the first year after hip fracture and to quantify the association between frailty at the onset of hip fracture and the change in HS and QoL 1 year later. The major hypothesis was that frailty, a clinical state of increased vulnerability, is a good predictor of QoL in patients recovering from hip fracture.
Design Prospective, observational, follow-up cohort study.
Setting Secondary care. Ten participating centres in Brabant, the Netherlands.
Participants 1091 patients entered the study and 696 patients completed the study. Patients with a hip fracture aged 65 years and older or proxy respondents for patients with cognitive impairment were included in this study.
Main outcome measures The primary outcomes were HS (EuroQol-5 Dimensions questionnaire) and capability well-being (ICEpop CAPability measure for Older people). Prefracture frailty was defined with the Groningen Frailty Indicator (GFI), with GFI ≥4 indicating frailty. Participants were followed up at 1 month, 3 months, 6 months and 1 year after hospital admission.
Results In total, 371 patients (53.3%) were considered frail. Frailty was negatively associated with HS (β −0.333; 95% CI −0.366 to −0.299), self-rated health (β −21.9; 95% CI −24.2 to −19.6) and capability well-being (β −0.296; 95% CI −0.322 to −0.270) in elderly patients 1 year after hip fracture. After adjusting for confounders, including death, prefracture HS, age, prefracture residential status, prefracture mobility, American Society of Anesthesiologists grading and dementia, associations were weakened but remained significant.
Conclusions We revealed that frailty is negatively associated with QoL 1 year after hip fracture, even after adjusting for confounders. This finding suggests that early identification of prefracture frailty in patients with a hip fracture is important for prognostic counselling, care planning and the tailoring of treatment.
Trial registration number NCT02508675
- hip fracture
- frailty
- quality of life
- elderly
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study addresses the paucity of knowledge on frailty in elderly patients with a hip fracture.
This multicentre, prospective cohort study included a large number of subjects.
Patients and proxy participants from different geographical locations were included, which increases the generalisability of this study.
Participants may not accurately recall their health status prior to the fracture, which might affect the results.
The frail group contained more no-show cases, which could have resulted in selective dropout.
Introduction
A hip fracture is a serious event in the elderly population. It is associated with high mortality, morbidity and disability for those who survive.1–3 Hip fracture risks rise exponentially with increasing age. With the rising longevity across the globe, it seems reasonable that hip fractures will remain an important global health problem with substantial socioeconomic costs.4 5 A hip fracture has a major impact on health status (HS) and quality of life (QoL).6 HS represents the perceived impact of a disease on the level of patients’ physical, emotional and social functioning.7 Several factors are negatively associated with HS in elderly patients with a hip fracture, including female gender, comorbidity, poor nutritional status, severe postsurgical pain perception, long duration of hospital stay, postoperative complications, and low physical or psychosocial functioning at prefracture, including cognitive dysfunction.6 QoL is a multidimensional concept including both positive and negative aspects of life, and it measures patients’ evaluation of functioning in line with their expectations.8 QoL in older people is limited by an individual’s loss of ability to pursue different attributes with regard to attachment, role, enjoyment, security and control.9 This multidimensional concept can be measured with a capability well-being instrument in frail older adults following a hip fracture.10 11
Inconclusive evidence was found for the predictive value of older age.6 However, ageing is associated with a decline in physiological reserves, which impedes the body’s ability to withstand and recover from major and minor challenges, for example, a hip fracture. This phenomenon is defined as frailty, a clinical state of increased vulnerability, and it interacts with psychological factors, such as emotional state, coping style and sociological state.12
A systematic review from Lin and colleagues13 demonstrated that frailty is associated with adverse outcomes in older postsurgery patients, including prolonged length of stay, complications and postoperative mortality.1However, the relationship between frailty and HS, and between frailty and capability well-being, is unknown. The aims of this study were to (1) compare HS by frailty status at the time of hip fracture, (2) describe the patterns of HS and capability well-being in the first year after hip fracture, and (3) quantify the association between frailty at the onset of hip fracture and the patterns in HS and capability well-being 1 year following a hip fracture. We hypothesised that frail hip-fractured patients would experience a higher likelihood of poor HS and capability well-being, even after accounting for traditionally measured clinical risk factors.
