Article Text

Abstract
Introduction The British Thoracic Society (BTS) responded to a call from the pleural community to establish this new Training Standard to detail the capabilities in practice for thoracic ultrasound (TUS), which will build on the previous curricula and extend the remit to include training for the emergency provision of TUS.
Methods BTS convened a working group to produce a set of Training Standards.
Results This document provides a comprehensive Training Standard for TUS facilitating timely and improved management of patients with respiratory presentations, particularly (but not exclusively) pleural pathologies.
Discussion The Training Standards document will be widely disseminated.
- pleural disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The use of thoracic ultrasound (TUS) in the UK has evolved significantly since the National Patient Safety Alert in 2008, which identified a number of deaths and iatrogenic complications following the insertion of Seldinger chest drains.1 As a consequence bedside TUS at the time of intervention for pleural fluid has become mandatory, with the majority of TUS being performed by respiratory physicians following publication of the British Thoracic Society (BTS) Pleural Disease Guideline in 2010.2 3 Despite this evolution of TUS into respiratory medicine, the training curriculum used remains the Royal College of Radiologists (RCR) ‘Focused’ and ‘Level 1’ TUS for trainees and ‘level 2’ for trainers, adopted by the Joint Royal Colleges of Physicians Training Board (JRCPTB) Respiratory Medicine Curriculum (2014 amendments).4 5 This poses problems for respiratory trainees whereby Level 1 competence requires attendance at ‘at least one session per week over a period of no less than 3 months, with approximately five scans per session performed by the trainee’.6 Concern has been voiced by both trainers and trainees that this is difficult to achieve, particularly in many hospitals across the UK in which TUS occurs in an ad hoc or on-demand manner. Recent survey data have confirmed that trainees are highly unlikely to be able to meet this requirement within radiology departments.2 Furthermore, while time has allowed many centres to develop TUS trainers who have achieved Level 2 via Level 1 and 2 years experience, it is recognised that there are TUS capable respiratory physicians who have not met these criteria and are hence currently unable to act as trainers.
In addition to the impracticalities presented by the RCR curriculum, TUS experience is also being gained in other specialties such as intensive care medicine and acute medicine. While point-of-care ultrasound and its diagnostic use is not incorporated into the respiratory training curriculum, it is likely respiratory trainees will have exposure to this and will require guidance. Furthermore, while the shift to specialty ownership of TUS and pleural procedures has led to improvements in the quality of care delivered in this field, it presents challenges in providing this level of care at all times of the day and night.
It is from these difficulties and practical concerns that BTS responded to a call from the pleural community to establish this new Training Standard to detail the capabilities in practice (CiP) for TUS, which will build on the previous curricula and extend the remit to include training for the emergency provision of TUS.
Aim and scope
The aim of this Training Standard is to provide a comprehensive training standard for TUS facilitating timely and improved management of patients with respiratory presentations, particularly (but not exclusively) pleural pathologies.
This Training Standard is predominantly intended for respiratory physicians, respiratory specialty trainees, respiratory (pleural) specialist nurses and physician associates. The Training Standard will also address the provision of acute or emergency pleural ultrasound and will therefore be relevant to providers of acute and out of hours medical care (acute medical and intensive care consultants, advanced nurse practitioners and specialty trainees in general and acute medicine). It is to be emphasised that TUS is to be used in conjunction with clinical information, complementary imaging modalities (plain radiography and CT) and thoracic radiology.
Inclusions
The assessment of normal and abnormal anatomy including normal lung, pleural fluid in infection and malignancy, and pulmonary infection.
The establishment and maintenance of TUS competencies.
Description of a practical and achievable structure for the provision of TUS training across secondary and tertiary healthcare settings.
Exclusions
This is not a training standard for the use of TUS in acute respiratory failure, which is addressed within other specialty curricula. We acknowledge that there will be individuals using point of care TUS in these settings and recognise the mixed and evolving evidence base for this. We suggest that while TUS in skilled hands has a potential role in that setting, it is not considered explicitly within the competency framework of this document.
This is limited to the training of TUS. It does not cover pleural service provision or pleural procedural competency. It does not provide a competence to determine pleural management, but to facilitate this via the provision of bedside TUS.
Methods
The BTS Board of Trustees and the JRCPTB Specialist Advisory Committee (SAC) for respiratory medicine reviewed and approved the proposal for the production of a training standard in TUS. The Chair of the BTS Education and Training Committee was invited to chair the writing group which comprised members of the Respiratory SAC, members of the BTS Pleural Diseases Specialist Advisory Group (BTS Pleural SAG), respiratory physicians with an interest in pleural disease (including pleural leads from specialist centres and from district general hospitals), a pleural nurse specialist, respiratory specialty trainees, and a co-author of the Focused Acute Medicine Ultrasound (FAMUS) curriculum from the Society of Acute Medicine.
The writing group met to discuss and establish the contents of the Training Standard and its format, drawing on preparatory work undertaken by members of the BTS Pleural SAG (Specialist Advisory Group).7
The principles of the document were presented to the open meeting of the BTS Pleural SAG at the BTS Winter Meeting in December 2018 and 2019. Feedback was expressly invited from the BTS Pleural SAG, the British Society of Thoracic Imaging, the Respiratory SAC and other stakeholder groups. The final draft was presented to Respiratory SAC and BTS Board of Trustees for approval in late 2019.
