Article Text

Abstract
Objective Fever of unknown origin (FUO) can be caused by many diseases, and varies depending on region and time period. Research on FUO in Japan has been limited to single medical institution or region, and no nationwide study has been conducted. We identified diseases that should be considered and useful diagnostic testing in patients with FUO.
Design A nationwide retrospective study.
Setting 17 hospitals affiliated with the Japanese Society of Hospital General Medicine.
Participants This study included patients ≥18 years diagnosed with ‘classical fever of unknown origin’ (axillary temperature ≥38°C at least twice over a ≥3-week period without elucidation of a cause at three outpatient visits or during 3 days of hospitalisation) between January and December 2011.
Results A total of 121 patients with FUO were enrolled. The median age was 59 years (range 19–94 years). Causative diseases were infectious disease in 28 patients (23.1%), non-infectious inflammatory disease in 37 (30.6%), malignancy in 13 (10.7%), other in 15 (12.4%) and unknown in 28 (23.1%). The median interval from fever onset to evaluation at each hospital was 28 days. The longest time required for diagnosis involved a case of familial Mediterranean fever. Tests performed included blood cultures in 86.8%, serum procalcitonin in 43.8% and positron emission tomography in 29.8% of patients.
Conclusions With the widespread use of CT, FUO due to deep-seated abscess or solid tumour is decreasing markedly. Owing to the influence of the ageing population, polymyalgia rheumatica was the most frequent cause (9 patients). Four patients had FUO associated with HIV/AIDS, an important cause of FUO in Japan. In a relatively small number of cases, cause remained unclear. This may have been due to bias inherent in a retrospective study. This study identified diseases that should be considered in the differential diagnosis of FUO.
- INTERNAL MEDICINE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This study is the first nationwide study of patients with fever of unknown origin in Japan.
-
The present study identified diseases that should be considered in the differential diagnosis of fever of unknown origin.
-
The rate of ‘unknown’ in our study was relatively small, but this retrospective study may have encountered bias because of the difficulty of enrolling patients with an unknown cause after undergoing tests.
Introduction
Fever of unknown origin (FUO) can be caused by many diseases, and causes can vary depending on region and time period. FUO was first reported in the medical literature 80 years ago.1 Since then, the causative diseases have greatly changed with changes in the social environment and widespread use of diagnostic imaging.2–6
A few reports of FUO have also been published in Japan, but have been limited to single-facility or limited-region studies7 ,8; no nationwide studies have yet been conducted. Moreover, few assessments of tests used in the diagnostic evaluation of FUO have been reported. In particular, few studies have assessed the clinical usefulness of tests such as serum procalcitonin or positron emission tomography (PET) in Japan, although these tests are now frequently used.
We therefore conducted a multicenter collaborative retrospective study of patients with FUO at hospitals affiliated with the Japanese Society of Hospital General Medicine. This is the first nationwide study in Japan on diseases causing FUO and the diagnostic workup, and identified diseases that should be considered when evaluating FUO in Japan. In addition, we investigated the rate of performing various tests in the current diagnostic workup of FUO.
Methods
Among 99 hospitals affiliated with the Japanese Society of Hospital General Medicine that were asked to participate in this study, 17 hospitals participated. The hospitals participated in our study had a wide geographic distribution throughout Japan, including 7 hospitals in Eastern Japan and 10 hospitals in Western Japan. These 17 hospitals included 13 university hospitals and 4 community hospitals. Data were collected by these participating hospitals from patients ≥18 years who were diagnosed with ‘classical fever of unknown origin’ between 1 January and 31 December 2011. The data were recorded on standardised case report forms and were collected by fax.
Classical FUO was diagnosed based on the definition by Durack et al9 in patients meeting all of criteria 1–4 below.
-
Fever with axillary temperature ≥38°C at least twice over a ≥3-week period.
-
Unknown cause after three outpatient visits or during 3 days of hospitalisation.
-
Not diagnosed with immunodeficiency before fever onset.
-
No confirmed HIV infection before fever onset.
Axillary temperature is usually measured in Japan, so fever was defined as a temperature ≥38°C.
The data described below were collected. No additional testing was performed in this study due to insufficient data.
-
Patient characteristics: sex, age, concomitant disease, medical history and medication history.
-
Clinical findings: subjective symptoms and objective physical findings.
-
Blood tests: blood count, biochemical examination and inflammatory markers (C reactive protein (CRP), erythrocyte sedimentation rate (ESR), procalcitonin).
-
Results of blood cultures if performed.
