Article Text

Abstract
Objectives: This study categorised syncopal patients, in a British accident and emergency (A&E) department, into three prognostic groups, using American College of Physicians (ACP) guidelines. The one year mortality of the three groups was studied to see if risk stratification using these guidelines is applicable to these patients and also whether admission improved outcome.
Methods: The records of all syncopal patients presenting to the Leeds General Infirmary A&E department during an eight week period from 2 November 1998 were identified. The cohort was grouped according to ACP guidelines into those who had an absolute indication for admission (group 1), a probable indication for admission (group 2) and no indication for admission (group 3). The actual disposal was recorded and for each patient mortality data were retrieved from general practices or health authorities one year later. The three groups were compared.
Results: Two hundred and ten records (1.7% of all new patients aged 16 years or above) were analysed. Forty per cent of the cohort were not assigned a diagnosis after their assessment in A&E. Forty seven (22%) were placed in ACP group 1, 63 (30%) in ACP group 2 and 100 (48%) in ACP group 3. Thirty six per cent of those in group 1 had died within a year, 14% of those in group 2 and none of those in group 3. In neither group 1 patients (“high risk”) nor group 2 patients (“moderate risk”) did admission to the hospital seem to influence outcome. However, three patients died within a week of their presentation, and two of them had been discharged from A&E.
Conclusion: It is possible to stratify syncopal patients presenting acutely to A&E, according to prognosis, using ACP guidelines. Disposal decisions for these patients should be based on their apparent prognosis (as defined in the ACP guidelines) and not on the diagnosis, which is often difficult to make.
- syncope
- prognosis
- risk stratification
- ACP, American College of Physicians
- CCF, congestive cardiac failure
- VF, ventricular tachycardia
Statistics from Altmetric.com
Syncope may be defined as a sudden loss of consciousness, associated with a decrease in cerebral blood flow, from which the patient makes a full recovery without the need for resuscitation or pharmacological intervention.1 There is no defined time limit for such a recovery to occur, but recovery periods of more than a few minutes may indicate a different disorder (for example, seizures).
Syncope (often described as “collapse query cause” in accident and emergency (A&E) notes) accounts for up to 3% of attendances at emergency departments in the United States, and up to 6% of all hospital admissions.2 A large variety of disease processes can result in the “collapse” of a patient.3 However, many of these patients do not immediately recover and so would not come under the definition of syncope described above.
It is important to note that syncope is a sign and not a disease, and that its occurrence is simply a marker of underlying disease. Such underlying conditions range from the very serious, such as hypertrophic cardiomyopathy or severe aortic stenosis, to the trivial such as a simple faint. Indeed, McClaren et al3 suggested that the heterogeneity of these underlying conditions precludes standardised assessment guidelines for collapsed patients in A&E departments. However, several studies 4–6 have shown that heart disease is prognostically important in patients presenting with syncope. Indeed, syncope itself is not thought to be a risk factor for mortality. Rather it is the underlying heart disease that predicts mortality, and assessment and investigation should be aimed at identifying and treating underlying heart disease.7,8 The American College of Physicians (ACP) recently reviewed the management of patients with syncope.9,10 They included guidelines on which patients should be admitted to hospital and divided patients into groups as follows, depending on the apparent risk of adverse outcome:
Admission indicated
-
history of coronary artery disease, congestive cardiac failure (CCF) or ventricular tachycardia (VT)
-
accompanying symptoms of chest pain,
-
physical signs of CCF, significant valve disease, stroke or focal neurology,
-
ECG findings of ischaemia, arrhythmia (serious bradycardia or tachycardia), long QT interval or bundle branch block.
Admission often indicated
-
sudden loss of consciousness with injury, rapid heart action or exertional syncope,
-
frequent episodes,
-
suspicion of coronary heart disease or arrhythmia,
-
moderate to severe postural hypotension,
-
age over 70 years.
A third group of patients, who do not fall into either of the above groups should be safe to discharge, with or without outpatient follow up.
AIMS
The aims of this study were:
-
To outline the demography of syncopal patients who present to a British A&E department,
-
To categorise these patients using the ACP criteria (as defined),
-
To document the mortality for these three groups after one year.
This study was, therefore, designed to find out if risk stratification (as defined by the ACP) for patients presenting with syncope is applicable to British practice, and also whether admission improved outcome in syncopal patients.
