Article Text

Abstract
Introduction: Emergency department (ED) physicians face frequent decisions on whether to admit patients with congestive heart failure (CHF) or acute exacerbation of chronic obstructive pulmonary disease (COPD). This feasibility study evaluated the potential of a structured 3-minute walk test as a clinical decision tool for admission and correlated its performance with poor clinical outcomes. It also aimed to gather evidence and directions for the design of a multicentre study to derive clinical guidelines.
Methods: In this prospective cohort study, a convenience sample was enrolled of 40 adult patients who presented to a tertiary care ED with CHF, COPD, or stable chest pain and were being considered for discharge. Patients walked at their own pace and their dyspnoea, respiratory rate, heart rate and oxygen saturation were recorded each minute for 4 minutes. The primary outcome was “poor clinical outcome” defined as admission to hospital, the need for biphasic positive airway pressure, the need for intubation, relapse, or death.
Results: 85.0% successfully completed the test and 30.0% had poor clinical outcomes. Of those with poor clinical outcomes, 41.7% were unable to complete the test compared with only 3.6% of those with good clinical outcomes (p<0.01). Significant differences were noted in the dyspnoea (p = 0.04) and respiratory rate (p = 0.03) as well as oxygen saturation measurements at 3 minutes.
Conclusions: The 3-minute walk test is a non-resource intensive, simple procedure with applicability in most ED for discharge decisions in patients with cardiopulmonary conditions. Multicentre studies are being planned to validate these findings and establish guidelines for admission and discharge of patients with CHF or acute exacerbation of COPD.
Statistics from Altmetric.com
Dyspnoea caused by congestive heart failure (CHF) or acute exacerbation of chronic obstructive pulmonary disease (COPD) has been estimated to account for 12.6% of adult emergency department (ED) visits in the USA.1 There are currently no clear guidelines to help the emergency physician decide which of these patients requires hospital admission. The ability to identify patients safe for discharge accurately and quickly would be extremely helpful, from both a patient care perspective and an administrative point of view. Walk tests have informally been used in the ED to determine whether patients with various respiratory and cardiac conditions are ready for discharge. To our knowledge, no studies have evaluated the performance of a structured walk test as a predictor of outcome in the emergency setting.
The goals of this study were to determine the feasibility of a structured 3-minute walk test in the ED from a resource and patient care perspective and to determine its preliminary usefulness as a predictor of clinical outcomes for patients with CHF or COPD exacerbation.
METHODS
Study design, study setting, and population
This prospective cohort study was conducted in the ED of The Ottawa Hospital, Civic Campus, a teaching tertiary care centre with an annual census of approximately 55 000 visits. The Research Ethics Board of our institution approved the study and all patients provided written, informed consent. We planned to enroll a convenience sample of patients more than 50 years of age presenting with either CHF or acute exacerbation of COPD over a 3-month period. A sample of stable chest pain patients was added half way through the study to allow for an adequate sample size to provide a meaningful evaluation. Patients were excluded if they were: (1) deemed too ill (ie, resting oxygen saturation <90% on room air or baseline oxygen, heart rate ⩾120 beats per minute for more than 1 minute, or systolic blood pressure <90 mm Hg); (2) definitely being admitted to hospital; (3) unable to ambulate; or (4) experiencing ongoing chest pain or acute ECG changes. No subsequent follow-up was conducted on these excluded patients.
Study protocol
Consenting patients meeting the inclusion criteria were interviewed by a trained research assistant at their bedside in the ED before conducting the test. The characteristics of the patients, including demographics, past medical history and home support, were collected. The 3-minute walk test protocol was as follows: after a brief explanation of the protocol, including how to rate dyspnoea on the modified Borg scale, patients were asked to ambulate within the ED for 3 minutes at their own pace on level ground either on room air or on their baseline home oxygen rate and with any walking aid they would normally use. Patients were accompanied by a respiratory therapist and a trained research assistant, who was responsible for recording the measures of dyspnoea, oxygen saturation, heart rate and respiratory rate on a standard case record form at baseline, and at 1, 2 and 3 minutes during the walk, and at 1 minute post-walk. The respiratory therapist carried all necessary equipment, including pulse oximeter (model NPB-40; Nellcor Puritan Bennett, Boulder, Colorado, USA) and portable oxygen tank if needed, leaving the patients relatively free to ambulate at their own pace. The walk test was discontinued if at any time the patient experienced severe shortness of breath (modified Borg scale rating ⩾7),2 anterior chest pain, or a decrease in oxygen saturation to less than 86% for 30 s, heart rate 120 beats per minute or greater for 60 s, or if the patient felt that he or she was unable to continue walking. For these patients, the missing data were not inputted for analysis. Data analysis was performed only on values recorded.
