Article Text

Abstract
Background/aim Resistance training is an exercise modality at which overweight and obese adolescents can excel and which can therefore positively affect their psychological well-being. The aim of this study was to determine the effect of a 6-month resistance training intervention on the self-concept strength and body composition of overweight and obese adolescent males.
Methods 56 overweight and obese males aged 13–17 years were randomly allocated to an Intervention (n=30) or Control (n=26) group. Primary (psychological) and secondary (strength and body composition) outcomes were assessed at baseline as well as at 3 (halfway through the intervention), 6 (immediately postintervention) and 12 months follow-up. Random effects mixed modelling was used to determine the effects of the intervention.
Results Statistically significant differences between the Intervention and Control groups were observed at 3-month and 6-month assessments for exercise self-efficacy, resistance training confidence and self-esteem. Large increases in strength for the Intervention group, relative to Controls, were also observed with no substantial changes in body composition shown for either group. Values for all variables returned to baseline following completion of the programme.
Conclusions A 6-month resistance training intervention can positively affect the self-concept and strength of overweight and obese adolescent boys.
- Children's health and exercise
- Adolescents
Statistics from Altmetric.com
Introduction
About 20–25% of adolescents in Australia are overweight or obese.1 The physical health-related consequences of overweight in this population are well documented2; however, less attention has been directed towards psychological impacts.3 ,4
Typically, aerobic exercise is recommended for overweight and obese adolescents.5–9 Aerobic exercise, however, does not provide overweight or obese adolescents with the best chance to compete evenly with their leaner peers, given the higher physical and physiological demands placed on them due to their larger size.10 For this reason, participation in aerobic exercise (especially in front of others) is usually avoided by overweight and obese adolescents in the hope that they will not be further ridiculed by their peers,11 and as such, adherence and compliance to such programmes can be problematic.12
Alternatively, resistance training offers a number of physical health-related benefits, such as improved body composition and increased strength.13–21 It is an exercise modality at which overweight and obese adolescents can excel relative to their non-overweight peers, given their larger fat-free mass.10 This success then has the potential to have a positive effect on their self-concept (or self-esteem) through improving exercise self-efficacy (ie, confidence to exercise) and physical self-worth (ie, self-perception of their physical ability and appearance).22 ,23
Despite the potential psychological benefit of resistance training, we have been unable to find a single study using a resistance training only intervention that has examined its effects on the psychosocial status of overweight and obese adolescents. Furthermore, only two studies using a resistance training only intervention employed a randomised controlled trial design (but did not measure psychosocial outcomes).17 ,21 The aim of the current study was to determine the effect of a 6-month resistance training intervention on the strength, body composition and self-concept of overweight and obese adolescent males, using a randomised controlled trial design. This study was registered with the Australia and New Zealand Trials registry (ACTRN12609001078246).
Methods and procedures
Participants
Adolescent male participants, considered to be very overweight or obese using Cole's criteria,24 were recruited from the Adelaide metropolitan area using a number of different processes (eg, newspaper advertisements, advertisements in school newsletters and flyers at community places of interest). Very overweight was defined as being above the mid-point between the age-sex specific body mass index (BMI) cut-offs for overweight and obese (eg, if the age–sex specific BMI cut-offs for overweight and obesity were 23 and 25, respectively, then the BMI cut-off for very overweight was calculated to be 24.0).
Participants who met the following inclusion criteria were invited to take part: (1) aged 13–17 years at their last birthday; (2) BMI ≥ age–sex specific cut-off; (3) Tanner stage ≥2; (4) categorised as a low or moderate risk by the Sports Medicine Australia screening questionnaire25 or, if categorised as high risk, obtained a medical clearance from their general practitioner and (5) had no history of injuries or musculoskeletal conditions.
Procedures
Orientation session
Prior to baseline assessments, each participant was required to attend an orientation session run by one of the trainers who was involved with the 6-month resistance training programme. The purposes of the orientation session were as follows: (1) to familiarise participants with the machines/exercises they would be using during their strength assessments and resistance training programme (if in the Intervention group); (2) to estimate one-repetition maxima for lower and upper body strength measures, which would be used to guide their strength testing and (3) to determine a starting load (10-repetition maximum) for each of the exercises comprising their resistance training programme (if in the Intervention group).