METHODS
The study was carried out in the A&E Department of Leeds General Infirmary, a large urban department that saw 96 202 new patients in 1998. For an eight week period, starting from 2 November 1998, I retrieved the records of patients with a presenting complaint of “collapse”, “collapse query cause”, “faint”, “vasovagal”, “syncope”, “fit”, “seizure” or “fall”. This was done on a weekly basis in the week after their presentation.
Patients were included in the study if they were aged 16 years or above and had a clear history (from the patient or a witness) of temporary loss of consciousness, but recovered spontaneously. Patients were excluded if any of the following applied: focal neurological signs or a GCS <15 when examined by the doctor; a clear seizure in a known epileptic; intoxication with alcohol or other drugs; patient “found on the floor” (that is, without a clear history of temporary loss of consciousness).
The A&E records of patients in the study were checked for details of their previous medical and drug histories. Records of postural blood pressure measurements were noted. Postural hypotension was defined as either a fall in systolic blood pressure of at least 20 mm Hg, a fall in diastolic blood pressure of at least 10 mm Hg or a rise in heart rate of at least 20 bpm within three minutes of standing.11–13 ECGs performed were documented and abnormalities were noted (as defined in the ACP guidelines). The patients were grouped as defined by the ACP, and their diagnoses and disposal after A&E assessment were recorded. This was done one year before data on the outcome (that is, one year mortality) were gathered, so that the ACP group assigned could not be influenced by knowledge of the outcome status of the patient. The general practice or health authority of all patients were contacted one year later to determine whether they were still alive and if deceased their date of death. The registrar of births, deaths and marriages in Leeds was contacted for data as to the cause of death in those who had died.
The study was approved by the local research ethics committee.
RESULTS
During the eight week study period 15 076 new patients, of whom 12 031 were 16 years old or above, attended the A&E department. Two hundred and eight patients satisfied the criteria for inclusion in the study, resulting in an incidence of 1.7% for syncope in patients aged over 15 years. Two patients presented twice during the study period. All 210 records were available for analysis.
There were more women (61%) than men (39%), and a bimodal age distribution with peaks at 25–34 years and 75–84 years (fig 1).

Age distribution of all 210 patients.
Forty seven patients (22%) were placed in group 1, and by ACP guidelines, should have been admitted. Sixty three patients (30%) were placed in group 2 and 100 episodes (98 patients, two of whom presented twice) (48%) were placed in group 3, and thus could have been discharged. However, only 135 patients (64%) had an ECG recorded in the A&E department and 39 (19%) had their postural blood pressures measured. Thus, in some cases, the classification of patients is based on other clinical data available on their record. Details of the three groups are in table 1.
Featurees of the three risk groups
The diagnoses reached after A&E assessment, in each of the three risk groups, are shown in table 2. These diagnoses were those written at the end of the A&E assessment and were not necessarily the final diagnoses. Importantly, half the patients in groups 1 and 2 were not assigned a diagnosis for the cause of syncope, following A&E assessment. The single patient who was diagnosed as suffering from situational syncope was thought to have collapsed secondary to a coughing fit. Among the 11 patients with other diagnoses, neurological conditions made up five (three ?transient ischaemic episode, one ?sub-arachnoid haemorrhage and one ?migraine), endocrine problems four (two hypoglycaemic episodes, one secondary to pre-existing Addison's disease and one secondary to hyponatraemia), one chest infection and one labyrinthitis.
Diagnoses of syncopal patients after A&E assessment
Thirty two patients (68%) in group 1 were admitted to hospital, compared with 34 (54%) in group 2, and 10 (10%) in group 3.
At one year 189 patients of the cohort (90%) could be traced via their general practice or local health authority. Of the 21 untraceable patients 3 (14%) were originally stratified into group 1, 6 (29%) to group 2 and 12 (57%) to group 3. The mortality data are based on the 189 patients traceable at one year.
A total of 24 patients (13%) had died within one year. Sixteen patients (36%) in group 1 (of whom 44 could be traced), and eight patients (14%) in group 2 (of whom 57 could be traced) died within one year. This difference in mortality was statistically significant (χ2=6.82; p=<0.01). No one in group 3 (of whom 88 could be traced) died within one year. Even if all those lost to follow up are assumed to have died, the difference in the proportions of patients who died in group 1 (19 of 47) compared with those in group 2 (14 of 63) and group 3 (12 of 100) remains statistically significant (p=0.039 and p=<0.001 respectively). However, using these data, the difference between groups 2 and 3 is not as marked (p=0.08). Nevertheless, it is highly unlikely that all 12 patients lost to follow up in group 3 died as they were mainly the younger patients without evidence of heart disease. Thus, using one year all cause mortality as the outcome, risk stratification of syncopal patients presenting acutely to A&E is possible using ACP guidelines. Group 1 patients are “high risk”, group 2 patients “moderate risk” and group 3 patients “low risk”, in terms of one year mortality.