Materials and methods
Study design and participants
The Brabant Injury Outcome Surveillance (BIOS), a multicentre, prospective, observational, follow-up cohort study, was conducted to obtain data at 1 week and at 1, 3, 6 and 12 months after hip fracture. Full details of the study, objectives and methods are described in detail elsewhere.14 This report has been prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.15
All participants were included between August 2015 and November 2016 from the 10 participating Dutch hospitals and were invited during hospital admission or within several days post-trauma by mail. Both patients aged 65 years and older and proxy respondents for patients with cognitive impairment were eligible for inclusion. Proxy participants could participate from 1 month onwards. Exclusion criteria were as follows: (1) pathological hip fractures, (2) patients and proxy respondents being unable or unwilling to give written informed consent, and (3) patients with insufficient knowledge of the Dutch language.
Data collection
Baseline prefracture information (T0) was gathered 1 week or 1 month after hip fracture by self-reported or proxy-reported questionnaires. The following data were collected at baseline within 1 month after hip fracture: demographic characteristics (age, gender, educational level), American Society of Anesthesiologists (ASA) grading, mobility, degree of frailty and HS. All participants were followed up at 1 week (T1), 1 month (T2), 3 months (T3), 6 months (T4) and 1 year (T5) after hospital admission. At follow-up sessions, questionnaires were sent to the participant or proxy. In cases of no return, they were contacted by telephone several times. If this method failed, the participant or proxy was considered to be a non-responder at that follow-up time point.
Patient and public involvement
Patients were involved in the recruitment to and conduct of the study. In a small pilot before inclusion in the BIOS, patients were asked their findings about the questionnaire and outcomes. We made small adjustments and results were disseminated to study participants who want to receive information by a newsletter.
Outcome assessment questionnaires
The Groningen Frailty Indicator (GFI) questionnaire was used to identify elderly individuals as being frail. The GFI is a 15-item self-reported instrument and screens for the loss of function and resources in four domains of functioning: physical, cognitive, social and psychological (online supplementary file).16 The sum score of the GFI ranges from 0 to 15, with a score of ≥4 indicating frailty. The study of Peters et al 17 concluded that the GFI is a feasible, reliable and valid self-assessment in home-dwelling and institutionalised elderly people by detecting those at high risk for poor outcomes.1
Supplementary material 1
The score on the EuroQol-5 Dimensions (EQ-5D) is a measure of HS.18 The EQ-5D has two parts: Visual Analogue Scale (VAS), which measures self-rated health, and an instrument along five health domains related to daily activities, including mobility, self-care, usual activities, pain and discomfort, and anxiety and depression. A respondent’s EQ-VAS presents self-rated health on a vertical scale with two endpoints, that is, ‘best imaginable health state’ (100) and ‘worst imaginable health state’ (0). Each dimension consists of a three-level response: no problems, moderate problems or severe problems. A scoring algorithm is available by which each HS description can be expressed into an overall score using a published utility algorithm for the Dutch population. HS was assessed with the utility score (EQ-5D utility), ranging from 0 representing death to 1 for full health. A negative utility score indicates an HS worse than death. The Dutch tariffs were used for this study to calculate EQ-5D-3 Level preference weights.19 The EQ-5D has good measurement properties and could be used to measure outcomes for patients recovering from hip fracture.11
The ICEpop CAPability measure for Older people (ICECAP-O) provides a broad assessment of capability well-being as it measures an individual’s ability to ‘do’ and ‘be’ the things that are important in life.20 This index of capability focuses on well-being defined in a broader sense, rather than defined by health, and covers the following five attributes: attachment (love and friendship), security (thinking about the future without concern), role (doing things that make you feel valued), enjoyment (enjoyment and pleasure) and control (independence). These attributes are used to calculate a tariff between 0, meaning no capability, and 1, representing full capability. The ICECAP-O has been validated in different elderly populations, and for this study the population of Makai et al of posthospitalised older people in the Netherlands was used to compare scores.21 22 The questionnaire shows good convergent validity with health and well-being instruments and is able to discriminate between elderly individuals with various health profiles.21 23 24