-
Results of imaging studies and endoscopy if performed.
-
Results of cytology, histology, genetic testing or autopsy findings if performed.
-
Final diagnosis, day of diagnosis and outcome.
Results
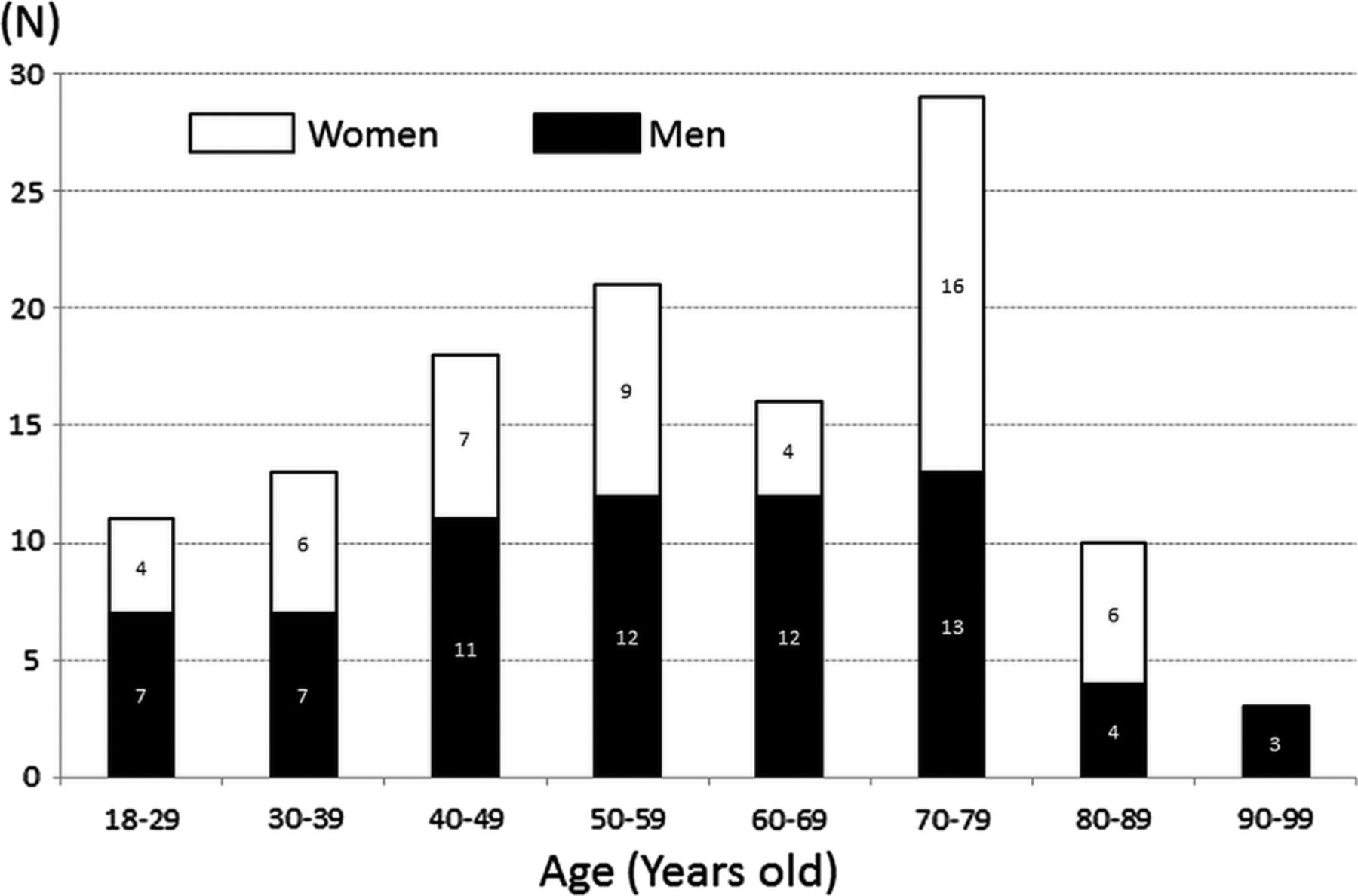
A total of 121 patients with FUO were enrolled at the 17 participating hospitals. There were 52 women (43.0%), and the median patient age was 59 years (range 19–94 years). The most frequent age group was patients in their 70s (figure 1). There were 112 patients from 13 university hospitals and 9 patients from 4 community hospitals.

Age and sex distribution of fever of unknown origin patients.
