Article Text

Abstract
Purpose The aim of this study was to determine whether iron treatments improve the iron status and aerobic capacity of iron deficient non-anaemic endurance athletes.
Method A meta-analysis of studies that investigated the effects of iron treatment on serum ferritin (sFer), serum iron (sFe), transferrin saturation (Tsat), haemoglobin concentration ([Hb]) and ( ). Seventeen eligible studies were identified from online databases.
). Seventeen eligible studies were identified from online databases.
Results Analysis of pooled data indicated that iron treatments had a large effect on improving sFer (Hedges’ g=1.088, 95% CI 0.914 to 1.263, p<0.001), sFe (Hedges’ g=1.004, 95% CI 0.828 to 1.181, p<0.001) and Tsat (Hedges g=0.741, 95% CI 0.564 to 0.919, p<0.001) and a moderate effect on improving [Hb] (Hedges’ g=0.695, 95% CI 0.533 to 0.836, p<0.001) and  (Hedges’ g=0.610, 95% CI 0.399 to 0.821, p<0.001). Regression analysis revealed a significant interaction between the effect of iron treatment on sFer and treatment duration, suggesting treatments that lasted beyond 80 days appear to have the least effect on sFer.
(Hedges’ g=0.610, 95% CI 0.399 to 0.821, p<0.001). Regression analysis revealed a significant interaction between the effect of iron treatment on sFer and treatment duration, suggesting treatments that lasted beyond 80 days appear to have the least effect on sFer.
Conclusions These results indicate iron treatments improve the iron status and aerobic capacity of iron deficient non-anaemic endurance athletes.
- Anaemia
- Iron metabolism
- Endurance
- Aerobic fitness
- Running
Statistics from Altmetric.com
Introduction
Endurance athletes are prone to negative changes in iron status caused by insufficient dietary intake, increases in haematuria, gastrointestinal bleeding, sweating and haemolysis.1 The effect of depleted iron stores on athletic performance depends on the severity of the iron deficiency, with the most severe cases impairing erythropoiesis (iron deficient anaemia, IDA).2 In such instances oxygen transport is reduced due to a fall in haemoglobin concentration [Hb], causing a decrease in aerobic capacity,3 and is often associated with symptoms of fatigue. However, when body iron stores fall, defined by a decrease in serum ferritin (sFer) or transferrin saturation (Tsat), the [Hb] in the blood can still remain above the level used to classify anaemia (Hb <12 g/dL). This is termed iron deficient non-anaemia (IDNA)
Although IDNA should not affect oxygen carrying capacity according to theory,4 ,5 animal6 and human7 studies reveal that IDNA negatively affects oxidative enzyme and respiratory protein activity. This provides a mechanism for IDNA to impair aerobic capacity in endurance athletes by reducing the ability to extract and utilise oxygen from haemoglobin. Indeed, in recent studies, indices of endurance performance8 ,9 and performance itself10 were impaired in IDNA athletes compared to those whose iron status was considered normal.
In clinical settings of hospitalised patients, anaemia is often a multifactorial issue, which manifests as either IDA or anaemia of chronic disease. Anaemia of chronic disease is characterised by the disruption of iron homeostasis initiated by a cytokine-mediated immune response, this can lead to functional iron deficiency, where normal iron stores are unable to be mobilised for erythrogenesis.11 Iron treatment has been effective in a wide variety of patient groups to improve haematological indices, iron status and postoperative/post-treatment outcomes.12–16
A similar process may occur in athletes where exercise-induced inflammation may upregulate hepcidin, the hormone considered to be the master regulator of iron absorption, thus reducing iron absorption from the gut and preventing iron recycling from macrophages and thereby causing iron deficiency.17 Given that IDA and IDNA can impair aerobic capacity and that iron treatments have helped clinical populations, we hypothesised that improving the iron status of iron deficient athletes would be beneficial. However, although iron treatment is a common intervention for athletes diagnosed with iron deficiency, definitive conclusions about the effectiveness of such treatment for IDNA are hindered by methodological variations in the current literature. These variations include the measures used to determine iron status and endurance performance, and the protocol undertaken for iron treatment.
Methods of iron delivery/treatment
Iron treatments can be administered to athletes orally or via intramuscular or intravenous injection. Oral iron absorption may be limited and restoration of total body iron stores takes 3–6 months.12 ,18 There is interest in the use of parenteral iron therapies in athletes but few investigations have utilised this method for IDNA athletes.18–21 Regardless of the method employed, iron treatment improves iron status in athletes3 ,5 ,18–35 but whether it improves aerobic capacity is not clear.
Utilising either oral or parenteral iron treatments has failed to enhance indices of aerobic capacity in some investigations19 ,26 ,31 ,32 ,34 but it was successful in others.5 ,23–25 ,27 ,28 ,35 A possible explanation for this apparent lack of agreement is the variation in the iron doses and methods of administration. Investigations on the effects of IDNA in endurance athletes have used doses well below those used successfully in clinical settings to improve patient iron status.36
Studies to date have assessed the efficacy of iron treatments to improve the iron status of athletes with varying degrees of IDNA and IDA, however, the subsequent impact of iron repletion on indices of aerobic capacity is not well reported. Variations in the method of administration and dosing protocol preclude the possibility of predicting the physiological and performance responses to such treatment. Thus, the aim of this meta-analysis was to describe the efficacy of iron treatments in iron deficient, non-anaemic athletes first to improve iron status and second to improve indices of aerobic capacity.