Assessment sessions
Participants were measured at the following four time points throughout the study: baseline (week following screening and orientation); 3 (halfway through the intervention); 6 (postintervention) and 12 months (follow-up, ie, 6 months after completion). All outcome variables (with the exception of DEXA which the lead author conducted) were conducted by trained research assistants who were blinded to group allocation. Participants were randomised (after baseline) to either the Intervention or Control conditions using a random number generator.
Table 1 shows the outcome variables, the tests used, the measurement points and the time taken per measurement.
Outcome variables measured at each time point
Self-efficacy
Exercise self-efficacy was measured by the Exercise Self-Efficacy questionnaire.26 Participants were required to indicate, using a five-point Likert scale, how confident they were that they could exercise when faced with different situations (eg, I am tired, my friends ask me to go out). The internal consistency of the questionnaire in adolescents (for 10 items) is very high (Cronbach's α=0.85).26
A modified version of the Resistance Training Self-Efficacy and Outcome Expectancy questionnaire27 was used to assess participants’ confidence and beliefs about resistance training specifically, using a five-point Likert scale. Cronbach's α values for this scale (in adolescents) are 0.75 and 0.83, respectively.27 Test-retest reliability is very good with intra-class correlation coefficients ranging from 0.69 to 0.88.28
Physical self-worth
Global physical self-worth was assessed by the Physical Self-Worth (PSW) scale.29 To minimise socially desirable responses, the PSW scale uses a four-choice structured alternative format (eg, one scenario presented to participants is as follows: ‘Some kids are proud of themselves physically’, but ‘Other kids don't have much to be proud of physically’). Test–retest reliability in adolescents (over 2 weeks) is very good with an intraclass coefficient of 0.86.30
Self-esteem
Self-esteem and its different components were measured by the Self-Perception Profile for Adolescents (SPPA),31 using the same four-choice structured alternative format and scoring scale as the PSW scale. SPPA demonstrates very good internal consistency (Cronbach's α=0.74–0.92).31 Convergent validity with grades, peer integration and physical activity participation is weak to very strong (r=0.21–0.77).32
Body composition
Body mass was measured using the Tanita (Tanita Corporation, Japan) or SECA (GMBH & Co., Germany) scales and stretch stature using the Height Measure stadiometer (Invicta Plastics Ltd., Leicester). Skinfolds were also measured (biceps, triceps, subscapular, iliac crest, supraspinale, abdominal, front thigh and medial calf) to calculate a sum of skinfolds measure, using Harpenden calipers. Stature, mass and skinfold measurements were taken using the International Society for the Advancement of Kinathropometry (ISAK) protocols33 and all research assistants were ISAK Level 2 trained anthropometrists who demonstrated intratester technical errors of measurement of <1.3% (girths) and <4.5% (skinfolds).
Body composition (per cent body fat, lean mass and bone mineral density) was assessed using whole body DEXA scanning using a Lunar scanner (Lunar Prodigy: Lunar Radiation Corp., Madison, Wisconsin). In our laboratory, repeated measures using DEXA show coefficients of variation for repeated measurements for total body scanning using DEXA, which are as follows: 2.1% for per cent body fat; 1.5% for fat mass; 2.1% for lean mass; and 1.3% for bone mineral density. The coefficient of variation for percent body fat relative to the criterion four-compartment model is 1.6%.34
Strength
Absolute upper and lower body strength was measured by the one-repetition maximum for the bench (using a Smith machine) and leg press (using an incline leg press) exercises. One-repetition maximum testing has been shown to be a safe measure of absolute strength for adolescents35 with a coefficient of variation for repeated measures of <7%.15
Intervention
Intervention participants undertook a 6-month resistance training programme in one of two gymnasia, supervised by undergraduates in exercise science who had passed an undergraduate resistance training course. A maximum participant to trainer ratio of 4:1 was maintained throughout the study and participants trained with a buddy (another participant from the Intervention group) where possible.