Entrustable professional activity/CiP
Increasingly in postgraduate education, ‘Entrustable Professional Activities (EPAs)’ are being used as an assessment tool to recognise eligibility for independent practice in various procedures or tasks. They are used in a wide variety of training programmes internationally, including pulmonary and critical care in the USA.8 An EPA is a core unit of professional work identified as a task or responsibility to be entrusted to a trainee once sufficient competence has been reached.9 They were conceived and have been used to provide a valid way to assess a variety of skills and to reflect what actually happens in the workplace (ie, trusting a trainee to do something they have shown they can do). They are valuable where a group of learners or trainees need to demonstrate competence in practical procedures in particular. These are often associated with varying complexities of knowledge, skills and attitudes, and ultimately clinical judgement, with ‘competency’ embedded.10 11
An EPA has different levels of supervision that a trainee is required to attain. At each level, trainees need to demonstrate appropriate evidence to allow entrustment decisions to be made and to progress through the levels to get to independent practice. They will become commonplace in the UK and are embedded within the new UK internal medicine curriculum (although termed ‘CiP’) as outcomes demonstrating trainees’ ability to perform the professional activities of a competent physician.12 13 The originally described EPA levels have been adapted by JRCPTB for the ‘CiPs’ in the new Internal Medicine Curriculum into four distinct levels.13 TUS is perfectly suited to having a CiP approach underpinning training and competency confirmation. These levels progress from Level 1, observation only, through to Level 4, independent practice. Of note at Level 3, trainees are entrusted to act with indirect supervision. This stipulates that the trainee is able to provide clinical care without the supervisor present in the room, but the supervisor must be able to attend the bedside to provide direct supervision if required. This would, therefore, not include overnight or out of hours practice directly informing intervention in which a TUS supervisor could not be called to the bedside. Any out of hours scans, therefore, performed by a Level 3 operator would only be undertaken to contribute to logbook for further imaging review.