Methods
Literature search
A systematic review with meta-analyses was conducted in accordance with the established guidelines of the International Prospective Register for Systematic Reviews (PROSPERO, 2013). Details of the protocol for this review were registered on PROSPERO and can be accessed at http://crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42013005528. Combinations of the following terms were searched until November 2013 in three online databases (Web of Knowledge, Sports Discus on EBSCO and PubMed): endurance, exercise, performance, running, rowing, cycling, athlete, iron, deficient, anaemia, supplementation, repletion, oral, injection. The reference lists of all eligible articles were examined to identify any further eligible studies.
Outcome variables
The literature was examined for the effects of iron treatments on iron status and aerobic capacity. Iron status was assessed using measures traditionally used to determine iron status including [Hb], sFer, Tsat and serum iron (sFe). Maximal oxygen uptake ( ), obtained from the use of incremental exercise tests to exhaustion, was used as the measure of aerobic capacity.
), obtained from the use of incremental exercise tests to exhaustion, was used as the measure of aerobic capacity.
Inclusion and exclusion criteria
Studies were included on the basis of the following (1) the experimental design was required to be either a randomised control trial or non-randomised control trial; (2) participants were taking part in endurance exercise and were classified as being iron deficient but not anaemic based on sFer ≤35 µg/L and [Hb] >12 g/dL18; (3) participants were separated into at least one group receiving an iron treatment and one group receiving a placebo or no treatment; (4) iron treatment was the sole intervention strategy There were no sex, age or ethnicity-based exclusion criteria.
Extraction of data
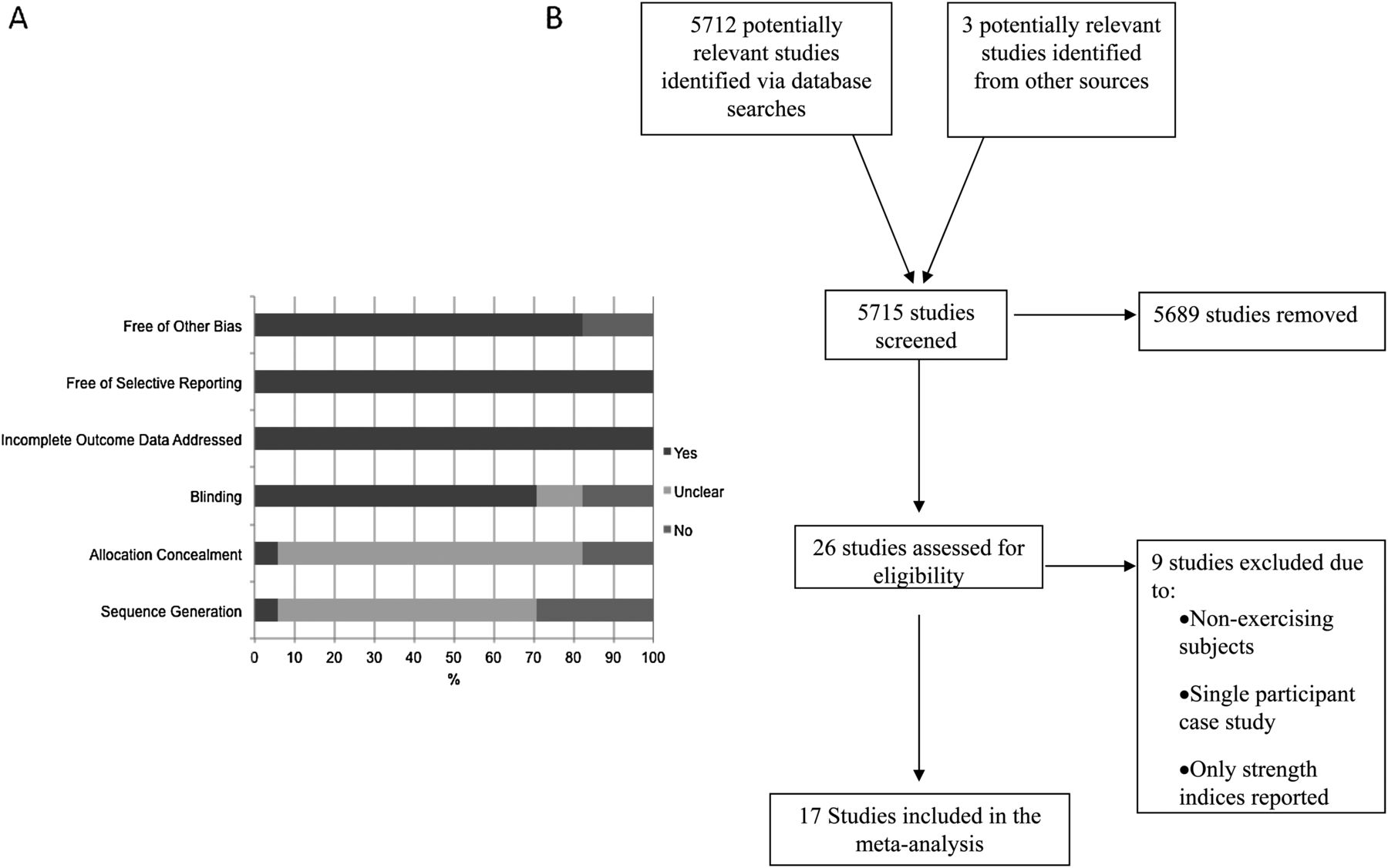
Mean and SD for all outcome variables were extracted from eligible studies, along with sample size and treatment method. Risk of bias was assessed in accordance with the Cochrane Collaboration (figure 1A).37
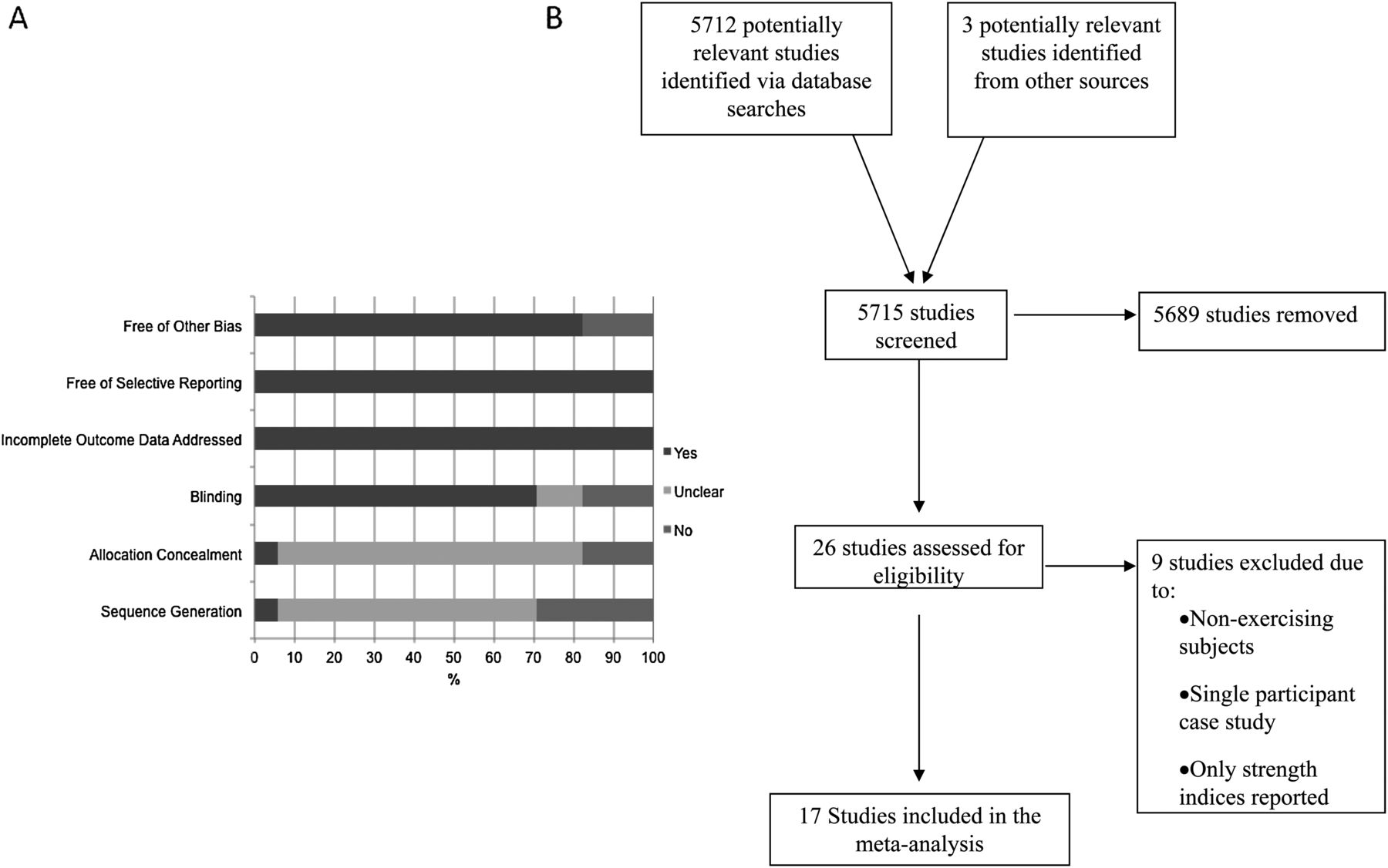