The programme consisted of three 75 min sessions per week on non-consecutive days. Each session included a 10 min warm-up, 60 min of resistance training, and a 5 min static stretching cool down. A total of 10 separate multijoint exercises and single-joint exercises for major muscle groups were trained during each session. Weight-stacked machines and free-weight exercises were used, including bench press, leg press, lat pulldown, leg curl (lying or seated), shoulder press (seated), seated row, biceps curl, triceps pressdown, calf raise (seated) and abdominal crunch. Table 2 shows the progression of the resistance training programme over a 6-month period. Control participants were instructed to continue with their normal everyday activities. At completion of their 12-month assessment, all Control participants were offered a complimentary 3-month gym membership.
Progression of the 6-month resistance training programme
Statistical analysis
Power calculation
With two groups and four measurement points for the primary outcome variables (exercise self-efficacy, physical self-worth and self-esteem), a sample size of 17 per group was required to detect a moderate effect size (Cohen's d) of 0.5 with 80% power and α of 0.01 (to allow for multiple comparisons).
Statistical procedures
Participants’ demographic data were analysed descriptively. t Test, Mann-Whitney and χ2 analyses were used to determine if there were baseline differences between the groups for demographic characteristics. Programme adherence was quantified as the percentage of intended training sessions attended.
The effect of the intervention on outcome measures was determined using random effects mixed modelling (REMM) to compare mean changes in the key outcome variables between groups at each measurement point (baseline, 3, 6 and 12 months).36 Sequential Bonferroni correction was applied to post hoc analyses, and analysis was performed on an intention-to-treat basis. Using raw descriptive summary statistics, standardised effect size (ES) changes relative to baseline measures for the Intervention and Control groups were calculated for all outcome variables at each measurement point along with the corresponding 95% CIs. Effect sizes were described as very small (<0.2), small (≥0.2 and <0.5), moderate (≥0.5 and <0.8) or large (≥0.8).37
Mediation effect analysis38 was run (for the Intervention group only) to determine whether changes in the primary outcome variables were mediated by changes in strength and/or body composition. The independent variable was training attendance, the dependent variables were the calculated change scores relative to baseline, for exercise self-efficacy, physical self-worth and self-esteem with the calculated change scores relative to baseline, for strength, body composition and exercise self-efficacy as the mediators. Analysis was run for 3-month (using attendance, as a percentage, after 3 months of the resistance training programme), 6-month and 12-month assessments (using attendance, as a percentage, at completion of the resistance training programme). Both direct and indirect effects were calculated.
Results
A total of 56 participants attended baseline testing and were randomly allocated to the Intervention (n=30) or Control (n=26) group. They were included in the analysis at all subsequent assessment sessions. Figure 1 shows how participants progressed through the study and how many participants completed each stage. At completion of the 6-month resistance training programme, the average attendance of all participants (who had not dropped out before their 6-month assessment, n=27) was 74% (ie, an average of 58 of 78 sessions were attended).

Flow chart of how participants progressed through the study and how many participants completed each stage.
Table 3 shows the descriptive summary statistics for basic physical (age, stature, mass, BMI) data for the Intervention and Control groups recorded at screening and baseline testing. The Control group had significantly lower scores on the social acceptance and close friends subscales of the SPAA questionnaire.
Descriptive summary statistics for age and basic physical data recorded at baseline assessment
Psychological outcomes
Table 4 shows the REMM analysis results for all psychological outcomes. For all questionnaires and their subscales, a higher score (or positive ES change) indicates higher self-efficacy/confidence or beliefs/self-perception.
Psychological REMM results table
For exercise self-efficacy, there were large and statistically significant differences between the Intervention and Control groups (for raw scores) at 3 and 6 months (ES: 0.88 and 0.83, respectively; table 4 and figure 2) with the results in favour of the Intervention group. There were no statistically significant differences between the Intervention and Control participants for resistance training beliefs; however, there were large and statistically significant differences between the two groups (for raw scores) at 3, 6 and 12 months for the resistance training confidence subscale (ES: 0.90, 0.93 and 0.97, respectively; table 4 and figure 2).