We have also added a Level 5 (as described in the original EPA literature) to allow for an individual to have clear guidance about how to become a trainer. Table 1 details these level descriptors.
Level descriptors for thoracic ultrasound capability in practice (text in bold represents addendum to JRCPTB GIM CIP descriptors)
A CIP for TUS
A graded approach to confirmation of TUS competency is described with four operator pathways each with clearly embedded CiP descriptors. These Operator pathways are as follows:
Emergency.
Primary.
Advanced.
Expert.
Trainees (or indeed established consultants who require skill development) could progress through CiP levels within particular pathways according to the stage of training and their training requirements. Attainment of levels of entrustability within each pathway would require demonstration of having met the key specific objectives. This bespoke TUS CiP has been designed to meet both the needs of trainees and the clinical demand, and to reflect the reality of where training opportunities exist. Such a framework will have the ability to be transferred between centres within training programmes, and indeed between different training programmes. This will facilitate greater transparency in level of experience acquired by an individual trainee as they move between training posts. The desired level attained would not necessarily be specialty specific but driven by the need of the individual trainee, although different specialty training programmes may choose to recommend certain pathways. Is critical to note that CiP for TUS does not provide pleural procedural capability, nor does it allow practitioners to make management decisions regarding pleural intervention.
This framework will allow trainees in respiratory, acute, emergency and intensive care medicine to attain the skills that will facilitate delivery of safe bedside TUS in a variety of clinical settings.
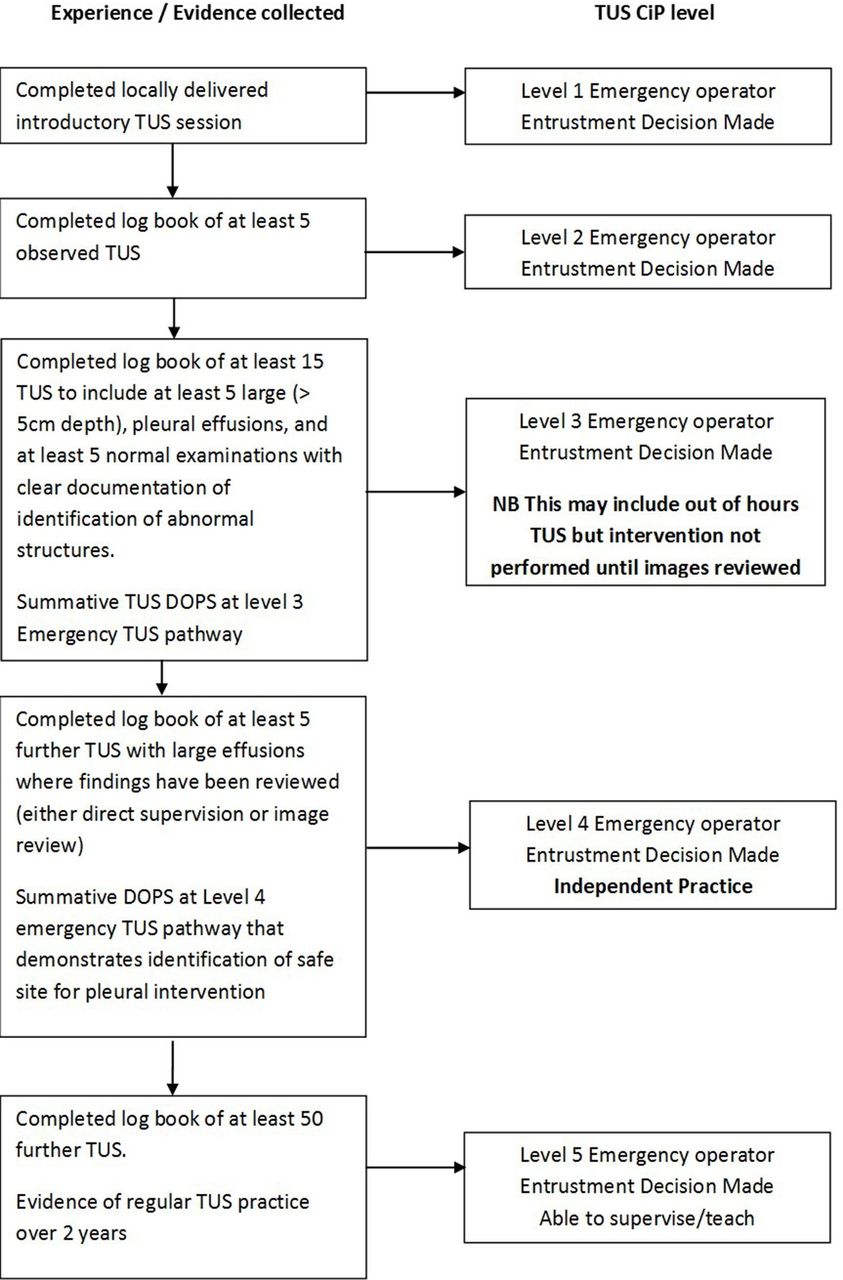
The Emergency Level Operator pathway (figure 1) is recommended as the minimum standard that would be required for anyone who would be undertaking TUS in emergency/overnight practice and would apply to acute/GIM trainees as well as consultants. It could also apply to other out of hours care providers including critical care outreach nurse practitioners.
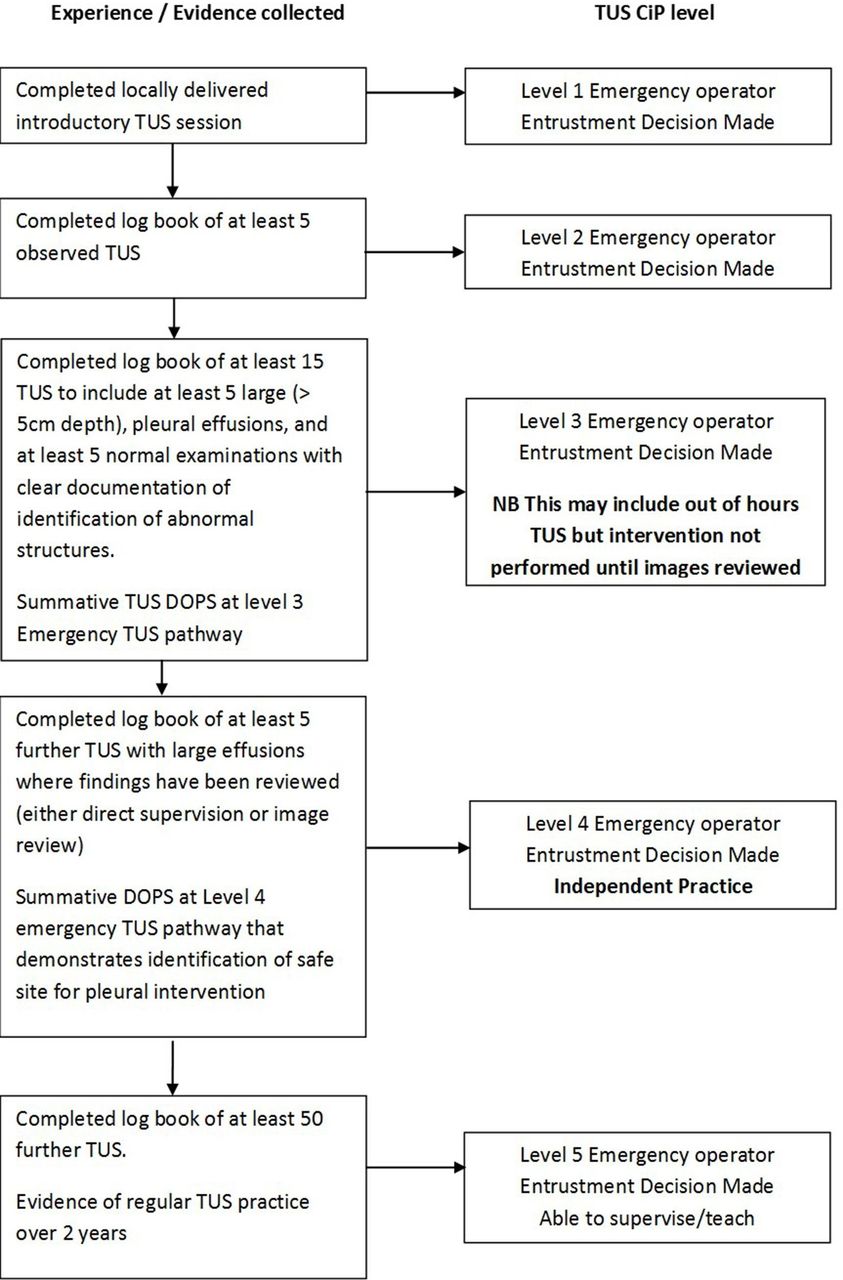
Thoracic ultrasound (TUS) capability in practice (CiP)—Emergency Operator pathway. CiP, capabilities in practice; DOPS, directly observed practical procedure; TUS, thoracic ultrasound.