(A) Analysis of the risk of bias according to the Cochrane Collaboration guidelines.37 (B) Schematic of the study selection process from initial identification of eligible studies to final inclusion.
Statistical analysis
All analyses were conducted using Comprehensive Meta-analysis software (V.2.2.057, Biostat Inc, Engelwood, New Jersey, USA). Data were analysed using a fixed effect model. Hedges’ g with 95% CI was used to indicate the standardised mean differences. Effect sizes were set at <0.40=small, 0.40–0.70=moderate, >0.70=large.37 Heterogeneity was assessed using an I2 statistic that indicates the percentage of variability across the studies due to heterogeneity rather than chance.37 When I2 was >30% (30–60% represents moderate heterogeneity)37 a subgroup meta-analysis of sex was carried out to investigate the source of heterogeneity. If heterogeneity still existed in the subgroup meta-analysis, further subanalyses of treatment method and time post-treatment (0–4 weeks, 4–8 weeks, 8+weeks) were conducted. Meta-regression analysis was carried out using SPSS Predictive Analytics Software (IBM, Portsmouth, Hampshire, UK), whereby interactions between the effect sizes of the measured iron and exercise indices and variables of treatment protocol (dose per week, total dose and dose duration) were investigated. A significance level of p≤0.05 was applied.
Results
A total number of 5712 studies were identified via electronic database searches (figure 1B). An additional three studies were included from searches of relevant reference lists. Of the 5715 studies screened, 5689 were removed for not meeting the specified inclusion criteria and the remaining 26 studies were assessed for eligibility. Nine studies were excluded due to: untrained participants; single participant case studies; outcome variables that were not in accordance with the inclusion criteria. The 17 remaining studies that met the inclusion criteria had data extracted for the meta-analysis. The total number of participants in the eligible studies was 443 (n=80 men and n=363 women) with a mean and SD age of 22.3±5.1 years. A summary of the studies included in the meta-analysis is presented in table 1. The outcome of the risk of bias assessment indicated that sequence allocation and allocation concealment were generally unclear (figure 1A).