Measures
The primary outcome measure was “poor clinical outcome” defined as any of the following within 14 days of the ED visit: (1) admission to hospital; (2) biphasic positive airway pressure; (3) endotracheal intubation; (4) relapse; or (5) death. Relapse was defined as return to hospital because of worsening respiratory or cardiac symptoms. These outcomes were determined by a review of the patients’ health records and by a follow-up telephone interview.
Data analysis
Univariate analyses were performed to determine the association between characteristics of patients and poor clinical outcomes. Fisher’s exact test, Student’s t test, or the χ2 test were used as appropriate. A repeated measures mixed general linear model was used to determine the association between the 3-minute walk test component measurements and poor clinical outcomes.
RESULTS
Between June and August 2005, 40 patients were enrolled into the study. The characteristics of the study population, the walk test results and the frequency of poor clinical outcomes are shown in table 1. The total duration of the procedure, from giving the patients instructions on how to rate their dyspnoea to the conclusion of the walk, was a mean of 8 minutes. Resources required for the completion of the walk test include a respiratory therapist, portable pulse oximeter and stopwatch.
Overall, 34 of 40 subjects (85%) completed the walk test and 12 (30%) were deemed to have a poor clinical outcome, mostly same-visit admission or relapse. The association between patient characteristics, including walk test results, and clinical outcome is shown in table 2. Inability to complete the 3-minute walk test was a strong predictor of poor clinical outcome; 96.4% of those with good clinical outcomes completed the walk test compared with only 58.3% of those with poor clinical outcomes (p<0.01). Furthermore, in analysing the results, we found that no patients in the good outcome group had an oxygen saturation of less than 90% at completion of the walk test (p<0.01).
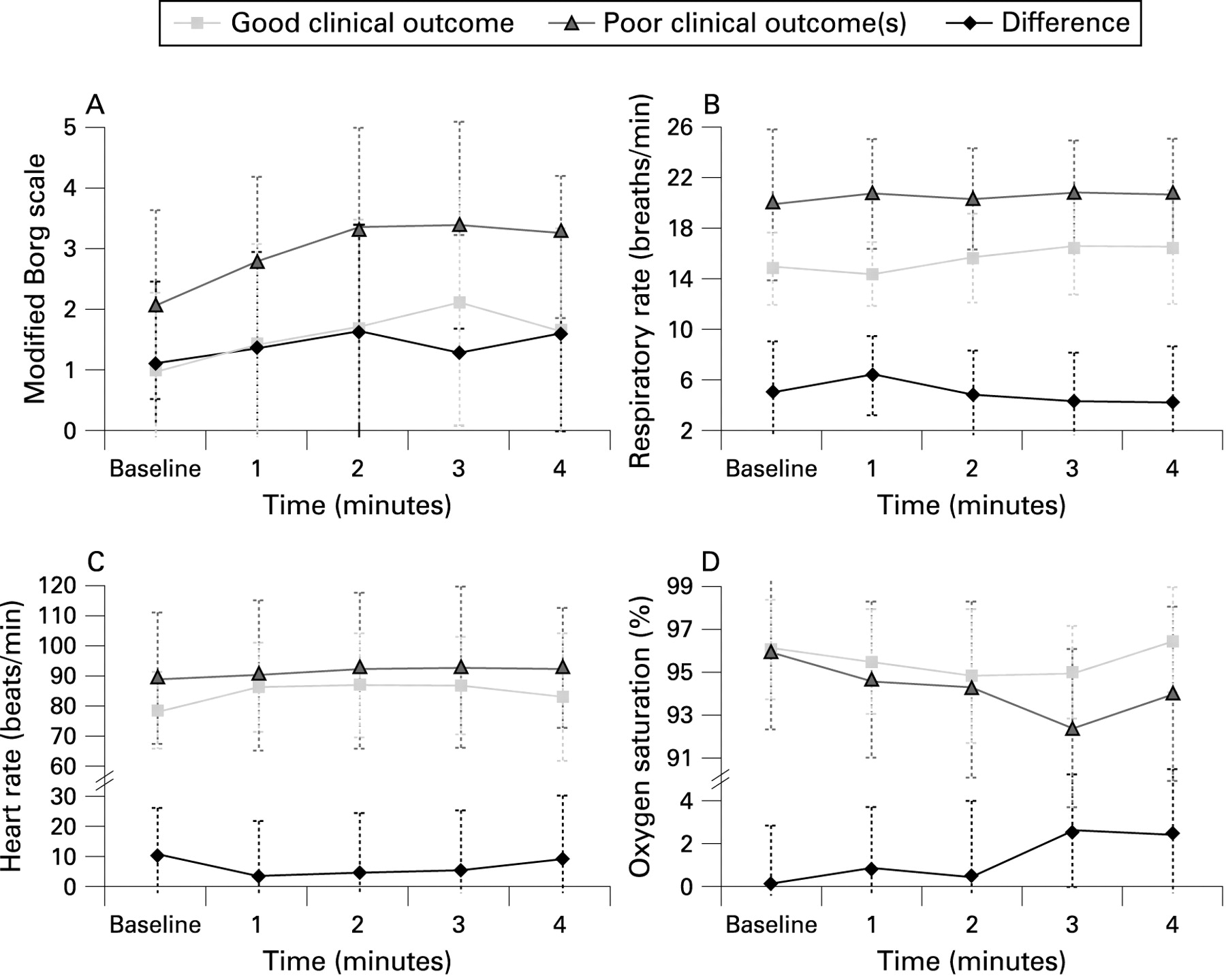