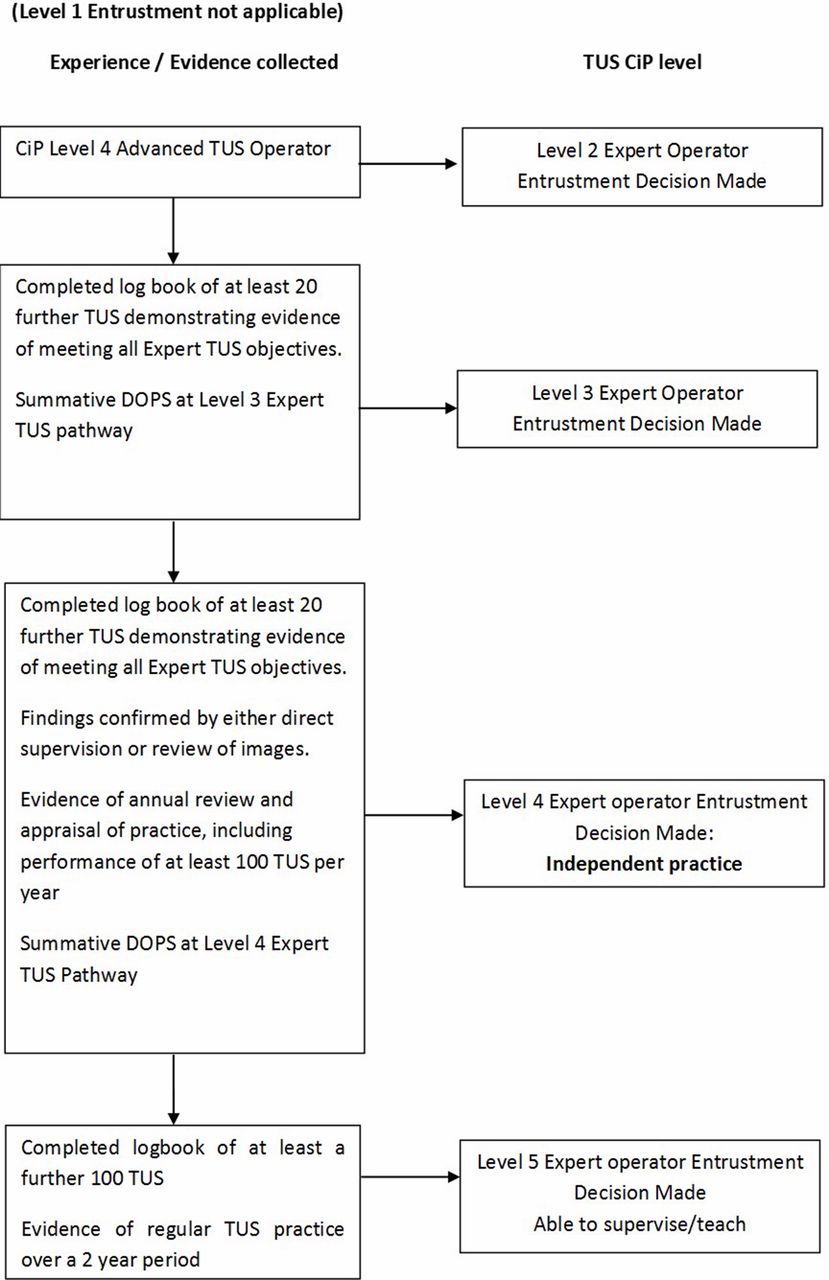
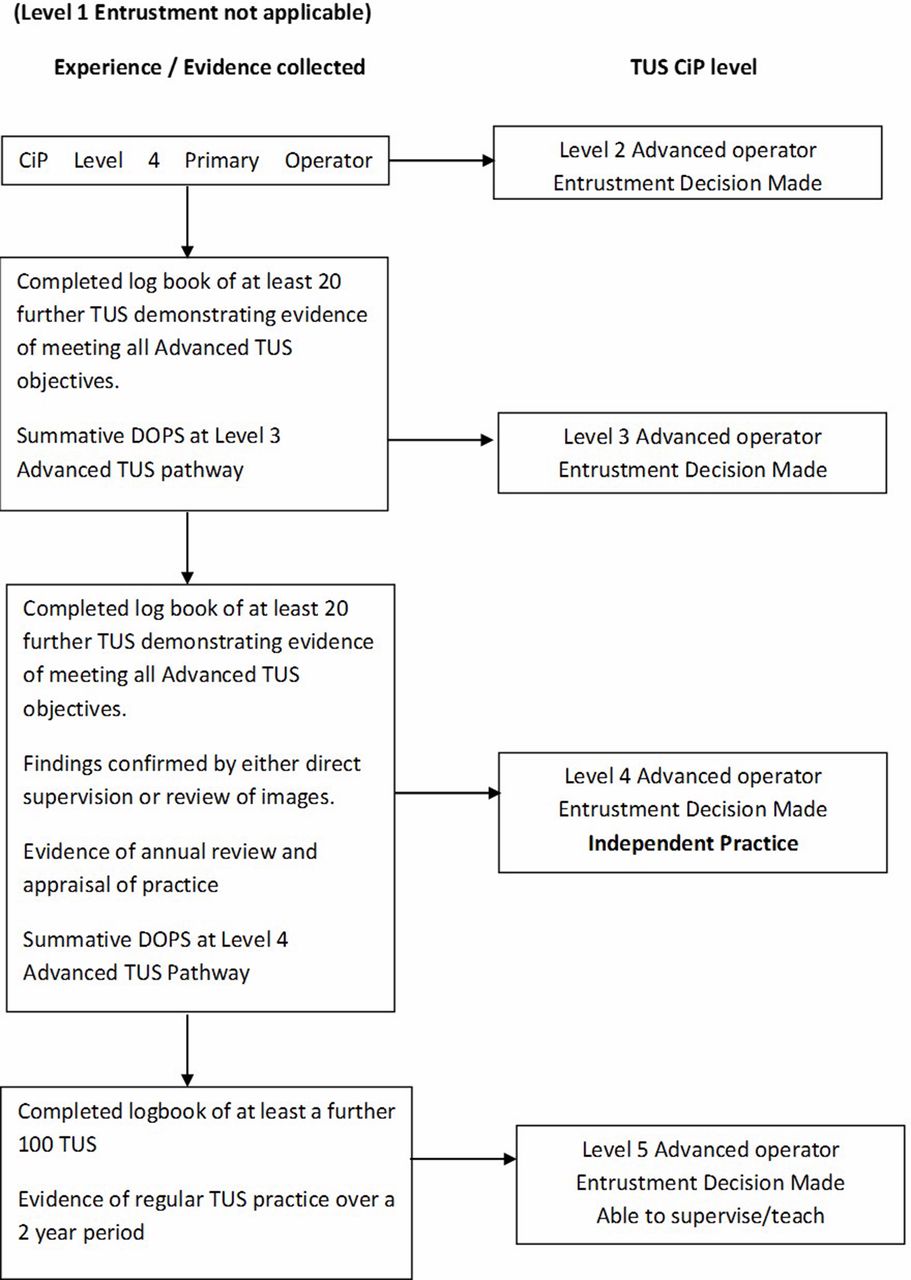
The Primary Operator pathway (figure 2A,B) would be the level that respiratory specialty trainees would be required to attain as part of their specialty curriculum, and that this would be expected at a point in training decided by the Respiratory SAC and JRCPTB. Some respiratory trainees might also wish to progress to Advanced level (figure 3) by the end of training (but this would not be mandatory). The Expert pathway (figure 4) would be reserved for individuals running a specialist pleural service or trainees completing pleural fellowships.

Thoracic ultrasound (TUS) capability in practice (CiP)—Primary Operator pathway. DOPS, directly observed practical procedure.

Thoracic ultrasound (TUS) capability in practice (CiP)—Advanced Operator pathway. DOPS, directly observed practical procedure.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Thoracic ultrasound (TUS) capability in practice (CiP)—Expert Operator pathway. DOPS, directly observed practical procedure.
Practicalities
Trainees must gather evidence as suggested within the relevant TUS level pathway in order to demonstrate competency and therefore allow ‘entrustment’ at the relevant levels within the relevant operator training pathway. To facilitate progression through each pathway, a specific directly observed practical procedure (DOPS) for TUS is required and is provided (online supplementary appendix 1). Opportunities to both observe and perform TUS examinations should be undertaken as and when available, with no specific requirement to attend a specific number of lists or perform a certain number of examinations within a session.
Supplemental material
Ultrasound guidance and ultrasound assistance
