Article Text

Abstract
Introduction The National Early Warning Score (NEWS) aids the early recognition of those at risk of becoming critically ill. NEWS has been recommended for use by ambulance services, but very little work has been undertaken to date to determine its suitability. This paper examines whether a prehospital NEWS derived from ambulance service clinical observations is associated with the hospital ED disposition.
Methods Prehospital NEWS was retrospectively calculated from the ambulance service clinical records of 287 patients who were treated by the ambulance service and transported to hospital. In this cohort study, derived NEWS scores were compared with ED disposition data and patients were categorised into the following groups depending on their outcome: discharged from ED, admitted to a ward, admitted to intensive therapy unit (ITU) or died.
Results Prehospital NEWS-based ambulance service clinical observations were significantly associated with discharge disposition groups (p<0.001), with scores escalating in line with increasing severity of outcome. Patients who died or were admitted to ITU had higher scores than those admitted to a ward or discharged from ED (mean NEWS 7.2 and 7.5 vs 2.6 and 1.7, respectively), and in turn those who were admitted to a ward had higher pre-hospital NEWS than those who were discharged (2.6 vs 1.7).
Conclusion Our findings suggest that the NEWS could successfully be used by ambulance services to identify patients most at risk from subsequent deterioration. The implementation of this early warning system has the potential to support ambulance clinician decision making, providing an additional tool to identify and appropriately escalate care for acutely unwell patients.
- emergency medical services
- ambulances
- early warning score
- national early warning score
Statistics from Altmetric.com
Key messages
What is already known on this subject?
There is little published evidence regarding the use of early warning scores by ambulance services and no recommendations regarding the urgency and scale of the clinical response that should be aligned to each risk category.
In 2012, the National Early Warning Score (NEWS) was introduced with the aim of standardising the recognition and response to the early signs of critical illness across the NHS.
There is a need to further explore whether prehospital NEWS could indicate hospital discharge disposition and thus assist paramedic decision making.
What this study adds?
There are strong associations between NEWS calculated from ambulance service clinical records and the patient’s disposition as reported by the ED.
Statistically, the time of NEWS calculation does not appear to influence the score; however, clinically, the timing of the calculation is likely to be important.
Before implementation, guidance for ambulance services is needed linking NEWS risk levels to the urgency and scale of the clinical response required.
Introduction
Early warning scores (EWSs) are simple scoring systems based on physiological measures designed to facilitate rapid recognition of the early signs of critical illness or deterioration and to inform the most appropriate clinical response.1 In 2012, the UK’s Royal College of Physicians (RCP) launched the National Early Warning Score (NEWS) with the aim of replacing the various early warning scoring systems used locally within hospitals and standardising the identification of those at risk of deterioration.2 Much support has been generated for the NEWS since its introduction, with positive results reported in several high-profile journals.3–11
The RCP strongly recommends the prehospital use of NEWS to facilitate communication of a patient’s clinical condition to the receiving ED.2 However a recent review12 showed there is little published evidence regarding either the use or effectiveness of EWS by ambulance services. Furthermore, guidance is unclear at what point in the patient’s prehospital care episode a NEWS should be calculated. To give an indication of the best time to calculate prehospital NEWS, we explored whether there were any differences in scores derived from the initial set of ambulance clinician observations compared with those taken prior to handing the care of the patient over to hospital.
Of the few studies that have examined the use of EWS by ambulance services,13–16 only one has specifically looked at NEWS. This study, conducted in Scotland, reported an association between elevated NEWS and a higher incidence of adverse outcomes, demonstrating its ability to identify high-risk patients at an early stage.17 Our study, the first to be conducted in an English ambulance service, aims to contribute to the limited body of evidence by examining whether prehospital NEWS can indicate subsequent hospital discharge disposition. We also examine whether the timing of the NEWS calculation in the prehospital phase is important.
Method
Study design
This retrospective cohort study examined associations between prehospital NEWS and hospital discharge disposition using observational clinical data collected from London Ambulance Service NHS Trust (LAS) records between April 2012 and January 2013 and a matched ED dataset from three EDs in West London. Data were opportunistically available as a result of a larger project specifically looking at the feasibility of linking ambulance service and ED clinical datasets.
Setting and population
The LAS operates across the UK’s capital city, London, covering a geographical area of 1580 km2 (610 m2) with a population of 8.6 million people. The LAS responds to ≈1.9 million calls annually and attends to 1.2 million incidents.18 There are 35 EDs in the London area to which LAS clinicians can convey patients.
Participants
Participants consisted of patients who, during the 12-month observation period, were treated by ambulance clinicians, conveyed to a hospital and for whom ED data were available. Records were excluded for patients aged under 16 years of age or pregnant (as per NEWS recommendations), or if they contained insufficient information to enable a NEWS calculation.