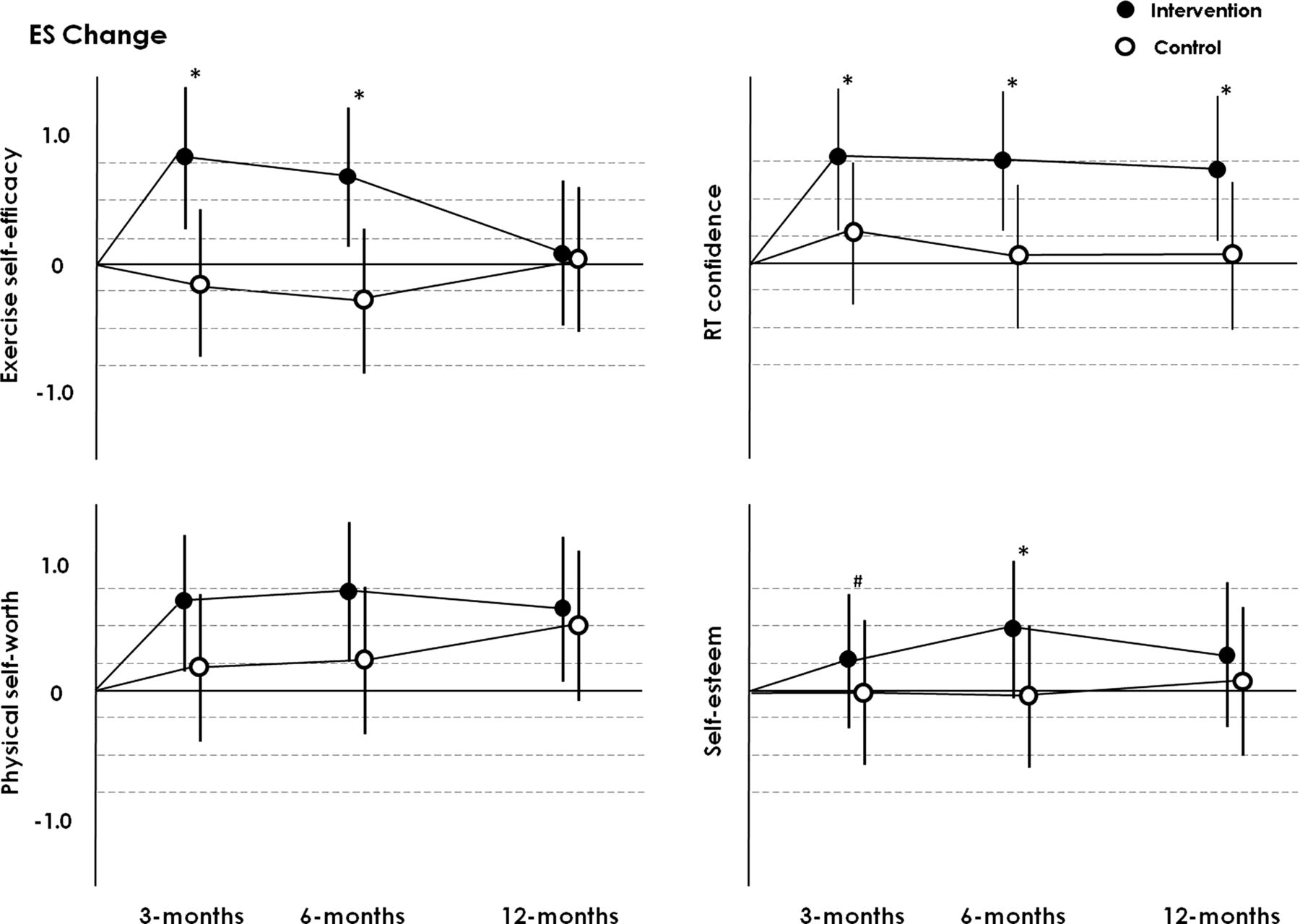
Effect size change scatterplots for the psychological outcomes. Note: Dotted lines show the thresholds for small, moderate and large. ES, effect size; RT, resistance training; #, significant difference (p<0.05) between the Intervention and Control groups (raw scores) at a given time point; *, significant difference (p<0.05) between the Intervention and Control groups (raw scores) at a given time point after Bonferroni correction.