There is clear differentiation between ultrasound-assisted and ultrasound-guided procedures. An ultrasound-assisted procedure is defined as ultrasound marking immediately prior to a pleural procedure (a point of care examination performed at the bedside with no delay or patient repositioning between the ultrasound and procedure) and is likely to comprise the majority of pleural procedures. An ultrasound-guided procedure is likely to be reserved for more complex pathologies and should be performed with Advanced and Expert Level practitioners. It involves performing the procedure in real time with the ultrasound probe still on the chest (and typically in a sterile sheath).
Trainers and TUS Mentors
An entrustment decision can only be made at each point of progression by either an operator with CiP Level 5 in the relevant pathway, or by a local ‘TUS Mentor’. This framework is, therefore, a departure from previous guidance requiring RCR Level 1 ‘sign-off’ by an RCR level 2 trainer. Here a primary level operator who has achieved CiP/EPA 5 (figure 2A,B) is able to teach and sign-off primary level trainees. As part of the governance framework around indicating ongoing capability, the creation of the role of TUS Mentor is essential. TUS Mentors will also be required to make annual recommendations regarding ongoing capability towards an individual’s appraisal. Trusts should recognise the demands on time that this will have on individuals taking on the role of TUS Mentor, both in the early phase of adoption of this training standard in agreeing CiP levels for existing practitioners, and thereafter. In addition, it would be anticipated that the TUS Mentor will be responsible for coordinating training, in particular of emergency pathway operators, and so supporting TUS Mentors with appropriate allocation of time within job plans will be essential.