Summary of literature included in the meta-analysis
sFer meta-analysis
Iron treatment had a large effect on sFer (Hedges’ g=1.088, 95% CI 0.914 to 1.263, p=0.001; figure 2A), from a total of 25 extracted data points. The I2 statistic of 86.8% indicated high heterogeneity in the results. Consequently subgroup meta-analyses of sex and treatment method were completed (table 2). Iron treatment was effective for improving sFer in females (p=0.001) and males (p=0.014) and both intramuscular injection and oral iron treatments had a significant effect (p=0.001). Owing to substantial heterogeneity (table 2) a further subgroup meta-analysis for time post-oral treatment was completed, which revealed that oral iron treatment was effective at increasing sFer in females up to 8 weeks (p=0.001). No further subgroup analysis of heterogeneity for intramuscular injection treatment was completed due to the small number of studies (n=2).
Results of subgroup meta-analyses to investigate sources of heterogeneity from original meta-analysis

(A) Forest plot of meta-analyses illustrating comparison of iron treatment versus control treatment on serum ferritin levels in iron deficient non-anaemic (IDNA) endurance athletes. Numbers in brackets represent the number of days a post-treatment measurement was made. Squares indicate individual study Hedges’ g and the lines represent 95% CI. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges’ g, with the width of the diamond signifying the 95% CIs. (B) The interaction between the effect size for serum ferritin and the total duration of treatment in days within the extracted studies included in the meta-analysis.
sFe meta-analysis
Iron treatment had a large effect on increasing sFe (Hedges’ g=1.004, 95% CI 0.828 to 1.181, p=0.001; figure 3A) from a total of 22 extracted data points. There was substantial heterogeneity in the results, so subgroup analyses of sex, treatment method and time post-treatment were performed (table 2). sFe iron increased in females (p=0.001) and males (p=0.001), with both oral (p=0.001) and intramuscular injection (p=0.011) being effective treatment methods. Oral iron treatment had a large effect on sFe up to 8 weeks (p=0.001; table 2). No further subgroup analyses for males were carried out due to an n of only two studies.

Forest plot of meta-analyses illustrating comparison of iron treatment versus control treatment on serum iron (A) and transferrin saturation (B) levels in iron deficient non-anaemic (IDNA) endurance athletes. Numbers in brackets represent the number of days a post-treatment measurement was made. Squares indicate individual study Hedges’ g and the lines represent 95% CI. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges’ g, with the width of the diamond signifying the 95% CIs.
Tsat meta-analysis
Tsat was significantly increased following iron treatment (Hedges g=0.741, 95% CI 0.564 to 0.919, p=0.001; figure 3B) from 21 extracted data points. Owing to substantial heterogeneity subgroup analyses of sex, treatment method and time post-treatment were conducted and revealed that iron treatment had a large effect on females (p=0.001) and a moderate effect on males (p=0.024). Both oral (p=0.001) and intramuscular injection (p=0.004) methods had a large effect on Tsat in females, with oral treatment producing large effects up to 8 weeks (p=0.001). No further subgroup analysis of heterogeneity for males was completed due to the small number of studies (n=2).
[Hb] meta-analysis
Iron treatment had a moderate effect on [Hb] (Hedges’ g=0.695, 95% CI 0.533 to 0.836, p=0.001; figure 4A) from 25 extracted data points. High heterogeneity was revealed (table 2) so subgroup analyses for sex, treatment method and time post-treatment indicated that iron treatment had a larger effect on [Hb] in women (p=0.001) than men (p=0.036). Oral treatments (p=0.001) and intramuscular injections (p=0.013) were effective at increasing [Hb], with large effects present up to 8 weeks after oral treatment (p=0.001; table 2).

Forest plot of meta-analyses illustrating comparison of iron treatment versus control treatment on haemoglobin concentration levels (A) and  (B) in iron deficient non-anaemic (IDNA) endurance athletes. Numbers in brackets represent the number of days a post-treatment measurement was made. Squares indicate individual study Hedges’ g and the lines represent 95% CI. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges’ g, with the width of the diamond signifying the 95% CIs.
(B) in iron deficient non-anaemic (IDNA) endurance athletes. Numbers in brackets represent the number of days a post-treatment measurement was made. Squares indicate individual study Hedges’ g and the lines represent 95% CI. The size of the square is proportional to the weight of the study within the meta-analysis. The diamond represents the overall Hedges’ g, with the width of the diamond signifying the 95% CIs.
 meta-analysis
meta-analysis

The meta-analysis of 15 extracted data points revealed iron treatment had a moderate effect on  (Hedges’ g=0.610, 95% CI 0.399 to 0.821, p=0.001; figure 4B) with an I2 statistic of 70.3%. A subanalysis for sex was not possible as
(Hedges’ g=0.610, 95% CI 0.399 to 0.821, p=0.001; figure 4B) with an I2 statistic of 70.3%. A subanalysis for sex was not possible as  was not included in the two male only studies. Therefore, a subanalysis for treatment method indicated that only oral treatments had a significant effect on
was not included in the two male only studies. Therefore, a subanalysis for treatment method indicated that only oral treatments had a significant effect on  (p=0.001) with moderate heterogeneity. A further subgroup analysis revealed a significant effect at all time points (p=0.004; table 2).