Sources of data
Routine ambulance clinical records were used to retrospectively calculate NEWS based on both the initial prehospital observations taken on arrival of the first ambulance clinician and the final prehospital observations taken prior to arriving at the ED. Using hospital discharge disposition data collected from the ED, we created four outcome categories: discharged, admitted to a ward, admitted to the intensive therapy unit (ITU) or died. NEWS scores were aggregated and categorised into clinical risk levels (low, medium and high) as described in the RCP Working Party Report.2
Data were collated and stored following Good Clinical Practice Guidelines and the relevant legislation governing the use of patient data. The NHS’s Health Research Authority Ethical Committee was satisfied that ethical approval was not required for this observational study using anonymised data. Potential sources of bias were minimised as NEWS was retrospectively calculated independently from the ambulance clinicians and hospital staff making clinical decisions.
The sample
During the study period, ambulance and ED records were electronically linked for a total of 47 964 patients: 28 757 (60%) were discharged, 18 957 (39.5%) admitted to a ward, 164 (0.3%) admitted to the ITU and 86 (0.2%) died. Due to the need for manual data entry of all clinical ambulance data necessary to calculate NEWS, it was not possible to include all cases. Using systematic sampling, we aimed to include 100 patients in each disposition category. Where fewer than 100 patient records existed, all cases were included. The records for 56 of the 86 patients who died did not contain sufficient information to allow prehospital NEWS calculations and as such this cohort consisted of 30 patients. For those admitted to the ITU, 107 patient records were not sufficiently completed leaving 57 patients in this group. In total, 287 patients were included in our study: discharged: n=100 (35%), admitted to a ward: n=100 (35%), admitted to the ITU: n=57 (20%) and died: n=30 (10%).
Statistical analysis
Data were analysed using IBM SPSS for Windows V.19. Using a paired t-test, we compared the initial and final NEWS to examine whether the timing of the calculation was important. Repeated measures analysis of variance (ANOVA) was used to test for interaction effects between initial and final NEWS scores and disposition (discharged, admitted to a ward, ITU or died). ANOVA was also used to examine the relationship between the retrospectively calculated NEWS and outcome. χ2 and logistic regression analyses were used to determine whether risk categories indicated outcomes.
Results
Comparison of initial and final NEWS
Initial prehospital NEWS for all study patients ranged from 0 to 17, with a median score of 3. There was a similar dispersion for the final prehospital NEWS ranging from 0 to 16 with a median score of 3. There were no significant differences between initial and final NEWS values (mean=3.92 vs 3.87; 95% CIs 3.49 to 4.35 and 3.40 to 4.33; p=0.68) indicating that overall the patient condition did not significantly improve or deteriorate during the prehospital phase.