Statistical analysis
The descriptive statistics of the cohort were presented as means with SDs for continuous variables and as numbers and percentages for dichotomous or categorical variables. Missing baseline characteristics and missing sum scores in EQ-5D and ICECAP-O were imputed according to multiple imputation, using the multivariate imputation by chained equations procedure.25 There were no variables with 5% or more missing values. The data set was imputed 15 times with 5 iterations. Patient demographics (age, gender) were compared between responders and non-responders. Univariate and multivariable linear regression models were used to compare HS by frailty status at time of hip fracture. To assess the association between frailty and QoL over 1 year, we used linear mixed model analyses for EQ-5D utility scores and ICECAP-O scores, and we used binary logistic mixed model analyses for domains of the EQ-5D. Multicollinearity was assessed with the variance inflation factor (VIF). After univariate analyses, we performed adjusted analyses in which confounders (prefracture HS, sociodemographic variables and comorbidity) were included in the model. Because the mortality of study participants caused dropout (loss to follow-up), we performed death-adjusted analyses to adjust for overly optimistic estimates of patient outcomes. According to Parsons et al 26, we assumed that the EQ-5D score ranges from zero to death; these observations were then carried forward to subsequent assessment occasions.26 Effects were expressed as regression coefficients (beta; β), ORs and adjusted ORs (aORs) with 95% CIs, representing the longitudinal association between frailty and HS and between frailty and capability well-being over time, reflecting both the within-subject and between-subject relationship.27 Statistical test results were considered significant at a level of p<0.05. Statistical analyses were performed in SPSS V.24.0 and R V.3.4.0 (The R Project for Statistical Computing).
Results
Study population
Figure 1 shows the flow diagram of study participants. Only patients who completed the prefracture questionnaire, including the GFI, were included in this study. No significant differences were found in patient demographics (age: p=0.215; sex: p=0.183) between responders and non-responders. In total, 696 patients were included, and 371 patients (53.3%) were considered frail. Table 1 shows patients’ characteristics and clinical parameters, divided into frail and non-frail participants. In total, the mean age was 80.3 years, and 70.4% of the sample were female. Furthermore, 216 (31.0%) proxy participants were included.
Demographic and clinical baseline characteristics of the cohort

Flow diagram of study participants. Participants who missed some of the measurements are indicated as ‘no show’. GFI, Groningen Frailty Indicator; T1, 1 week; T2, 1 month; T3, 3 months; T4, 6 months; T5, 1 year.
The longitudinal association between frailty and HS
There were significant differences in HS between frail and non-frail patients during all follow-up time points (p<0.0001; figure 2). Prefracture frailty was associated with prefracture HS, adjusted for residential status as a confounder (β −0.29; SE 0.02; p<0.001; 95% CI −0.33 to −0.26).

Patterns of health status according to frailty status over time. EQ-5D, EuroQol-5 Dimensions.
The pattern of recovery trajectories in the prevalence of reported problems in the domains of the EQ-5D during the first year period after hip fracture differed between the frail and non-frail patients (figure 3A,B). For prefracture, a significantly higher proportion of patients in the frail group had problems with mobility, self-care and usual activities, and experienced more pain and signs of anxiety/depression (p<0.001; table 2). The percentage of patients with problems of anxiety/depression in the frail group was 54.7% at 1 week and 58.3% at 1 year, compared with 18.9% at 1 week and 14.2% at 1 year in the non-frail group. The aOR of the anxiety/depression domain revealed a 1.346-fold increase in problems (95% CI 1.045 to 1.734) experienced by frail patients over 1 year, compared with the problems in the non-frail group.