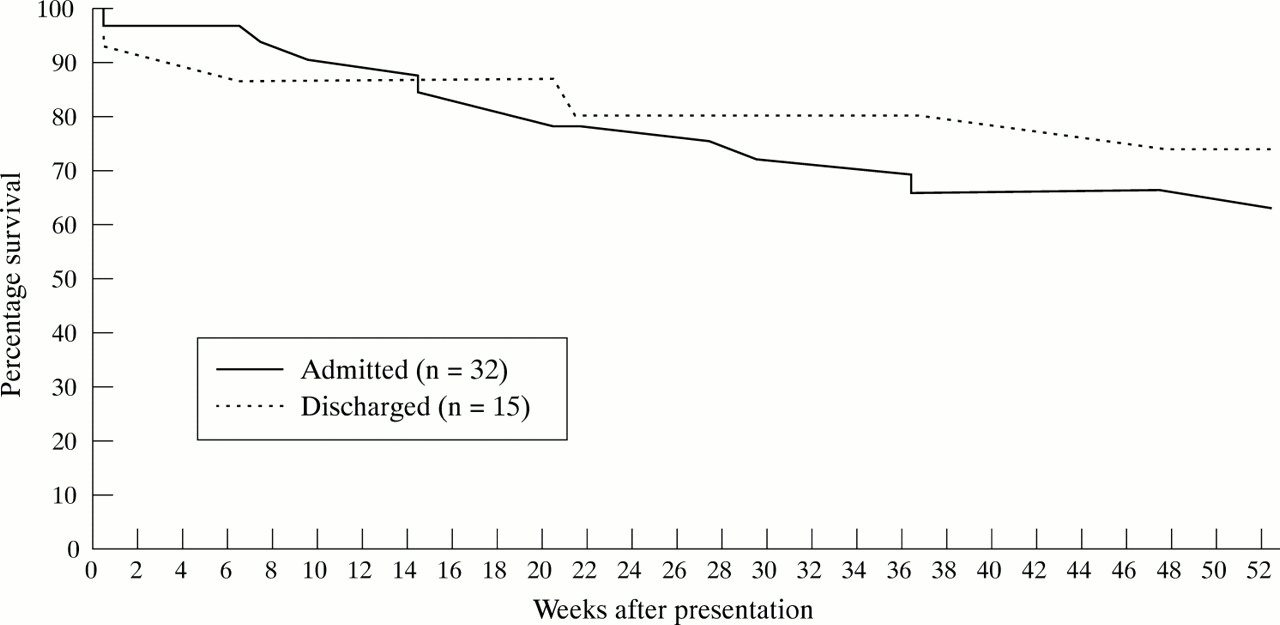
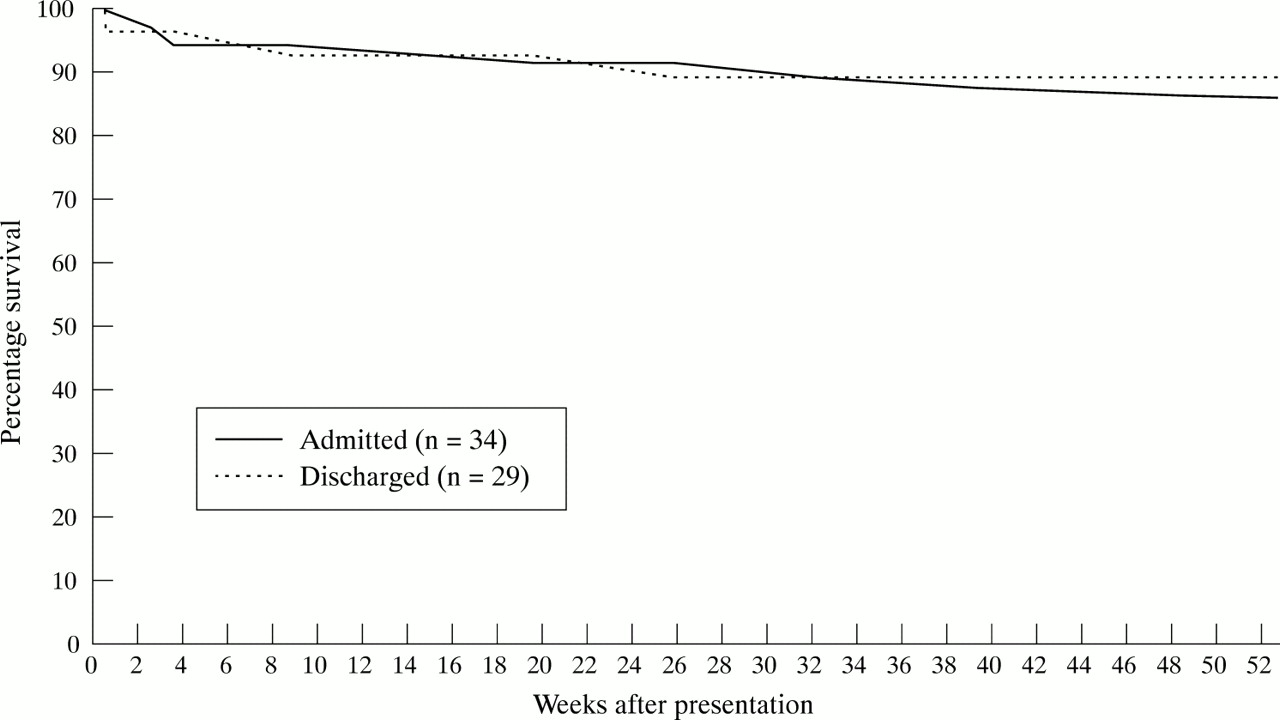
Kaplan-Meier survival curves for patients in the three groups are displayed in figure 2. The data for patients in the “high” and “moderate risk” groups are displayed in terms of disposal in figures 3 and 4 to permit a comparison of those admitted and those discharged to be made. In both the “high risk” (log rank test =0.43, p=0.51) and “moderate risk” (log rank test =0.15, p=0.70) groups, statistical analysis revealed no significant difference in overall survival among those admitted compared with those discharged. This is despite the fact that, in the “high risk” group, those admitted and those discharged were statistically similar in terms of age, proportion over 70 years old, sex, proportion with known organic heart disease and proportion with abnormal ECG. In the “moderate risk” group , however, those admitted were significantly older than those discharged (proportion aged 70 years or over in those admitted was 80%, compared with 54.6% in those discharged).

Survival curves for the three patient groups.

Survival curves for “high risk” group according to disposal.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves for “moderate risk” group according to disposal.
The mean duration of inpatient stay across all specialties was one week (range 1 day to 25 days). Only three patients died during the first week (two of whom had been discharged from A&E) and only five within the first month. Most patients died several months after the index presentation. Sixteen (66%) of the 24 deaths occurred in the Leeds area. Details of the registered cause of death are given in table 3. Interestingly, the two patients who died within the first week after discharge from A&E both had deaths registered as being caused by bronchopneumonia.
Causes of death of the 16 patients who died in Leeds
DISCUSSION