Positive trends relative to baseline measures were shown for both groups for physical self-worth; however, there were no statistically significant differences between the Intervention and Control participants (table 4 and figure 2). There were moderate to large and statistically significant differences (ES: 0.57 and 0.86) between the Intervention and Control groups (for raw scores) at 3-month assessments and 6-month assessments, respectively, for global self-esteem, in favour of the Intervention group (table 4 and figure 2).
Body composition
Table 5 shows the REMM analysis results for body composition outcomes. Increases are considered to be negative, with the exception of lean mass, where an increase is a positive result. There were no statistically significant differences between the Intervention and Control groups for any of the body composition outcomes (table 5).
Body composition REMM results table
Strength
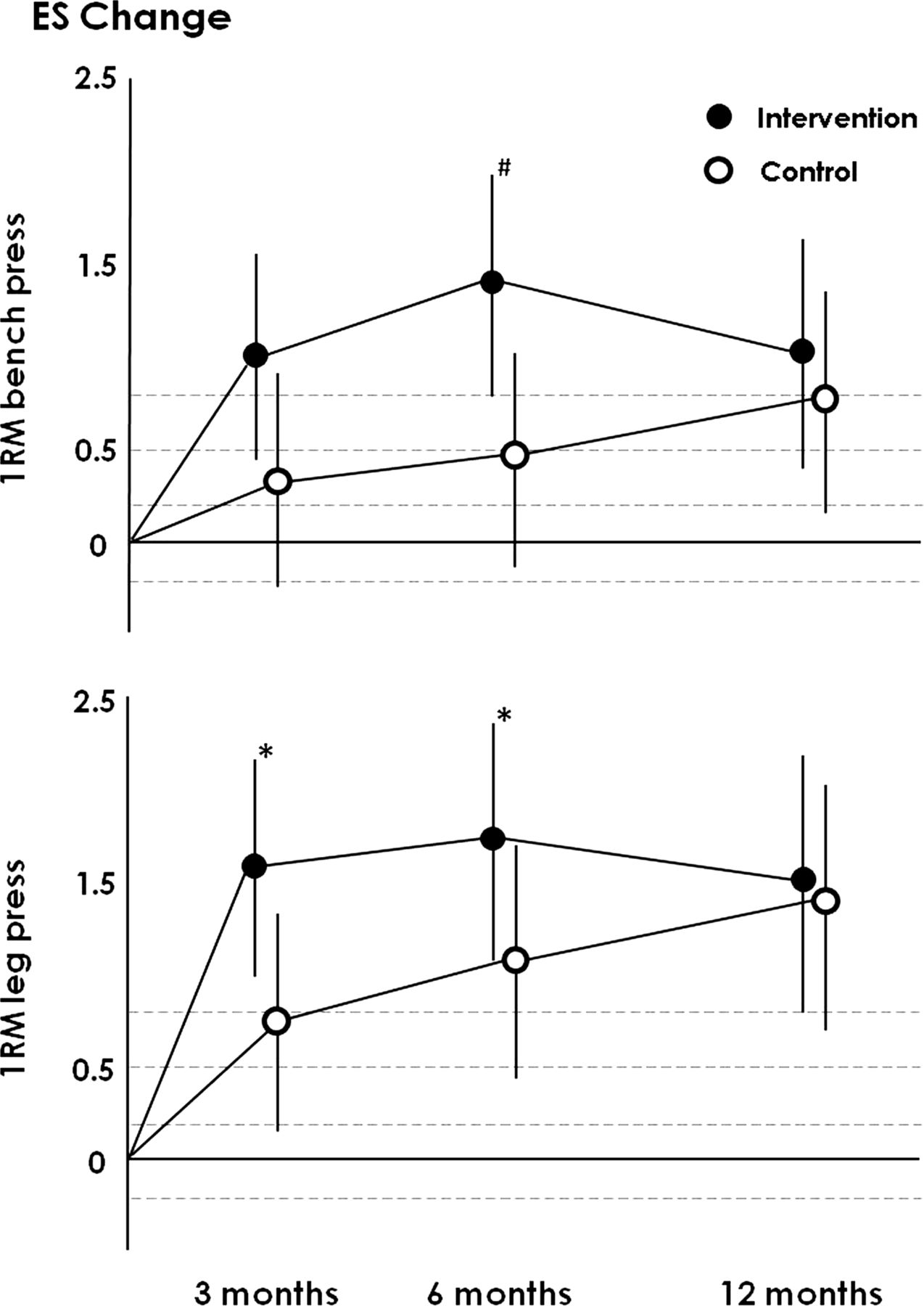
Table 6 shows the REMM analysis results for strength, with an increase (ie, a positive ES change) considered to be a positive result. There were moderate to large and statistically significant differences (for raw scores) between the Intervention and Control participants at 3 months for leg press (ES: 0.96) and at 6 months for bench and leg press (ES: 0.65 for both measures) in favour of the Intervention group (table 6 and figure 3).