Mixed model analyses of change in EuroQol-5 Dimensions-3 Level for frail patients compared with non-frail patients over time
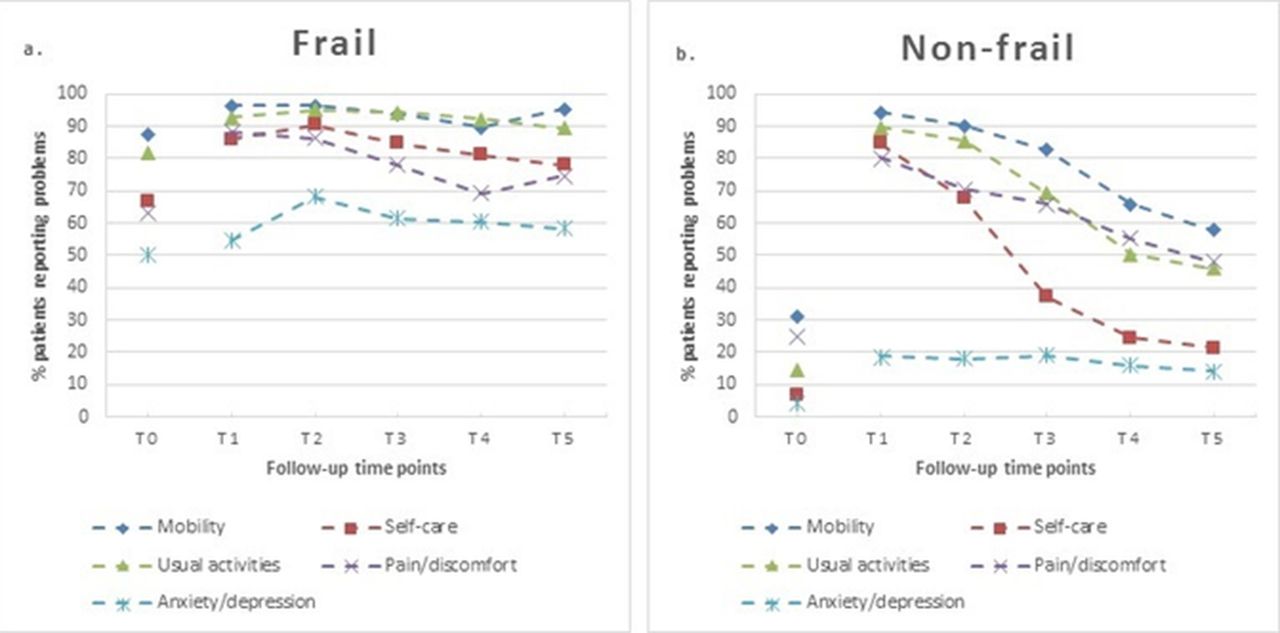
Percentage of frail (A) and non-frail (B) patients reporting problems on each EuroQol-5 Dimensions 3 Level. Questionnaire item at each follow-up time point.
The VIF before the final model analysis ranged from 1.23 to 1.69, indicating that there was no problem with multicollinearity. Frailty was negatively associated with HS (β −0.333; 95% CI −0.366 to −0.299) and self-rated health (β −21.9; 95% CI −24.2 to −19.6) in elderly patients 1 year after hip fracture (table 3). The estimated crude regression coefficient of −0.333 for frail patients in relation to HS can be interpreted as follows: a patient considered to be frail at baseline has a 0.333 lower EQ-5D utility score compared with non-frail patients. The regression coefficient was −0.115 (95% CI −0.160 to −0.069) for the association between frailty and HS, adjusted for deceased dropouts and for confounders, including prefracture EQ-5D score, age, prefracture residential status, prefracture mobility, ASA grading and dementia.