This study has confirmed the results of earlier studies2,3 that show that syncope is a common problem presenting to emergency departments. An incidence of 1.7% is about four syncopal patients every day in a large urban A&E department. This figure is lower than those in the American literature,2 but may indicate that some patients presented primarily with other symptoms (for example, chest pain, palpitations or headache), which this study did not identify. It is essential that all A&E doctors are aware of the factors that put patients at risk of adverse outcome so that proper assessment, investigation and disposition can occur.
This study has shown that 40% of patients presenting acutely with syncope, were not assigned a diagnosis after their assessment in the A&E department. This concurs with other studies1,14–16 that suggest that after clinical history, examination and simple investigations between 37% and 50% of patients who present with syncope cannot be assigned a diagnosis.
This study has shown that many patients attending with syncope did not have an ECG performed or postural blood pressures taken, and it is important to perform these investigations if accurate risk stratification using the ACP guidelines is to be accomplished. Orthostatic vital signs (BP and pulse) should be taken after a period of at least three minutes supine and once again immediately and over a period of three minutes after standing. Positive changes in orthostatic signs include a decrease of 20 mm Hg in systolic blood pressure or 10 mm Hg diastolic blood pressure on standing.12 An increase in heart rate of 20 bpm or more on standing is also an important sign of orthostatic dysfunction and should be included in the definition.11,13 It has been shown that most patients with orthostatic intolerance develop signs and symptoms of this within three minutes of standing hence the need for measurements over this period.17
The results suggest that syncope was the presenting complaint of patients in whom bronchopneumonia was the recorded cause of death. Therefore, it is recommended that patients presenting with syncope have a thorough chest examination as well as chest radiography for those with symptoms and signs of chest disease. Chest radiography would also be part of the evaluation of other underlying diseases, notably congestive cardiac failure and pulmonary embolus.