There was a significant interaction effect p<0.05 (figure 1). Patients who were ‘admitted to the ITU’ and ‘died in ED’ had much higher initial and final NEWS with the biggest difference between the two scores being within the group who died.
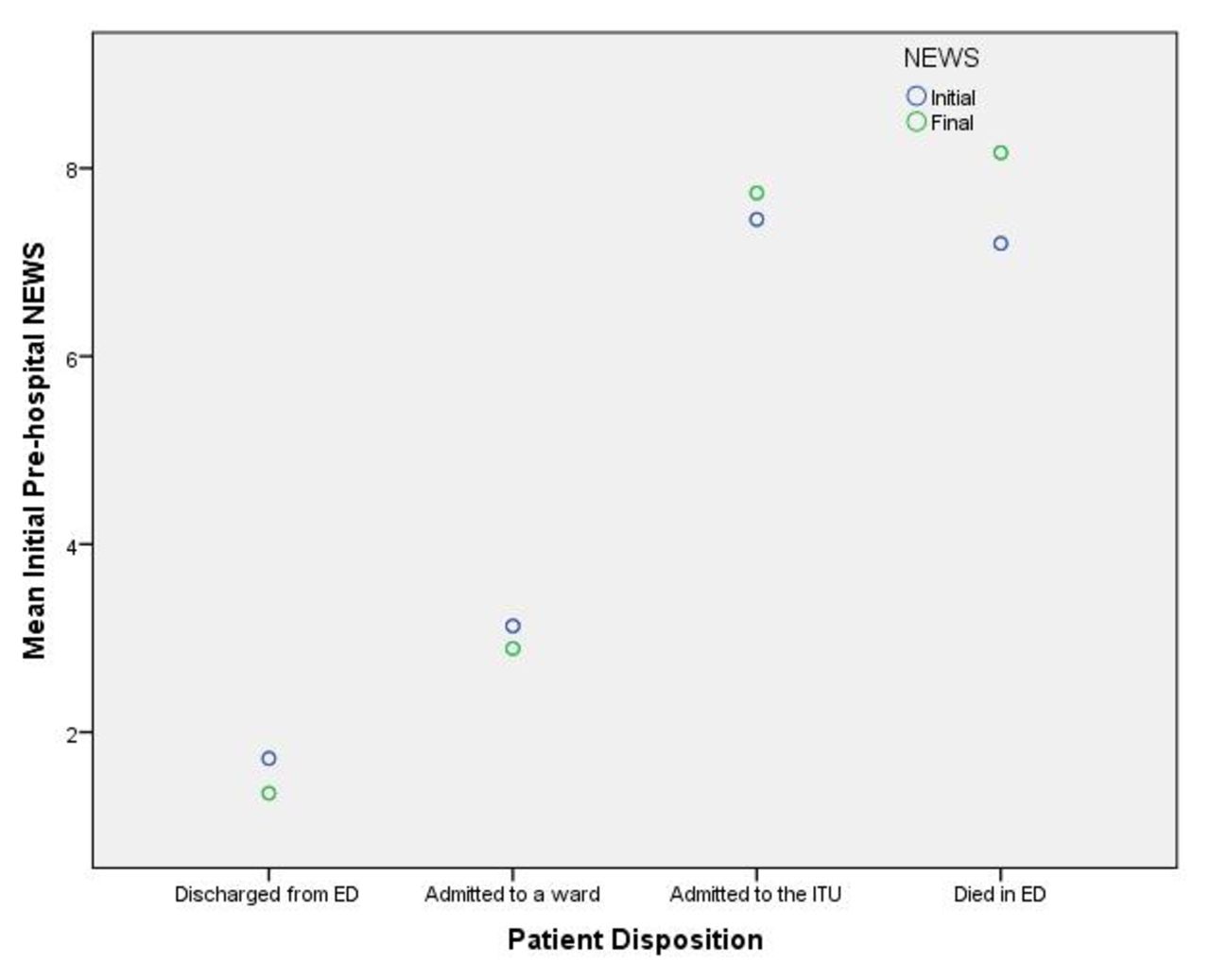
Mean initial and final prehospital NEWS by patient disposition group. ITU, intensive therapy unit; NEWS, National Early Warning Score.
As there were no differences between NEWS calculated using the initial set of observations and those taken later in the prehospital episode, the remainder of this paper focuses on initial NEWS calculations only as it is the initial score that ambulance clinicians are most likely to use to inform clinical and transportation decisions.
Demographics for each patient disposition group
The mean age of the sample was 63 years (ranging from 16 to 97 years). Overall, the proportion of males was slightly higher than females (52% vs 48%) reflected in each disposition groups with the exception of those who died in the ED. The chief complaint given at the time of the 999 call and the presenting illness of the patient on arrival of the ambulance clinicians were varied with ‘Breathing problems’ (13.2%) being the most frequently documented chief complaint among the whole sample and ‘Abdominal pain’ being the most commonly recorded presenting illness (9.1%). The most frequently reported chief complaint and presenting illness for each disposition group are presented in table 1.
Demographics presented by patient disposition
NEWS for each patient disposition group
NEWS calculations significantly differed between patient disposition groups p<0.001 (table 2). Post hoc tests (Tamhane’s T2) confirmed that patients who were discharged had significantly lower NEWS than those who were admitted to a ward, admitted to ITU or died. Patients admitted to a ward had lower NEWS than those admitted to ITU or died. There were no significant differences between the scores for patients who were admitted to ITU and who died in the ED.
Descriptive analysis of initial prehospital NEWS presented by patient disposition
The means and 95% CIs of NEWS for each outcome group can be seen graphically in figure 2.

{kind=link}
{kind=link}
Mean NEWS and 95% CIs by patient disposition group. ITU, intensive therapy unit; NEWS, National Early Warning Score.
Risk category by patient disposition group
Retrospectively calculated risk categories were significantly associated with patient disposition p<0.001. Table 3 shows a clear pattern between and within patient disposition groups, where an increasing severity of risk level is associated with worsening outcome. In the low-risk group (n=158), the highest proportion of patients were discharged from ED (81%, n=81), with a declining trajectory of patients being admitted or dying (table 3). The opposite pattern was observed for patients with high NEWS risk scores, with few patients being discharged from ED and the majority dying. Looking at the cohort of patients who died in ED, 63% (n=19) was initially categorised as high risk, 24% (n=7) was medium risk and 13% (n=4) as low risk.