TUS Mentors can be either a consultant radiologist with an interest in thoracic imaging or a respiratory physician who is the local lead for pleural disease and actively delivers a TUS service, with appointment agreed locally. This individual should ideally be competent to the standard defined in the Advanced TUS pathway. It is anticipated that there would be at least one Expert TUS operator available regionally if not locally. CiP level 5 entrustment decisions (ie, the ability to sign off trainees) for all levels of pathways (Emergency to expert) should be made by TUS Mentors only. It is, therefore, envisaged that pleural leads or pleural subspecialists will be TUS Mentors. Local circumstances for pleural services provision may dictate the requirement for more than one TUS Mentor in one Trust as a practical solution (eg, split/multisite trusts). It is appreciated that in smaller hospitals pleural leads might not be Advanced level trained. While this should remain aspirational for all centres in the future, it could be agreed at a local or regional level whether pleural leads with primary level CiP level 5 entrustment are able to impart CiP level 5 sign-off at Emergency level. Regional pleural networks if not already in place should be established to facilitate the progression of capability of primary operators without Advanced or Expert operators in their centres. Importantly, other pleural practitioners who have reached CiP level 5 entrustment at Primary level are still able to provide primary level TUS training.
Trainees aiming to complete Primary TUS pathway can gain and log experience of more complex ultrasound examinations which could, once EPA level 4 in the Emergency TUS pathway is obtained, be used as evidence towards CiP levels within the Primary pathway (figure 2A). It is recognised that there will be trainees on the Primary pathway from the outset and so a specific competence progression is described to meet this need (figure 2B). It would not be appropriate that a trainee could pursue either the Advanced or Expert pathway from the outset, and this framework makes no such provision.
To allow for the varied length of placements within training programmes and for variation between individuals for time taken to achieve varying levels of competence, it is not essential that all entrustment decisions are made by the same trainer. Each trainer must, however, be satisfied that the trainee has provided enough evidence and demonstrated they are meeting the relevant objectives within each pathway, at each entrustment point. Such evidence would be recorded by an individual in their e-Portfolio or a specific ‘pleural passport’. The numbers detailed in the matrix are provided as a minimum and starting point for discussion only—different learners will demonstrate competence with different numbers of procedures. Progression between levels of entrustment is therefore learner—and not time—or numbers driven.
Operator levels: aims and objectives
The aims and objectives for each level of the 4 levels of operator are described below and summarised in table 2a–d. It is again emphasised that TUS is a tool to complement clinical findings and other imaging modalities including plain radiography and CT.
Proposed levels of thoracic ultrasound (TUS) operator and relevant learning objectives
Emergency level TUS operator
Aim
The majority of pleural interventions occur within working hours. Very rarely, there will be a situation where a patient with a life-threatening pleural effusion presents out of hours, when there are no skilled TUS operators available. The rationale for an Emergency level of operator is to address this problem and to give a framework for individual trusts to facilitate the provision of TUS in an emergency where they may not have 24 hours respiratory on call (or weekend respiratory cover) and/or have only distant radiology out of hours service provision.
Training
Training for Emergency level can occur locally. The trainee would be expected to familiarise themselves with local ultrasound machines, under the guidance of a local practitioner with the appropriate skills and experience to undertake this task. This focus is on rapidity of training to promote safety (see competencies in practice section below) and be able to mark a simple large effusion, nominally more than 5 cm in depth. This figure has been chosen to balance ease of identification and safety, and the likelihood for respiratory compromise.
Requirements
The operator should be able to distinguish between vital organs and an effusion. Particular care should be taken to identify acoustic shadows created by ribs, since this can have a similar appearance to an anechoic pleural effusion. Having identified a large effusion, the operator would then be able to recommend a suitable site for safe aspiration or drainage. See table 2A and figure 1).
The Emergency Operator should recognise the limitations and boundaries of their practice such that any findings not typical for a simple large pleural effusion should prompt onward referral to a more experienced practitioner. As part of a personal appraisal, there should be annual review of practice to demonstrate maintenance of competencies (and failure/complication rate).
Practitioners with a completed log book of 50 Emergency level procedures and at least 2 years experience can be signed off by the local TUS Mentor at Emergency CiP level 5 permitting them to supervise and train at eEmergency level.
Service provision issues: emergency level ultrasound operator
The pool of healthcare professionals providing emergency level ultrasound will vary between trusts. The anticipation would be that staff already using USS for other indications (emergency/acute medicine/critical care) may wish to broaden their expertise, especially given it is most likely that these front door areas are where the need for this will be. In addition to providing a training structure for non-respiratory specialists or trainees (eg, in acute, general or emergency medicine), it is also hoped that it will facilitate training in other more permanent practitioner groups (eg, critical care outreach teams) who are also present out of hours within hospitals. The local TUS mentor would agree a pool of emergency TUS operators within their trust. All decisions to intervene should be made by an appropriately capable person in conjunction with local SOP (standard operating procedure) and BTS pleural guidelines.3
Primary TUS operator
Aim
Primary TUS operators require more knowledge in TUS. It is expected that this level of practitioner will form the backbone of TUS services. It is suggested that this level of experience and training should be achieved by ST5 in respiratory training and would be the minimum requirement for CCT (certificate of completion of training) in respiratory medicine. Trainees with a specialist interest may wish to progress to Advanced level prior to CCT in respiratory medicine or within existing consultant posts.
Training
Operators will be expected to have undergone formal training in Primary TUS on a recognised course (course contents are outlined later in this document).
Requirements
The focus of Primary Level training should be on more complex, yet still common pathologies, such as smaller effusions, complex effusions, consolidated lung and pleural thickening. The operator should be able to differentiate between a simple and complex effusion, lung parenchymal consolidation, significant pleural thickening and structures such as the liver and spleen. The Primary Level Operator should be able to identify gross pleural and diaphragmatic nodularity and classify more complex effusions, including identifying features suggestive of an exudate, characterise septations and loculations, and recommend a site for appropriate aspiration or drainage of these. There should be an awareness that TUS can be used to measure diaphragmatic function, both in terms of movement, as well as thickening. See table 2B and figure 2A,B.