The 12 lead ECG may only elucidate the cause of syncope in a small proportion of cases (2%–7%),1,16,18 and while postural hypotension may be found in up to a third of the elderly, another, more likely cause of syncope can often be found.17 Therefore, the addition of these simple tests alone would not have vastly improved the diagnosis rate. Nevertheless, they are essential for the accurate risk stratification of patients with syncope.
This study has shown that a large proportion of syncopal patients are elderly and such patients often have complex medical and social problems. There is often more than one possible cause for collapse in these patients and A&E doctors may, therefore, end their assessment without a definite diagnosis. Unfortunately, many studies of syncopal patients have stratified the risk of adverse outcome according to the final diagnosis. Cardiac causes of syncope are known to have a poor prognosis (up to 33% one year mortality), while non-cardiac causes and unknown causes of syncope have a much better prognosis (up to 10% one year mortality).14,19,20 Such risk stratification systems can only be useful if a clear diagnosis is made.
The most important aspect of the A&E assessment of syncopal patients should therefore be to define the apparent prognosis for individual patients and not necessarily the diagnosis. Previous work 4–6,21–24 consistently points to diseases of the heart as being of particular prognostic importance and the focus of any assessment should therefore be to define cardiac disease. The ACP guideline is intended to reflect these risks, and states that for those in group 1, admission is advised for “observation and prevention of the consequences of a more serious subsequent episode or to rule out myocardial infarction”.
This study has shown that patients with risk factors for adverse outcome are those at highest risk of mortality within the year after the episode of syncope. This is reassuring and provides evidence that the ACP Guidelines can be used in British A&E departments. In addition, this study, in common with another from America,25 has shown that 70% of syncopal patients can be stratified into either a “high risk” or “low risk” group, meaning that for the vast majority of patients disposal decisions should not be difficult. Reassuringly, patients at “low risk” (who made up nearly half the cohort) had a 0% one year mortality.
This study has also shown that the occurrence of syncope implies a dismal prognosis for the patient with underlying heart disease, with over a third being dead within a year of the episode. Syncope in these patients is likely to be a symptom of their underlying heart disease and its occurrence should result in thorough evaluation and treatment for any heart disease found. The ACP suggests admission for such an evaluation to take place but it remains unclear whether admission to the hospital does anything to reduce mortality. It is almost certain that, among those at “high risk”, those admitted had a greater severity of underlying heart disease or had greater comorbidity than their discharged counterparts, and it is therefore impossible to draw any firm conclusions about the most appropriate disposal for these patients. Nevertheless, given the fact that two of the three early deaths occurred in those discharged from A&E, it would seem reasonable (as suggested by the ACP) to admit all “high risk” syncopal patients and strongly consider admission for those at “moderate risk”. Early access to outpatient syncope assessment clinics (which have previously been shown to have a high diagnostic yield 26) may allow patients at “moderate risk” to be discharged safely from A&E in the future.
Mention should be made of the limitations to this study. Firstly, the quality of data obtained in a retrospective study is only as accurate as that which is recorded and stored. For example, it is possible that some patients had an ECG recorded and it was lost, or that some had a diagnosis made but that this was not recorded in the notes. Secondly, knowledge of mortality data in the 21 patients in which this could not be obtained may also have altered the results.
CONCLUSION
Some 1.7% of all new adult attendances at a British A&E department present with syncope. Patients at highest risk of adverse outcome are those with underlying heart disease and can easily be defined with reference to ACP guidelines. “High risk” patients (as defined in ACP guidelines) have a one year mortality rate of 36% after an episode of syncope. In A&E practice, management decisions are more important than diagnoses. A&E doctors should, therefore, assign a prognosis, rather than a diagnosis, to syncopal patients in order to make decisions about proper disposition and follow up. This decision making process should be aided by a detailed history, examination (including measurement of postural blood pressure) and an ECG in all such patients, with chest radiography in those with symptoms and signs of chest disease.
Acknowledgments
I would like to acknowledge the help of Wendy Parsons (medical statistician at the Leeds Teaching Hospitals NHS Trust), Mr David Simpson (Chief Superintendent Registrar for Leeds) and Maureen Braithwaite and the reception staff at the Accident and Emergency Department of Leeds General Infirmary.
CONTRIBUTORS
Steven Crane developed the study protocol, collected all the data, and wrote the paper. He is the guarantor of the paper.
REFERENCES
Footnotes
-
Funding: none.
-
Conflicts of interest: none.