(p=0.001) with moderate heterogeneity. A further subgroup analysis revealed a significant effect at all time points (p=0.004; table 2).
Regression analysis
Meta-regression was carried out to determine interactions between treatment protocol variables (dose per week, total dose and dose duration) and sFer, sFe, Tsats, [Hb] and  . A significant interaction between effect size for sFer postiron treatment and treatment duration was revealed (β −0.021, p=0.014; figure 2B), with treatments that lasted beyond 80 days appearing to have the least effect on sFer. No other significant interactions were indicated.
. A significant interaction between effect size for sFer postiron treatment and treatment duration was revealed (β −0.021, p=0.014; figure 2B), with treatments that lasted beyond 80 days appearing to have the least effect on sFer. No other significant interactions were indicated.
Discussion
This meta-analysis focused on endurance athletes with iron deficiency without anaemia. Our results suggest that iron treatment has a moderate to large effect on improving iron status (sFer, Hedges’ g=1.088) and a moderate effect on improving aerobic capacity ( ) (Hedges’ g=0.610).
) (Hedges’ g=0.610).
Iron status
Ferritin is commonly used as a marker to reflect the whole body iron status.38 ,39 Ferritin levels increase after exercise as a consequence of the acute phase inflammatory response.1 Furthermore, the combined effects of training-induced iron losses via gastrointestinal bleeding, sweating and haemolysis1 and the inflammation mediated upregulation of hepcidin, which impairs iron absorption,11 ,17 ,18 ,40–42 may contribute to the decreased ferritin levels reported in IDNA endurance athletes. The potential for athletes with consistently low ferritin levels to develop IDA may be a concern. There is evidence that [Hb] remains stable despite low sFer,21 suggesting that the risk of IDNA athletes developing IDA is small, providing dietary practices remain adequate. The optimal sFer level for athletes is not known, yet low ferritin is associated with oxidative stress43 and therefore treating IDNA endurance athletes may be desirable. Our results indicate that low ferritin levels can be significantly increased with iron treatment (Hedges’ g=1.141, p<0.001; figure 2A) in IDNA endurance athletes.
Serum iron and Tsat are also used to indicate iron status. Iron is transported through the circulation via the protein transferrin, whose ability to bind with transferrin receptors on cells is determined by iron saturation.38 ,39 Accordingly, the lower the Tsat, the lower the cellular iron uptake. Thus, the desirable outcome of iron treatment would be increases in both sFe and Tsat. Our results suggest that iron treatment does have a large effect on both sFe (Hedges’ g=0.966, p<0.001; figure 4) and Tsat (Hedges’ g=0.730, p<0.001; figure 3). However, this finding should be interpreted with caution if one intends is to use these measures to indicate iron status or a positive response to treatment because some individual studies showed no change after treatment.15 ,19 ,25 ,27 ,28 ,31 ,34 ,35 ,39 ,41 The treatment failure common to these studies suggests that the IDNA was not severe enough for an intervention to impact iron status. Differences between the pretreatment sFer levels may explain the variation in the response of both sFe and Tsat in the included literature. Although, finding an effect of iron treatment on sFe and Tsat in this meta-analysis despite some of the individual studies failing to do so may be a consequence of the different statistical approaches adopted.
The vast majority of iron supplementation research has used traditional statistics to determine the significance of an intervention, the use of effect sizes is gaining popularity, particularly when elite athletes are the investigated population.20 Small changes that are meaningful to athletes and are identified by effect sizes may not be recognised using traditional p values.44
The variations in response to iron treatment adds weight to the contention that sFe and Tsat may not be sensitive enough to be stand-alone markers of whole body iron status.45 Measurements of sFe can be affected by large day-to-day biological variation.46 Moreover, the use of soluble transferrin receptor (sTfR) in conjunction with sFer and Tsat may provide greater sensitivity for the diagnosis of iron deficiency. sTfR is not an acute phase protein and therefore is not affected by exercise-induced inflammation;2 investigations have shown little variability in sTfR under endurance conditions.47–49 Thus, sTfR can be used as a marker of iron status when tissue iron deficiency occurs50 and should be included in studies investigating the iron metabolism of endurance athletes. Nevertheless, caution should also be exercised with measurements of sTfR, as there is variability in the performance of commercially available assays and a lack of an international standard,51 which can make comparisons of sTfR values difficult.