Recognition of atypical appearances is important. The Primary practitioner should be aware of his or her own limitations and when to refer on to more experienced practitioners. Since it is expected that this level of training will be for the more regular operator, there should also be a focus on when a procedure is inappropriate based on sonographic findings. There should be demonstration of ongoing practice capabilities as well as audit of outcomes. This would include referral rates to a more experienced practitioner.
This new Training Standard will make the attainment of primary TUS practically much easier for trainees by removing the need to attend regular TUS ‘lists’. It is, however, appreciated that trainees undertaking, but not yet at Level 4 capability in, the primary pathway will have fulfilled the criteria to be signed off at Level 4 Emergency pathway and hence be able to provide emergency out of hours (OOH) TUS for large effusions. TUS primary pathway supervisors or TUS mentors are, therefore, able, with appropriate logbook review and DOPS, to sign off level 4 emergency pathway capability in this situation.
Advanced TUS operator
Aim
Advanced level would be expected in those with regular pleural practice most likely within a dedicated pleural service.
Training
An Advanced level operator should have a minimum of 2 years experience as a Primary level operator, with ongoing practice at this level. It is expected that the local pleural lead would have experience at this level, but it is accepted in smaller trusts that services might not support this, whereby leads would be expected to be Primary level operators with EPA/CiP level 5. EPA/CiP level 5 requires sign off by a regional Advanced level practitioner.
Requirements
Greater focus will be on the detection of more complex sonographic pathology. In addition to greater proficiency in the above competencies, this includes pathologies such as more subtle pleural thickening and its differentiation to fluid via colour Doppler. An Advanced level practitioner will have an understanding of the role of TUS in pneumothorax identification. They will also develop an awareness of how diaphragmatic paralysis may potentially be confirmed via the ‘sniff’ test, but not be specifically required to accurately demonstrate this. The Advanced operator should also be able to identify ‘B’ lines and have an understanding of the potential role of this artefact in pulmonary pathology. See table 2C and figure 3.
The Advanced level practitioner should be able to perform ultrasound guided procedures, such as aspiration and drain insertion. In addition, he or she should be able to scan a patient in the lateral decubitus position in order to guide placement of an indwelling pleural catheter or medical thoracoscopy.
As with previous grades, the Advanced practitioner should be aware of his or her own limitations and refer on to more experienced practitioners when appropriate. There should be demonstration of ongoing practice and capabilities, as well as audit of outcomes. This may include referral rates to a more experienced practitioner.
Expert TUS operator
Aim and training
An Expert level operator should have vast experience in TUS. As such it is reasonable to expect minimum 2 years at advanced level, with over 70 ultrasound procedures per year.
Requirements
The operator should be proficient in using expert modes of ultrasound, for example, M mode and colour Doppler, and maintain practice using more expert techniques. This level of operator is likely to be working as a pleural specialist.
An Expert operator should be able to better estimate diaphragmatic function via assessing movement and change in diaphragmatic thickness during respiration.
In addition to greater proficiency in ultrasound guided procedures, the Expert operator should also be able to perform more complex ultrasound-guided tasks such as pleural and lung biopsy. This would also include pneumothorax induction for medical thoracoscopy under ultrasound real-time guidance. An Expert level operator will maintain an awareness of the benefits of TUS guided biopsy compared with CT-guided biopsy. It is appreciated that Expert operators might also be experienced at USS-guided lymph node biopsies in the cervical and supraclavicular regions, but this is not mandated.
As with previous grades, the Expert practitioner should be aware of his or her own limitations and refer on to other more experienced practitioners when appropriate, although this might not be available locally. There should be demonstration of ongoing practice as well as audit of outcomes. See table 2D and figure 4.
Existing practitioners
Existing practitioners will not be expected to gain formal sign off, but will be able to establish their current level of practice by agreement at local level with the TUS Mentor. It is hoped this will enable current practitioners not previously formally level 2 RCR to be able to obtain CiP level 5 at Primary level TUS and hence officially assess trainees. There will be some individuals practising in dedicated pleural units who would appropriately wish to declare level 4/5 CiP in Advanced/Expert operator pathway but may not have a more experienced TUS operator locally or regionally to provide such entrustment.
They should discuss the scope of their practice with their clinical lead/medical director in relation to the objectives required within the relevant operator pathway to confirm entrustment, and annually thereafter for ongoing capability confirmation. If needed national Expert practitioners could be approached to be involved in any review of practice.
For health professionals at CIP level 4 for Emergency TUS who rotate between trusts it is envisaged that prior to, or at the time of arriving in a new trust an initial meeting with the local TUS mentor will be required. This should take place prior to independent practice to confirm capability and to enable familiarisation with local TUS equipment and SOPs. This would ultimately enable the provision of out of hours emergency TUS across secondary care. It is stressed that CiP level 4 Emergency level does not provide a capability to undertake pleural procedures or intervention, but to facilitate the provision of this.
Maintenance of competency
The aim of this document is not only to provide a structure against which TUS training can be undertaken, but also to emphasise that maintenance of capabilities is essential. Recording and evidencing of ongoing capability for all practitioners should form part of annual appraisal or Annual Review of Competency Progression (ARCP), including peer review of logbook of procedures performed, complications and onward referral. Maintenance of such documentation is responsibility of the practitioner and should be reviewed annually with the TUS mentor. The local TUS mentor should make recommendation regarding ongoing capability to the individual’s appraiser. While a specific number of scans would not be required, a minimum number (either supervised or independent) performed indicating ongoing practice and supporting evidence of maintenance of capability is recommended as follows:
Emergency level operator five scans/year with effusions.