Strength REMM results table

{kind=link}
{kind=link}
{kind=link}
Effect size change scatterplots for strength. Note: Dotted lines show the thresholds for small, moderate and large. 1RM, one repetition maximum, ES, effect size; #, significant difference (p<0.05) between the Intervention and Control groups (raw scores) at a given time point; *, significant difference (p<0.05) between the Intervention and Control groups (raw scores) at a given time point after Bonferroni correction.
Mediation analysis
There were no significant indirect effects at 3, 6 or 12 months for any of the primary outcome variables. In addition, there were no consistent relationships shown for any of the direct effects.
Discussion
In this study, a 6-month resistance training intervention for overweight and obese adolescent males had a moderate-to-large effect on exercise self-efficacy, resistance training confidence, self-esteem and strength relative to controls and no substantial effect on body composition. However, the statistically significant between-group differences observed during the 6-month training period were not apparent at 12 months. Changes in psychological outcomes were not mediated by changes in strength or body composition. In relation to strength and body composition, these results are similar to those of previous studies that have used a resistance training intervention,14–21 ,39 with very small to small and non-significant effects shown for body composition and moderate-to-large effects shown for strength.
While no previous studies have examined the effects of resistance training on psychological outcomes for overweight and obese adolescents, there are studies that have examined these effects on the general population.40 ,41 A study conducted by Valez et al40 recruited 15 Hispanic adolescents to take part in a resistance training intervention three times a week for 12 weeks, while a study run by Morgan et al41 recruited 50 ‘low active’ adolescent boys (attending low socioeconomic status schools) to participate in a 6-month school-based multicomponent intervention with a focus on resistance training. Both studies assessed the same psychological outcomes as those in this study utilising the same assessment tools. Small to large improvements in physical self-perceptions were reported with significant changes (relative to Controls) shown for physical self-worth (ES: 0.33)41 and global self-worth (or self-esteem) (ES: 1.04).40 Moderate and statistically significant changes (relative to Controls) were also reported for resistance training self-efficacy at the completion of the 6-month intervention period (ES: 0.75).41 These results are comparable to those reported in this study.
Self-concept (measured by self-esteem) is a multidimensional hierarchical construct that can be modified by many factors.22 Given the structure of self-concept and the Exercise Self-Esteem Model (ie, changes in self-efficacy will affect changes in physical self-worth and then self-concept),42 one could speculate that changes in direct measures (strength and body composition) would directly influence self-efficacy through the mastery of skill, which could then flow on to positively affect physical self-concept. Ultimately, these changes could have an effect on self-concept if the stimulus was applied for long enough (ie, at least 6 months).23 This study did not support this model as there were no substantial changes in body composition, and the changes in the primary psychological outcomes (self-efficacy, physical self-worth and self-esteem) were not mediated by changes in strength. Why then did the psychological profiles of participants improve during the programme?
Global self-concept can also be influenced by one's emotional and social concept, which are alongside physical self-concept in the hierarchical model.22 Therefore, at the specific situational level, having a positive effect on one's social interaction (with peers and significant others) and emotional state could potentially have the same positive flow-on effects for global self-concept.22 Therefore, it is feasible to suggest that the same improvements in psychological outcomes could occur for any intervention as long as positive social interactions are experienced. However, this is unlikely given that there were improvements in exercise self-efficacy and physical self-worth, not just self-esteem. Even though these changes were not mediated by changes in strength or body composition, the participants still perceived that their strength and appearance improved and without these improved self-perceptions, the overall enhancement in self-esteem may not have resulted. We recommend that future studies investigating the effect of any exercise intervention on psychological well-being include a non-exercise placebo group, which mirrors the social interaction experience of the Intervention group, to determine whether similar effects on psychosocial outcomes are observed.