Causative diseases for FUO were infectious disease in 28 (23.1%) patients, non-infectious inflammatory disease (NIID) in 37 (30.6%), malignancy in 13 (10.7%), other in 15 (12.4%) and unknown in 28 (23.1%; figure 2). The most common causative disease was polymyalgia rheumatica (PMR; 9 patients), followed by malignant lymphoma (8 patients) and adult Still's disease (7 patients). Among the nine patients with PMR, coexisting giant cell arteritis was ruled out by PET in four patients and temporal artery biopsy in one patient. In the remaining four patients, symptoms and the success of treatment with low-dose steroids suggested PMR alone. Table 1 lists the frequent causative diseases. The prognosis in patients with undiagnosed FUO has been reported as relatively good.10 In our study as well, among 28 patients with undiagnosed FUO, only 3 died (10.7%). Among the three patients who died with undiagnosed FUO, one was a 72-year-old man who developed disseminated intravascular coagulation (DIC) 2 months after fever onset and died. Another was an 82-year-old man who similarly developed DIC of unknown cause 1 month after fever onset and died. The other was a 63-year-old woman in whom the cause of FUO remained unknown despite PET and random skin biopsies. This patient developed respiratory failure about 6 months after fever onset and died.
Frequent causes

Causative disease in fever of unknown origin. NIID, non-infectious inflammatory disease.
In patients ≥65 years (51 patients), malignancy as the causative disease was twice as common as in patients <65 years, and the cause remained unknown in only a few of these patients (figure 3).

(A) Causative disease in patients <65 years (70 patients). (B) Causative disease in patients ≥65 years (51 patients).
The median duration from fever onset to evaluation at each hospital was 28 days. Among the 24 patients requiring ≥100 days from fever onset until diagnosis, 10 patients (41.7%) had malignancy, exceeding the number with infection (7 patients, 29.2%; figure 4). Among patients with malignancy, 60% had malignant lymphoma. The longest time required for diagnosis was a case of familial Mediterranean fever, which required ≥2 years from the time of fever onset for diagnosis.

Causative disease in patients requiring ≥100 days until diagnosis (24 patients).
Tests performed for diagnostic evaluation included blood cultures in 86.8%, serum procalcitonin in 43.8%, gallium scintigraphy in 31.4% and PET in 29.8% of patients (figure 5). However, only 1 of 17 patients (5.9%) with a serum procalcitonin level ≥0.25 ng/mL showed bacterial infection and 3 patients (11.5%) with a value <0.25 ng/mL also had bacterial infection.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Frequency of tests performed for diagnostic evaluation. WCC, white blood cells count; CRP, C reactive protein; ESR, erythrocyte sedimentation rate; Ga, gallium; PET, positron emission tomography.
Nine deaths occurred among all 121 patients. The most common cause was malignant lymphoma, in four patients. Pathological autopsy was performed on a small proportion of the patients who died (n=2; 22.2%). The diagnosis was malignant lymphoma in both of these autopsied cases.
Discussion
Causative diseases underlying FUO vary by region and time period, and evaluation of these causes over a wide area using recent data is important. A previous study in Japan reported tuberculosis as the most common cause of FUO, accounting for 10% of cases.7 The present study identified NIID as the most common cause. Infections, including tuberculosis, were diagnosed based on appropriate culture or serological tests, before meeting the definition of classical FUO.
On the basis of the results of a survey conducted by the Organisation for Economic Cooperation and Development (OECD) in 30 member countries, Japan has 92.6 CT scanners and 40.1 MRI scanners per million population, the highest among OECD member countries.11 Because CT and MRI tend to be performed early after fever onset, FUO due to deep-seated abscess and solid tumours has decreased markedly. Among our 121 patients, the only deep-seated abscess was an ovarian abscess found in one patient, and the solid tumours were renal carcinoma in one patient and anal canal carcinoma in one patient only.
PMR was the most common disease causing FUO (9 patients) in the present study. This was probably influenced by the ageing of the Japanese population. According to data from the Ministry of Internal Affairs and Communications Statistics Bureau, among the total population in Japan of 127.34 million, 31.4 million (24.7%) are elderly persons ≥65 years, the highest number ever.12 In our study, 42.1% of patients were ≥65 years. A diagnosis of PMR, which occurs with a relatively high incidence in elderly patients, must thus be considered for FUO. Moreover, this trend should also be considered in Western countries, where ageing of the population is also expected. PMR had an influence, and when participants ≥65 and <65 years were compared, rates of NIID as a cause of FUO were similar (figure 3).