The data for the measurements taken during the 3-minute walk test are summarised in fig 1. A repeated measures mixed general linear model was used to determine statistical differences of those with good clinical outcomes versus those with poor clinical outcomes, which yielded p values of 0.04, 0.03, 0.08 and 0.09 for dyspnoea, respiratory rate, heart rate and oxygen saturation measurements, respectively. Patients who had poor clinical outcomes rated their dyspnoea worse, had higher respiratory rates and heart rates both at baseline and during the walk test, and developed lower oxygen saturations during the walk test.
{kind=link}
Serial dyspnoea scores and vital signs during the 3-minute walk test (mean, SD). (A) Dyspnoea (p = 0.04); (B) Respiratory rate (p = 0.03); (C) Heart rate (p = 0.08); (D) Oxygen saturation (p = 0.09).
None of the chest pain patients experienced a poor clinical outcome and all completed the walk test. The performance of the walk test among the a priori study population of CHF or COPD is shown in table 3. The unadjusted odds ratio for association between completing the walk test and experiencing a good clinical outcome in this subgroup of patients was 8.6 and that of oxygen saturation of 90% or greater at 3 minutes and good clinical outcome was 9.7.
DISCUSSION
This study serves as an initial step in the analysis of the utility of the 3-minute walk test as a predictor of outcome for patients with CHF or COPD exacerbation. Individuals with severe exacerbations of these conditions decompensate when their cardiopulmonary system is stressed. A standardised walk test provides the opportunity to test the patient’s performance in a safe environment. From a resource and equipment perspective, the 3-minute walk test is an extremely portable test. Heart rate and oxygen saturation were easily measured using the pulse oximeter. However, respiratory rate measurements proved challenging and difficult to measure reliably. This variability might be improved by using a respiratory rate monitor. For dyspnoea, the use of the modified Borg scale has been well established as a reproducible and accurate measure of dyspnoea in the exercise setting.3 4 However, some patients had difficulty coming to a decisive conclusion as to their level of dyspnoea, whereas a few initially reversed the scale when evaluating their shortness of breath, but were able to rate their dyspnoea correctly once the modified Borg scale was re-explained.