Analyses results on the association between frailty and health status/capability well-being over 1 year after hip fracture
The longitudinal association between frailty and capability well-being
Figure 4 shows differences in capability well-being between frail and non-frail patients during all follow-up time points (p<0.0001). We found a significantly strong negative association on average between frailty and capability well-being over time, with a death-adjusted regression coefficient that included all confounders of β −0.146 (95% CI −0.187 to −0.106; table 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patterns of capability well-being according to frailty status over time. ICECAP-O, ICEpop CAPability measure for Older people.
Discussion
Summary of results
It is well known that elderly patients with a hip fracture have poor QoL.6 However, it is unknown how much frailty affects patients’ QoL. This longitudinal cohort study shows that (1) frail patients with a hip fracture had poorer HS than non-frail patients at baseline, (2) frail patients had poorer HS and poorer capability well-being than non-frail patients over time, and (3) frailty at the onset of hip fracture was negatively associated with HS and capability well-being 1 year after hip fracture. The pattern of recovery trajectories in the prevalence of reported problems in the domains of the EQ-5D during the first year period after hip fracture differed between the frail and non-frail patients. However, after adjustment for confounders, especially for the concerned prefracture status of the EQ-5D domain, the major differences between frail and non-frail patients disappeared. Confounders, such as prefracture HS, age, prefracture residential status, prefracture mobility, ASA grading and dementia, also weakened the association between frailty and QoL, but the association remained significant and clinically relevant. Our findings demonstrate that prefracture frailty is significantly associated with poor HS, self-rated health and capability well-being the first year after recovery from hip fracture.
Comparison with existing literature
This study demonstrates that frailty is a common condition among elderly patients with a hip fracture. In our study, 53.3% of the patients with a hip fracture were considered frail. This finding is in line with that of a small pilot study of Kistler et al,28 who found that 51% of patients were considered frail.28 Previous studies, summarised in a systematic review by Lin and colleagues, showed frailty to be associated with adverse outcomes, such as prolonged length of stay and mortality in older surgical patients.13 This finding is in line with ours, showing a significant difference in length of stay between frail and non-frail patients (t(696)=−5.845, p<0.001). In line with the findings of Patel et al 29 and Dayama et al,30 we also found increased 1-year mortality rates in frail patients with a hip fracture. However, apart from these associations, our results showed that frailty is also negatively associated with QoL. This finding is of major importance because frailty seems to influence patients’ postoperative outcomes, such as mortality and complications, and has a perceived impact on the level of patients’ physical, emotional and social functioning. In the Netherlands, there is no difference in postfracture treatments between frail and non-frail patients. However, frail patients have already prefracture more problems with their mobility and self-care, and therefore this could have influenced their postfracture rehabilitation possibilities.
In our study, HS and capability well-being do not generally fully recover within 12 months after hip fracture for both frail and non-frail patients. This finding is in line with that of the prospective cohort study of Griffin et al,31 who also revealed an initial marked decline in HS after hip fracture, followed by improvement within 4 months and no return to baseline at 1 year after hip fracture.31 This is also in line with the International Costs and Utilities Related to Osteoporotic Fractures Study.32 33 However, in our study, we showed the pattern of QoL and distinguished between frail and non-frail patients. We revealed a significantly more prominent decline in HS, self-rated health and capability well-being for frail patients compared with non-frail patients the first year of recovery from hip fracture. To show that our findings are clinically relevant, Walters and Brazier34 published the minimum clinically important difference of 0.074 for the utility score of the EQ-5D.34
It is remarkable that in the non-frail group, a high percentage of individuals do not return to prefracture levels within a year on all domains of the EQ-5D. In particular, the domains mobility, pain and usual activities showed major differences between the percentage of non-frail patients and that of frail patients reporting problems at baseline and 1 year after hip fracture. However, the same did not apply to the EQ-5D domain anxiety and depression, which revealed a strong positive association between frailty and anxiety/depression. Until now, the literature revealed a prevalence rate of 10% of patients reporting depressive symptoms after hip fracture.35 Future research should provide insight into whether frailty is a predictor of psychological distress, characterised by symptoms of anxiety, symptoms of depression and symptoms of post-traumatic stress.