In Japan, 1529 new HIV infections were reported during 2011,13 and this increase in HIV-infected persons is continuing. Our study also found four patients with FUO caused by HIV/AIDS. The importance of HIV/AIDS as a cause of FUO will probably continue to increase in Japan. In our study, patients already diagnosed with HIV infections before meeting the definition of classical FUO were excluded.
Evaluations vary regarding the usefulness of ESR to diagnose FUO.6 Well-known diseases associated with ESR >100 mm/h include PMR, tuberculosis, multiple myeloma and osteomyelitis (vertebral discitis), but malignancies have also been reported in about 60% of such cases.14 In our study, 18 of 121 patients (14.9%) had an ESR of 100 mm/h, including 5 with unknown cause, 2 with PMR and 2 with ANCA-associated vasculitis.
When evaluating FUO, performing differential diagnosis for bacterial infections is important, given the need for prompt antibiotic therapy. It goes without saying that blood cultures are essential. In patients with bacteraemia given inappropriate treatment without performing blood cultures, the mortality rate has been reported as 3.18 times higher compared with patients with initial appropriate treatment. However, if treatment is switched based on blood culture results, the mortality rate is only 1.27 times higher.15
In recent years, the usefulness of serum procalcitonin in the differential diagnosis of bacterial infections has increasingly been reported, and serum procalcitonin is now in wide use in Japan. Simon et al reported that for differential diagnosis of bacterial infection from non-infectious disease, serum procalcitonin offers higher sensitivity (88%) and specificity (81%) than CRP (75% and 67%, respectively).16 In our study, serum procalcitonin was measured in 43.8% of patients. Although use of this test is widespread in Japan, 5.9% of patients with a serum procalcitonin level ≥0.25 ng/mL showed bacterial infection, and 11.5% of patients with a value <0.25 ng/mL also had bacterial infection. It is, therefore, difficult to conclude that serum procalcitonin is a superior test for the differential diagnosis of bacterial infection in patients with classical FUO. Serum procalcitonin testing is also more expensive than CRP or ESR testing, so indiscriminate measurement of serum procalcitonin in febrile patients should be avoided.
PET appears promising as a useful test to evaluate FUO. Many studies have been performed using this modality in patients with FUO, all showing a percentage helpfulness that exceeds that of CT, MRI or other diagnostic possibilities.17–20 However, the fact that PET is not covered by National Health Insurance in Japan for patients with FUO is problematic. A previous Japanese study about PET included patients with FUO evaluated by radiology departments.21 In the present study, it was interesting to see the frequency of PET use in general medical settings, mainly for evaluating FUO.
Previous studies have reported increasing rates of FUO in which the cause remains unknown.22 ,23 A prospective study from the Netherlands reported that the cause of FUO remained unknown in 51% of cases.6 The rate of ‘unknown’ in our study was relatively small, but this retrospective study may have encountered bias because of the difficulty enrolling patients with an unknown cause after undergoing tests. Furthermore, retrospective studies also encounter the problem that there may be no follow-up observation of patients until a final diagnosis has been obtained. We are planning a prospective study of patients who are enrolled at the time when criteria for FUO are fulfilled, to perform periodic follow-up observations. Only 17 hospitals participated in this study, so the results may not be generalisable to the overall situation in Japan. We hope that more hospitals will participate in future studies.
Conclusion
We conducted the first nationwide study of patients with FUO in Japan. Our study identified diseases that should now be considered in the differential diagnosis for FUO. This will be useful in future clinical practice. In addition, we identified tests that are performed during the FUO evaluation process at each hospital. This will serve as a reference for selecting diagnostic tests in the future. Guidelines should be created based on this type of study for future evaluation of FUO.
References
Footnotes
-
Contributors TN, MM, AU, NM, FO, SS, ST and JH conceived and designed the study. TN, MM, FM, KK, KT, SO, HM, AU, NM, FO, YO, NN, KM, KM, KA, KY and SS were involved in acquisition of data. TN, MM, FM, KK, KT, SO, HM, AU, NM, FO, YO, NN, KM, KM, KA, KY and SS analysed the data. TN, KT and MY wrote the manuscript.
-
Funding Grant-in-Aid from MEXT (Ministry of Education, Culture, Sports, Science and Technology) Supported Program for the Strategic Research Foundation at Private Universities, 2012–2017.
-
Competing interests None.
-
Ethics approval Research Ethics Committee of Juntendo University School of Medicine.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.