Aerobic capacity
The effect of depleted iron stores on  may depend on the severity of the iron deficiency. In the most severe cases when the reduction of sFer leads to an impairment of erythropoiesis,2
may depend on the severity of the iron deficiency. In the most severe cases when the reduction of sFer leads to an impairment of erythropoiesis,2  is reduced due to a fall in [Hb], causing a subsequent decrease in oxygen transport capacity.18 Conversely, IDNA is characterised by a reduction in ferritin without [Hb] falling below 12 g/dL,5 ,8–10 ,18 ,19 ,22 ,24 ,26–28 ,31 ,32 ,34 ,35 ,52 so the maintenance of [Hb] should mean that oxygen carrying capacity is not affected,4 ,5 and exercise performance maintained.8–10 ,21 Despite having initial [Hb] values within the normal range, our study indicates that iron treatment has a moderate effect on [Hb] (Hedges’ g=0.670, p<0.001; figure 4A). It is plausible that increases in [Hb] following iron treatment are related to the initial iron status and [Hb] of the athlete. For example, the studies included in this review that showed the largest effect sizes for [Hb] had initial sFer <10.80 µg/L25 ,30 and [Hb] <12.5 g/dL.27 ,28 ,32 This may indicate that the overall effect size for [Hb] was influenced by those studies whose populations had an initial [Hb] at the lowest end of the normal range for an endurance athlete. The influence of iron treatment on [Hb] in IDNA athletes should not be dismissed, as it has been suggested that although iron treatment may not elevate [Hb], it may serve to prevent an otherwise detrimental reduction, which would place the athlete at a greater risk of developing IDA.22 ,35 Furthermore, the suitability of [Hb] as an indicator of iron status should be questioned on the basis that it is influenced by haemodilution and plasma volume shifts, and therefore likely to vary during different stages of an athlete's training programme. Total haemoglobin mass (tHb-mass) is not affected by changes in plasma volume and is therefore a more stable measure of haemoglobin.53 Yet, little is known about the response of tHb-mass in IDNA endurance athletes because no randomised control trials have been carried out on this population. A recent study compared the effects of both oral and intravenous iron treatments and reported a likely effect on tHb-mass following intravenous iron injection (mean change of 4.9%) but not oral supplementation.20 However, an oscillation in tHb-mass of 6.9% over the course of a year has been reported in individual athletes,53 which suggests it may be difficult to associate very small changes in tHb-mass to intravenous iron treatment and therefore, care is warranted when using tHb-mass to assess the effectiveness of iron treatments. Future research should include a randomised placebo control approach to assess the sensitivity of tHb-mass to changes in iron status in clinical and athlete populations.
is reduced due to a fall in [Hb], causing a subsequent decrease in oxygen transport capacity.18 Conversely, IDNA is characterised by a reduction in ferritin without [Hb] falling below 12 g/dL,5 ,8–10 ,18 ,19 ,22 ,24 ,26–28 ,31 ,32 ,34 ,35 ,52 so the maintenance of [Hb] should mean that oxygen carrying capacity is not affected,4 ,5 and exercise performance maintained.8–10 ,21 Despite having initial [Hb] values within the normal range, our study indicates that iron treatment has a moderate effect on [Hb] (Hedges’ g=0.670, p<0.001; figure 4A). It is plausible that increases in [Hb] following iron treatment are related to the initial iron status and [Hb] of the athlete. For example, the studies included in this review that showed the largest effect sizes for [Hb] had initial sFer <10.80 µg/L25 ,30 and [Hb] <12.5 g/dL.27 ,28 ,32 This may indicate that the overall effect size for [Hb] was influenced by those studies whose populations had an initial [Hb] at the lowest end of the normal range for an endurance athlete. The influence of iron treatment on [Hb] in IDNA athletes should not be dismissed, as it has been suggested that although iron treatment may not elevate [Hb], it may serve to prevent an otherwise detrimental reduction, which would place the athlete at a greater risk of developing IDA.22 ,35 Furthermore, the suitability of [Hb] as an indicator of iron status should be questioned on the basis that it is influenced by haemodilution and plasma volume shifts, and therefore likely to vary during different stages of an athlete's training programme. Total haemoglobin mass (tHb-mass) is not affected by changes in plasma volume and is therefore a more stable measure of haemoglobin.53 Yet, little is known about the response of tHb-mass in IDNA endurance athletes because no randomised control trials have been carried out on this population. A recent study compared the effects of both oral and intravenous iron treatments and reported a likely effect on tHb-mass following intravenous iron injection (mean change of 4.9%) but not oral supplementation.20 However, an oscillation in tHb-mass of 6.9% over the course of a year has been reported in individual athletes,53 which suggests it may be difficult to associate very small changes in tHb-mass to intravenous iron treatment and therefore, care is warranted when using tHb-mass to assess the effectiveness of iron treatments. Future research should include a randomised placebo control approach to assess the sensitivity of tHb-mass to changes in iron status in clinical and athlete populations.
Independent of changes in [Hb], IDNA has been shown to negatively affect oxidative enzyme and respiratory protein activity in both animals6 and humans,7 implying that IDNA has the potential to impair aerobic capacity in endurance athletes. Indeed, improvements in maximal and sub-maximal  have been reported following iron treatment despite no changes in [Hb].23 The authors concluded that aerobic capacity was enhanced and attributed it to iron-mediated improvements in muscle oxidative capacity and improved mitochondrial function. Yet, measures of oxidative capacity at the muscle were not included in the study and therefore the conclusions are speculative.23 Likely improvements in
have been reported following iron treatment despite no changes in [Hb].23 The authors concluded that aerobic capacity was enhanced and attributed it to iron-mediated improvements in muscle oxidative capacity and improved mitochondrial function. Yet, measures of oxidative capacity at the muscle were not included in the study and therefore the conclusions are speculative.23 Likely improvements in  following intravenous treatment have been reported but these findings are limited by the lack of a control group.20 Results of the present study showed that iron treatment had a moderate effect on