Limitations and strengths
This study had several limitations. First, participants may not accurately recall their status prior to the fracture, which might affect the results of the GFI and the EQ-5D at baseline. To minimise recall bias, the prefracture frailty status and HS data were only collected in patients included in the study until 1 month had passed. In addition, because of the length of the questionnaire, we did not ask the items of the ICECAP-O prior to the fracture, and we could not compare this longitudinal outcome with prefracture capability well-being. Second, frail patients showed a higher capability well-being score at 1-week follow-up than at 1-month follow-up. This is probably due to selection bias because frail patients in relatively good condition were able to complete the questionnaire at this early follow-up time point. Furthermore, there were more no-show cases in the frail group, which could have resulted in selective dropout. Therefore, the overall QoL of patients after a hip fracture, especially in the frail group, is probably worse than that presented in this study. On the other hand, an early follow-up time point at 1 week is unique in prospective research in hip fracture populations, and we adjusted for confounding variables in our mixed model analyses. Third, it is well known that surgery for hip fractures is frequently followed by complications.36 However, information about complications after hip fractures was not collected in this multicentre study, and complications could have affected patients’ QoL.
A strength of this study is the set-up in the form of a multicentre, prospective cohort study. We could include a large number of participants from different geographical locations, along with the possibility of including a wider range of hip fracture population groups, which increases the generalisability of this study. We also included proxy participants in case a patient was unable to participate in this study for several reasons, including cognitive impairment. Particularly, it is essential to include this group in this study because a major proportion of the frail group (41.2%) was suffering from dementia. Gabbe et al 37 published a study on trauma patients showing that differences in HS between patient and proxy respondents showed random variability rather than systematic bias. They concluded that group comparisons using proxy responses are unlikely to be biased. Another strength of this study is that we reported death-adjusted outcomes according to Parsons et al.26 When reporting QoL for patients after a hip fracture, excluding patients who die during follow-up leads to overly optimistic estimates of patient outcomes and is likely to cause bias.
Implication for clinical practice
The findings of this study support the hypothesis that prefracture frailty has an unfavourable effect on HS, self-rated health and capability well-being after a hip fracture. Preoperative frailty assessment can be valuable in informing patients and their relatives about the impact of hip fracture on patients’ physical, emotional and social functioning in the recovery period after a hip fracture. This frailty assessment could classify patients at high risk for unfavourable outcomes regarding poor QoL. It could support clinicians in tailoring treatment for medical decision making at an early phase. A clinically easy-to-use and universal frailty indicator, such as the GFI, could have important implications in prognostic counselling and care planning among older adults with hip fracture.
Conclusions
Our results show that frailty is negatively associated with patients’ QoL 1 year after hip fracture, even after adjusting for prefracture HS, age, prefracture residential status, prefracture mobility, ASA grading and dementia. This study highlights hip fracture as a major cause of burden and morbidity, especially in frail patients. This finding suggests that early identification of prefracture frailty in patients with a hip fracture is important for prognostic counselling, care planning and the tailoring of treatment.
References
Footnotes
Contributors CvdR, NK, LdM, TG and MACJ contributed to conception and design of this study. CvdR, MJFL, NK and LdM contributed to data collection. CvdR, MJFL, NK, LdM and MACJ contributed to analyses and interpretation. CvdR, MJFL, NK, LdM, JPJS, TG and MACdJ contributed to preparation of the manuscript. The final version of the article was approved by all the authors.
Funding This work was funded by a grant from the Netherlands Organisation for Health Research and Development (ZonMW; 842004005) TopCare projects section. This funding source did not play a role in the investigation.
Competing interests None declared.
Ethics approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study has been approved by the Medical Ethics Committee Brabant, the Netherlands (project number NL50258.028.14).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data could be shared after consultation with the BIOS study group.
Patient consent for publication Not required.