Primary level operator 20 scans/year.
Advanced level operator 30 scans/year.
Expert level operator 70 scans/year.
The numbers above are intended as a guide, with some flexibility around absolute numbers. Where it has not been possible to complete the indicative number of scans, a positive recommendation regarding ongoing capability can still be made through review of previous experience. If there are any concerns relating to capability (eg, long gaps between cases), the local TUS mentor may request additional supporting evidence (eg, DOPS) or additional numbers to confirm capability.
For healthcare professional returning after a period away from practice (eg, maternity leave, prolonged absence or research out of training), it is important practitioners check their level of capability with the local TUS mentor in the trust into which they are returning to work. This will help facilitate a supported return to work if required.
Applicability to other specialties and allied health professions
This document outlines training standards that are designed for clinicians and allied health professionals within respiratory medicine, and those who undertake the care of General Internal Medicine patients with respiratory disease. It is recognised that other training standards exists which cover aspects of TUS (in particular the point of care ultrasound standards FAMUS and CUSIC, which include components of TUS in respiratory failure).14 15 These are complementary to, but separate from, this standard and there will be overlap. Core Ultrasound in Intensive Care (CUSIC) competency requires mentored practice of ‘30 scans with no more than 10 normal scans…. An appropriate range of pathology should be included. Trainees must demonstrate competence in ultrasound guided (direct and indirect) pleural aspiration and drainage’. FAMUS curriculum requires ‘supervision of 10 TUS scans (20 lungs) and 30 mentored scans (60 lungs) and a core pathology achievement which includes the identification of pleural effusion including a site marked for drainage’.14 It is, therefore, accepted that FAMUS and CUSIC accreditation would provide Emergency TUS CiP level 4, but formal agreement of such cross accreditation should be agreed at a local level with the TUS Mentor. FAMUS or CUSIC accredited operators who reach CiP level 5 Emergency level TUS are therefore able to train at this level. This is likely to include current FAMUS and CUSIC mentors (but both groups require local TUS Mentor sign off to achieve level 5 CiP). Maintenance of this CiP level will be reviewed by the local TUS Mentor as part of regular appraisal.
It is acknowledged that the evidence base for TUS is constantly evolving, and as such these training standards will be updated to reflect those changes if and when required.
Further considerations
Image storage
It is noted that demonstration of TUS CiPs will require the ability to store TUS images to facilitate review by trainers and for governance. The authors are aware that this may present technical and financial challenges to trusts. This document, with others, aims to provide a stimulus to gain support of trusts in this important training and governance issue. It is, therefore, expected that all trusts should have systems in place to allow the recording and review of portable TUS images.
Training courses
Many TUS training courses exist across the UK at both national and regional level. It is intended that course contents will reflect the learning aims for the appropriate CiP levels (as outlined above). In addition, the ambition of the group is that the Emergency level CiP will be achievable and allow trusts and deaneries to establish training to facilitate out of hours provision of emergency TUS for the rare occasions this is required.
A ‘Primary’ level TUS course should cover:
Physics and basic principles of sound waves.
Behaviour through different densities.
Characteristics of different frequencies, including probe selection.
Normal artefacts, for example, A-lines and B-lines, mirror imaging.
Doppler effect.
Normal sonographic appearance of thoracic structures, including lung, diaphragm, heart, liver, spleen, kidneys, the pleural line, ribs with acoustic shadow and lung sliding.
The appearance of different densities:
Solid organ.
Fluid.
Aerated lung.
Pathologies, at least in a didactic lecture setting
Simple effusion.
Complex/loculated effusion.
Consolidation.
Pleura nodularity and thickening.
Diaphragmatic paralysis, including ‘sniff test’.
Hands-on, supervised practical experience of varied pleural pathology . In addition:
Demonstration of near gain, far gain and autogain.
Change in depth.
Patient positioning.
Introduction to more complex ultrasound imaging modalities
Probe orientation.
‘B’ mode.
‘M’ mode.
Doppler.
Document review
This document is the first BTS Training Standard document. Given the implications this will have for training and service delivery it will undergo an early review by mid-2021, with anticipation that further reviews will be needed every 3–5 years. This will be overseen by the BTS Education and Training Committee. All stakeholders involved in the creation of this document will be included in this review process. Feedback is also welcomed via email to bts@brit-thoracic.org.uk
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was first published. In figure 2 the word “basic” has been corrected to “primary”.
Contributors JP chaired the working group, and AS and JP as lead authors led the drafting and revision of the document. All authors contributed to drafting the document guideline and undertook revisions of the paper. JP and AS had final responsibility for the document submitted to BMJORR. Dr Anthony Edey represented the British Society of Thoracic Imaging.
Dr Jack Kastelik represented the Respiratory Specialty Advisory Committee.
Dr Nick Smallwood represented the Society for Acute Medicine.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors have completed a declaration of interest form in line with BTS policy and copies are available from BTS head office on request. AE, SH, JK, JL, LL, TN, JP, MR, NS and AS have no funding to declare. ME has declared funding from Astra Zeneca, Pfizer, Abbvie and MSD. IF has declared funding from Boehringer Ingelheim.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.