Patient disposition by NEWS clinical risk level
The relationship between risk level and outcome was further investigated using multinomial logistic regression analysis. This model was statistically significant p<0.001, explaining 37.8% (Nagelkerke R 2) of the variance and correctly classifying 47.4% of cases overall. Patients discharged from ED were 128 times more likely to be in the low risk category than those who died in the ED (p<0.001) (table 4).
ORs determined by multinomial logistic regression analysis (single predictor of clinical risk categories)
Discussion
EWSs are important tools indicating the likelihood of subsequent clinical deterioration. While the NEWS is recommended for ambulance service use, there is little evidence of its effectiveness in the ambulatory environment. There are also currently no recommendations regarding the urgency and scale of the clinical response that should be aligned to each risk category when used in the emergency prehospital setting.
We found strong associations between NEWS calculated from ambulance service clinical records and the severity of the patient’s condition as indicated by a proxy measure of patient disposition. Those with a higher NEWS risk category were more likely to be admitted to the ITU or die, whereas those with a low risk category were more likely to be discharged from the ED. This finding suggests that patients in the low risk category may be safely treated by ambulance clinicians and left at home, with NEWS informing clinical decision making. However, it is important to note that patients discharged from ED may have had further assessments and treatments undertaken at hospital that were necessary and outside of the standard remit of ambulance clinicians. Further research needs to explore the tests and treatments that discharged patients receive in ED, if any, and to investigate whether these are something that could be done in the prehospital environment. The inclusion of patients that reattend the ED after discharge and those who were not transported to a hospital (eg, those left at the scene or referred to another healthcare provider) would also help determine whether the NEWS could be beneficial in supporting transportation decisions.
There were a small number of low-risk patients in our study who subsequently died in ED; this finding highlights the importance of using NEWS and any associated guidance, alongside the ambulance clinicians’ skill set rather than replacing experience and clinical judgement.
We found no significant differences between NEWS calculated soon after arrival of the ambulance clinician and those calculated later in the prehospital care episode; this finding has important implications for prehospital implementation. Although statistically the time that the NEWS is assessed does not seem to influence the score, clinically the timing of the calculation is likely to be important. By calculating the NEWS as early as possible, decisions regarding transportation and whether an ED prealert is required can be made sooner so that those with the highest clinical needs reach definitive care most quickly. However, there is also an argument for calculating NEWS later in the prehospital episode once treatment has had a chance to take effect. This would allow the clinician to take account of any changes in the patient’s condition as a result of prehospital intervention. Further research into the best time to calculate NEWS would be beneficial.
It is a limitation of this study that NEWS was calculated retrospectively from the clinical paperwork rather than calculated by clinicians at the time of the assessment. However, as the documented observations were objective standard measurements, we have no reason to believe that they would have yielded different scores had they been calculated prospectively. The argument that our methodology is unlikely to have impacted the validity of our study is further strengthened by the similar findings reported in Silcock et al’s prospective study, which reported an association between high NEWS and incidence of adverse outcomes.17 A prospective methodology may have been helpful in reducing the number of missing observations recorded on the ambulance service paperwork, which resulted in small sample sizes for some patient disposition groups (those admitted to the ITU or who died in the ED). Given the emergency nature of the ambulance environment, it is not surprising that documentation is sometimes incomplete when the clinical care of the patient and the prompt transportation to hospital takes priority.
Hospital data beyond the ED were not available to us and could have provided potentially useful information about subsequent deterioration or improvement. It is unfortunately a common occurrence that hospital outcome data are not routinely available to ambulance services due to a lack of infrastructure and resources that would enable data matching and linkage. The data that were shared with us from the EDs occurred due to a wider project that is currently underway attempting to ensure prehospital and hospital data sharing. If successfully implemented such data sharing could dramatically enhance prehospital research and audit.
Our findings suggest that NEWS could successfully be utilised in the prehospital emergency setting to predict those most likely to deteriorate and inform clinicians’ decision making. Using the NEWS to standardise assessments within both the hospital and the pre-hospital setting will allow a consistent approach and more efficient handover. It would also provide hospitals with the ability to track trends of the NEWS for a longer period showing improvement or deterioration of the patient from the time that they were attended by the ambulance service. Prehospital guidance is needed linking the NEWS risk levels to decisions regarding patient destination and, if transported to hospital, whether they need to be prealerted to the arrival of the patient.
Acknowledgments
The authors would like to acknowledge the Imperial College Healthcare NHS Trust for providing the ED outcome data, and Kate Grayson, Statistics by Design, for her expert advice and analysis support.
Footnotes
Contributors JS, RF, SC and FM conceived and designed the work. JS managed the research and, along with SC, collected the data. JS analysed the data. JS and RF interpreted the data. JS and RF drafted the paper, and all authors reviewed it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. JS and RF are the guarantors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.