Given the wide range of levels of normal exercise tolerance for individuals with varying disease severity, we attempted to compensate for this by measuring how well patients tolerated the 3-minute walk test from their baseline level of functioning. If the patients required regular supplemental oxygen at home, then this oxygen rate was provided to them during the walk test. Furthermore, patients were allowed to walk at their own pace and use any supplemental walking aids, such as a cane or walker, during the walk test protocol. The premise for this is to allow for meaningful assessment of the patients’ ability to compensate for a cardiopulmonary stress applied to their normal level of functioning.
This study showed that those in the poor clinical outcome group had higher dyspnoea scores, respiratory rates, heart rates and lower oxygen saturation levels. The ability of patients to complete the walk test and their oxygen saturation levels at 3 minutes were predictors of clinical outcomes. These trends are strongly encouraging for further study of the 3-minute walk test. Of the poor clinical outcome measures, the decision to admit was decided by the attending ED physician. Although this individual was not blinded to the results of the test, leading to potential bias, we feel that the effect is minimal as ambulatory oximetry tests are frequently and informally used in the study setting and that in most cases the patient’s disposition had generally been decided upon before the start of the test. Furthermore, because of the prevalence of informal walk tests being used at the study centre, physicians were less likely to alter their discharge decision and clinical thresholds for discharge as a result of awareness of the study in the absence of clear guidelines.
Current risk stratification algorithms for dyspnoeic patients deal primarily with hospitalised patients or the chronic setting.5–7 Moreover, tests of exercise capacity such as the 6-minute walk test may be unrealistic for the ED setting as the main measure is distance and the test calls for a straight unobstructed hallway 100 feet long.7 The use of a respiratory therapist in the study protocol was to ensure patient safety during this novel study; however, from a practical perspective, no extra resources or specialised training is needed for the measurements as dyspnoea symptoms were self-reported by the patient and the other measurements can easily be obtained from an automated portable monitor. Furthermore, the test would be conducted within the confines of the ED, so risk associated with the test from a patient safety perspective would be minimal.
In this study, we added stable chest pain patients to the study population to allow us to evaluate the feasibility of performing the test in the ED environment as a result of the limited enrollment of patients during the study period. Although these patients were instrumental in the evaluation of the feasibility aspect of the 3-minute walk test, they contributed little information to the predictive value of the walk test. The stable chest pain patients did not experience any adverse outcomes during the protocol, and as such can contribute to bias in the interpretation of the walk test results. Furthermore, no concrete reason was identified to explain the limited enrollment during the study period; some possible reasons are as follows. A convenience sample of patients was enrolled and those who undertook the walk test had to meet specific inclusion criteria and fail to meet the exclusion criteria. Approximately three-quarters of the patients who presented to the ED with acute dyspnoea during the study period were interviewed but did not undertake the walk test because they either declined to participate, were incapable of consenting, failed to meet the inclusion criteria, or met one of the exclusion criteria.
The results from this study support continued study of the 3-minute walk test, including other conditions beyond CHF and COPD exacerbations. Our research group is currently planning a multicentre national study to evaluate further the 3-minute walk test for CHF, acute exacerbation of COPD, pneumonia and asthma, as well as to formulate clinical decision guidelines for the admission or discharge of patients with these conditions.
CONCLUSIONS
The study showed that the 3-minute walk test is a simple and fast test. Its portability supports further study for incorporation into discharge decisions for patients with CHF or COPD exacerbation. The study sample did not provide sufficient power to draw definite conclusions for clinical practice, and further multicentre studies are being planned to study the role of the walk test to provide risk stratification guidelines for dyspnoeic patients.
Footnotes
Presented at the 2006 Society of Academic Emergency Medicine Annual Meeting in San Francisco, CA (18–21 May 2006) and at the 2006 International Conference on Emergency Medicine in Halifax, NS (3–7 June 2006).
Competing interests: None.
Ethics approval: The Research Ethics Board of the Ottawa Health Research Institute approved the study.
Patient consent: Obtained.
Linked Articles
- Primary survey