following intravenous treatment have been reported but these findings are limited by the lack of a control group.20 Results of the present study showed that iron treatment had a moderate effect on  (Hedges’ g=0.585, p<0.001; figure 4B). There is variation among the included studies on the response of
(Hedges’ g=0.585, p<0.001; figure 4B). There is variation among the included studies on the response of  post-iron treatment (figure 4B) with no improvement in many studies.12 ,18 ,19 ,23 ,25 ,26 ,32 ,34 ,35 ,52 The moderate effect on
post-iron treatment (figure 4B) with no improvement in many studies.12 ,18 ,19 ,23 ,25 ,26 ,32 ,34 ,35 ,52 The moderate effect on  may be a result of the initial training status of the studied populations. The studies with the largest effect sizes had initial
may be a result of the initial training status of the studied populations. The studies with the largest effect sizes had initial  values <40 mL/kg/min24 ,27 ,28 compared to studies which showed no effect (>45 mL/kg/min), suggesting a greater potential for
values <40 mL/kg/min24 ,27 ,28 compared to studies which showed no effect (>45 mL/kg/min), suggesting a greater potential for  enhancement, particularly if the iron supplementation was combined with aerobic training. A recent meta-analysis investigating the effects of oral iron supplementation in women of reproductive age also reported significant effects on relative and absolute
enhancement, particularly if the iron supplementation was combined with aerobic training. A recent meta-analysis investigating the effects of oral iron supplementation in women of reproductive age also reported significant effects on relative and absolute  (increase of 2.35 mL/kg/min; 95% CI 0.82, 3.88 and 0.11 L/min; 95% CI 0.03 to 0.20, respectively).54 Despite not being specific to iron deficiency or endurance athletes, this does support the suggestion that iron supplementation can enhance aerobic capacity. It should be noted that
(increase of 2.35 mL/kg/min; 95% CI 0.82, 3.88 and 0.11 L/min; 95% CI 0.03 to 0.20, respectively).54 Despite not being specific to iron deficiency or endurance athletes, this does support the suggestion that iron supplementation can enhance aerobic capacity. It should be noted that  is only one indicator of aerobic capacity and where an improvement in
is only one indicator of aerobic capacity and where an improvement in  has not been observed, improvement in another measure such as energetic efficiency52 and tHb-mass3 has been demonstrated. The findings of the present review support the efficacy of iron treatments to improve iron status and
has not been observed, improvement in another measure such as energetic efficiency52 and tHb-mass3 has been demonstrated. The findings of the present review support the efficacy of iron treatments to improve iron status and  in IDNA endurance athletes but it is a limitation of this meta-analysis that the mechanisms underpinning the response are not fully addressed due to the descriptive nature of the studies. The aim of future research should be to clarify the underlying causes of IDNA in order to better understand iron metabolism in this population.
in IDNA endurance athletes but it is a limitation of this meta-analysis that the mechanisms underpinning the response are not fully addressed due to the descriptive nature of the studies. The aim of future research should be to clarify the underlying causes of IDNA in order to better understand iron metabolism in this population.
Iron administration and methodological considerations
The variations between studies in the response of iron status and  to iron treatment are likely due to methodological differences. There are currently no evidence-based treatment guidelines to inform the treatment of IDNA athletes. The Ganzoni formula is used clinically to calculate the iron requirements of patients, whom often require 1000–2000 mg of iron to adequately replenish body iron stores.55 Moreover, a single dose of 1000 mg is safe for individuals with [Hb] >10 g/dL.36 Although the iron requirements of individuals undergoing clinical diagnoses are likely to be greater than athletes, these dosages far exceed those reported in the studies included in this meta-analysis where oral iron is prescribed in a broad range of 10–425 mg, 1–3 times per day for 6–15 weeks22–29 ,31 ,32 ,34 ,35 ,52 and although research utilising parenteral treatments is sparse, dosages range from 500–550 mg, divided between 3–4 intramuscular injections, spread over 8–42 days.18 ,19 This wide variety of treatment protocols and the heterogeneity in responses highlights the need for a better understanding of the relationship between dose and response. The meta-regression carried out in this study indicates a significant interaction between the effect of iron treatment on sFer and dose duration (figure 2B). Thus, the effect of iron treatment on sFer appears to diminish the longer the treatment period continues, particularly if treatment lasts beyond 80 days. It could be implied from this that higher doses over a shorter period of time would be more effective than smaller doses over longer periods but no significant interaction was found between total iron dose and the effect on sFer or
to iron treatment are likely due to methodological differences. There are currently no evidence-based treatment guidelines to inform the treatment of IDNA athletes. The Ganzoni formula is used clinically to calculate the iron requirements of patients, whom often require 1000–2000 mg of iron to adequately replenish body iron stores.55 Moreover, a single dose of 1000 mg is safe for individuals with [Hb] >10 g/dL.36 Although the iron requirements of individuals undergoing clinical diagnoses are likely to be greater than athletes, these dosages far exceed those reported in the studies included in this meta-analysis where oral iron is prescribed in a broad range of 10–425 mg, 1–3 times per day for 6–15 weeks22–29 ,31 ,32 ,34 ,35 ,52 and although research utilising parenteral treatments is sparse, dosages range from 500–550 mg, divided between 3–4 intramuscular injections, spread over 8–42 days.18 ,19 This wide variety of treatment protocols and the heterogeneity in responses highlights the need for a better understanding of the relationship between dose and response. The meta-regression carried out in this study indicates a significant interaction between the effect of iron treatment on sFer and dose duration (figure 2B). Thus, the effect of iron treatment on sFer appears to diminish the longer the treatment period continues, particularly if treatment lasts beyond 80 days. It could be implied from this that higher doses over a shorter period of time would be more effective than smaller doses over longer periods but no significant interaction was found between total iron dose and the effect on sFer or  from the studies included here.
from the studies included here.