Strengths and limitations
Only a handful of other studies targeting overweight and obese adolescents have used a resistance training only intervention strategy.14–21 ,39 In comparison to these, this study exhibited a number of strengths. First, a randomised controlled trial design was employed, which provides the strongest level of evidence when examining the effects of an intervention.43 Second, this study has examined the effects of resistance training on the largest sample of overweight and obese adolescents until now, and the duration of the intervention programme and the volume of training prescribed to participants surpasses that of previous studies. This study also assessed participants at mid-intervention and at a 6-month follow-up which has not been previously performed.
This study is the first to examine the effects of resistance training on the psychological well-being of overweight and obese adolescent males. The tools used to assess psychosocial variables included various subdomains to ensure that the multifaceted nature of global self-concept and physical self-worth was examined. While the effects of resistance training on body composition and strength have been widely examined, this study has employed both criteria and indirect measures to capture a more complete picture (eg, one-repetition maximum testing, DEXA and physical measures).
Stereotypically, resistance training is a masculine activity that may improve self-perception in adolescent boys at a stage in their lives when they are constructing their identities.44 It was therefore thought that recruitment and adherence to the programme would be better with an all-male cohort. The recruitment of only adolescent males means that the effect of resistance training on the psychological well-being of overweight and obese adolescent females is still unknown. This study is also limited by the lack of a control group experiencing social interaction that can positively influence psychological well-being.
Conclusion
A 6-month resistance training intervention can positively affect certain aspects of self-concept and the strength of overweight and obese adolescent males but appears not to substantially affect body composition. Upfront, these results seem quite straightforward and positive. However, further research is still needed if we want to have a significant and lasting impact on the physical and psychological well-being of overweight and obese adolescents, as this study has shown that once the stimulus has been removed, participants typically return to baseline. The mechanisms behind how exercise participation can improve the self-concept of overweight and obese adolescents need further examination, and the inclusion of sustainable community or school-based programmes are imperative if any improvements in strength and self-concept are to be maintained.
What are the new findings?
-
A 6-month resistance training intervention has a moderate-to-large effect on the exercise and self-esteem of overweight and obese adolescent males, relative to Controls.
-
Changes in psychological outcomes were not mediated by changes in strength and body composition.
-
At the12-month follow-up, all positive changes had returned to baseline.
How might it impact on practice in the near future?
-
The inclusion of resistance training in sustainable community or school-based programmes to maintain positive changes in psychological outcomes.
-
Highlights the importance of including a non-exercise placebo group to evaluate the social interaction impact on self-concept.
-
Shows that there is a need to design sustainable programmes that can have a positive effect on not only psychological outcomes but also physical outcomes such as body composition.
Acknowledgments
The authors would like to thank all the participants and their parents/guardians for their involvement with the study. They would also like to acknowledge all the trainers who volunteered their time and the University of South Australia HLS Health and Fitness Centre (Health Solutions) and the YMCA Aquadome Health and Fitness Centre for the use of their facilities. We would like to dedicate this article to our friend and colleague, JP, who, during the preparation of this manuscript, suddenly died from a heart attack. John, we sincerely thank you for all of your statistical support over time. Your statistical knowledge, selfless work ethic and outstanding ability to communicate and educate was unparalleled and will be sorely missed.
References
Footnotes
-
Contributors NS was responsible for designing the study, data collection, interpreting the results, writing the manuscript and making changes to each subsequent draft. GT, TS and NP provided guidance in study design and interpretation of the results and also reviewed each draft of the manuscript before submission. JP conducted all statistical analysis and assisted with interpretation of the results.
-
Competing interests NP is supported by the National Health and Medical Research Council Programme Grant funding (# 320860 and 631947).
-
Ethics approval University of South Australia Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.