Treatment method is also a consideration when attempting to determine the most suitable treatment for IDNA athletes. Evidence from clinical investigations in patients suggests that oral iron is poorly absorbed due, in part, to inflammation and the resulting upregulation of hepcidin, thus, taking 3–6 months to fully restore total body iron stores.12 ,18 Conversely, parenteral iron treatments, which are commonly used in clinical settings in the form of non-dextran iron formulations, can be administered in a single, higher dose with minimal potential for adverse affects such as anaphylactic reactions.56 ,57 Increases in [Hb] within 2 weeks of the treatment have been reported using these methods.16 Of note, in the present study the sub group meta-analysis of treatment method indicated that oral treatments had larger effects sizes for [Hb] and  than iron treatment carried out via intramuscular injection in IDNA athletes. This finding is likely the result of the small number of studies using intramuscular injection treatments. Additionally, it should be noted that the injection studies included in this meta-analysis used intramuscular injections, whereas the use of intravenous injections may yield different results due to the increase of bioavailable iron afforded with this method.58 Although an attempt has been made to determine the difference in the effectiveness of intravenous injection and oral iron treatments,20 it is evident that more research is required in order to establish an optimal dose, method and protocol for the treatment of IDNA in endurance athlete populations. In particular, the small number of intramuscular injection studies that met the inclusion criteria in the current meta-analysis and the absence of intravenous iron treatment studies highlights the need for further randomised, placebo controlled trials to assess the efficacy of parenteral iron treatments for IDNA endurance athletes.
than iron treatment carried out via intramuscular injection in IDNA athletes. This finding is likely the result of the small number of studies using intramuscular injection treatments. Additionally, it should be noted that the injection studies included in this meta-analysis used intramuscular injections, whereas the use of intravenous injections may yield different results due to the increase of bioavailable iron afforded with this method.58 Although an attempt has been made to determine the difference in the effectiveness of intravenous injection and oral iron treatments,20 it is evident that more research is required in order to establish an optimal dose, method and protocol for the treatment of IDNA in endurance athlete populations. In particular, the small number of intramuscular injection studies that met the inclusion criteria in the current meta-analysis and the absence of intravenous iron treatment studies highlights the need for further randomised, placebo controlled trials to assess the efficacy of parenteral iron treatments for IDNA endurance athletes.
An additional factor to consider when examining the effectiveness of iron treatments for IDNA endurance athletes is the potential for sex variation in the response. Hormones that are involved in the regulation of the menstrual cycle such as oestrogen and progesterone are reported to influence post exercise iron metabolism via hepcidin.59 sFer and sFe have been found to be higher in women who are taking the oral contraceptive pill (OCP) than those who were not60 ,61 and 6 months of OCP use has significantly increased sFer.62 The mechanism for improved iron status following OCP use is thought to be reduced menstrual blood loss63 or an oestradiol-mediated suppression of hepcidin, allowing for greater iron absorption.64 Thus, there is a possibility that women may respond to iron treatment differently to men. The subgroup meta-analysis for sex carried out in this review (table 2) revealed larger effect sizes (Hedges’ g >0.700) for females compared to males for all iron parameters, [Hb] and  . It should be noted that iron treatment was still effective at improving sFer (Hedges’ g=0.614), sFe (Hedges’ g=1.049), [Hb] (Hedges’ g=0.521) and Tsat (Hedges’ g=0.561) in male IDNA athletes.
. It should be noted that iron treatment was still effective at improving sFer (Hedges’ g=0.614), sFe (Hedges’ g=1.049), [Hb] (Hedges’ g=0.521) and Tsat (Hedges’ g=0.561) in male IDNA athletes.
The iron indices focused on in this meta-analysis are the most common measures used to determine an athlete's iron status. However, additional red cell indices and reticulocyte parameters are important in the differentiation of various anaemic conditions such as thalassaemia trait, which is relatively common in athletes.64 Therefore, measures such as mean cell volume and reticulocyte counts should be used in conjunction with the more traditional iron indices when interpreting the effectiveness of iron treatments.
Conclusions
Research has produced inconsistent findings on the effects of iron treatments for IDNA athletes. Despite the lack of evidence-based guidelines, iron treatment is a frequently used intervention for athletes diagnosed with iron deficiency. This meta-analysis confirms that iron treatments improve iron status and, furthermore, that iron treatments are effective for improving the  of IDNA endurance athletes. Both oral and intramuscular injection treatments are effective for improving
of IDNA endurance athletes. Both oral and intramuscular injection treatments are effective for improving  . The very small number of studies that have investigated injection treatments and the successful employment of intravenous iron injections in clinical settings implies that further research to elucidate the effects of iron injections on IDNA in athlete populations is warranted.
. The very small number of studies that have investigated injection treatments and the successful employment of intravenous iron injections in clinical settings implies that further research to elucidate the effects of iron injections on IDNA in athlete populations is warranted.
Regression analysis in the present study revealed a significant interaction between the effect of iron treatment on sFe and treatment duration, suggesting that the effect diminishes if treatment lasts longer than 80 days. An optimal dose protocol that ensures the most effective and time efficient treatment is of particular importance to endurance athletes. Further studies are needed to improve the understanding of the relationship between iron dose and response. As the studies included in this review are descriptive they do not shed light on the iron metabolism mechanisms of IDNA endurance athletes. Future research should determine if there are any long-term consequences of having IDNA. Similarly, the consequences of long-term iron treatment in this population need to be established
Summary of findings
Iron treatment via both oral supplementation and parenteral injection are effective at improving the iron status of iron-deficient but non-anaemic endurance athletes.
The effect of iron treatment on serum ferritin appears to diminish if the treatment period continues beyond 80 days.
The improved iron status following treatment may enhance aerobic capacity (
).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
Footnotes
Contributors RJB participated in protocol design, data extraction, data analyses and manuscript preparation. CP participated in protocol design, data analyses and manuscript preparation. KM participated in protocol design and manuscript preparation. TR and GW participated in manuscript preparation. All authors have read and approved the final manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.