Article Text

Abstract
Valvular heart diseases in Africa affect mainly children and young adults and are a result of rheumatic fever. Rheumatic fever is a preventable disease, but in Africa the combination of a lack of resources, lack of infrastructure, political, social and economic instability, poverty, overcrowding, malnutrition and lack of political will contributes to the persistence of a high burden of rheumatic fever, rheumatic valvular heart diseases and infective endocarditis. Combating and eradicating rheumatic fever and rheumatic heart diseases requires economic development and implementation of best practices of primary and secondary prevention measures. The barriers to achieving this goal in Africa are numerous, but not insurmountable.
Statistics from Altmetric.com
Valvular heart diseases (VHD) from rheumatic fever (RF) affecting children and young adults are the predominant form of VHD on the African continent.1 2 The World Health Organisation expert panel on RF and rheumatic heart disease (RHD) reviewed the global burden of these disorders and estimated that about 12 million people world wide in 1994 had RF and RHD, most of them in developing countries.1 A more recent review3 4 of the current evidence for the global burden of RF and RHD estimates that 15.6–19.6 million people have RHD (2.4 million children aged 5–14 years) causing 233 364–294 398 deaths from RHD each year (based on annual mortality of 1.5% per year). The number of people with previous RF without subsequent carditis, but who need continuing secondary antibiotic prophylaxis is estimated to be 1.88 million. The highest prevalence of RHD is in sub-Saharan Africa with a prevalence of 5.7 per 1000, compared with 1.8 per 1000 in North Africa, and 0.3 per 1000 in economically developed countries with established market economies.3 4 In this review, the aetiology of RF and rheumatic and non-rheumatic valvular diseases and their complications and overall disease burden on the African continent, as well as current strategies and efforts to ameliorate and eradicate these disorders are discussed.
AETIOLOGY OF RHEUMATIC FEVER
The aetiology and pathogenesis of RF and RHD are incompletely understood.5 6 The current working paradigm on which diagnosis, treatment, primary and secondary prevention measures and vaccine development are based is that RF, a multiorgan disease which can affect the heart, joints, skin and brain, results from a delayed immune response to Lancefield group A β-haemolytic streptococcus (GABHS) pharyngitis after a latent period of 1–5 weeks (average 19 days).7 8 The link between acute RF and GABHS pharyngitis has been established firmly by observational and experimental data in Western countries.7 9–13 Three per cent of GABHS pharyngitis leads to RF if left untreated,14 but the risk of RF increases from 3% to 75% after subsequent or recurrent GABHS pharyngitis.15–17 GABHS pharyngitis represents 20% of all pharyngitis with symptoms of fever and sore throat and affects principally children and young adults, most commonly in the age group 5–15 years.18 However, 30–50% of all children who later develop RF do not recall a preceding pharyngitis.19 Rarely, adults may also have acute RF where contact with young children appears to be a predisposing factor.20 The presence of GABHS in the throat may also reflect a carrier state and without a true infection, carriers are not at risk of RF.21
Complicating the current paradigm that RF is a consequence only of GABHS pharyngitis are data from Australian aborigines who have among the world’s highest incidence of RF and prevalence of RHD.22 The suggested link of RF in that population is to non-GABHS infections and GABHS skin infections (pyoderma), from dynamic, diverse and unique strains, and GABHS throat colonisation is uncommon and GABHS pharyngitis rare.22 This would have immediate consequences for the epidemiology and prevention of RF and RHD in parts of the world that continue to be afflicted with a high burden of these diseases.22
Pharyngeal carriage of GABHS in a 1980 study in Coloured and Indian schoolchildren in South Africa was 24.4% and 21.3%, respectively, in the summer, and 4.3% and 3.4% in the spring.23 A recent survey in Benin City, Nigeria in 2001 found a streptococcus throat carriage prevalence of 9.7%, which comprised group C (38%), G (36%), F (20%) and B (7%), but no GABHS.24 However, there are no studies in Africa linking non-GABHS to RF and RHD.
DIAGNOSTIC CRITERIA
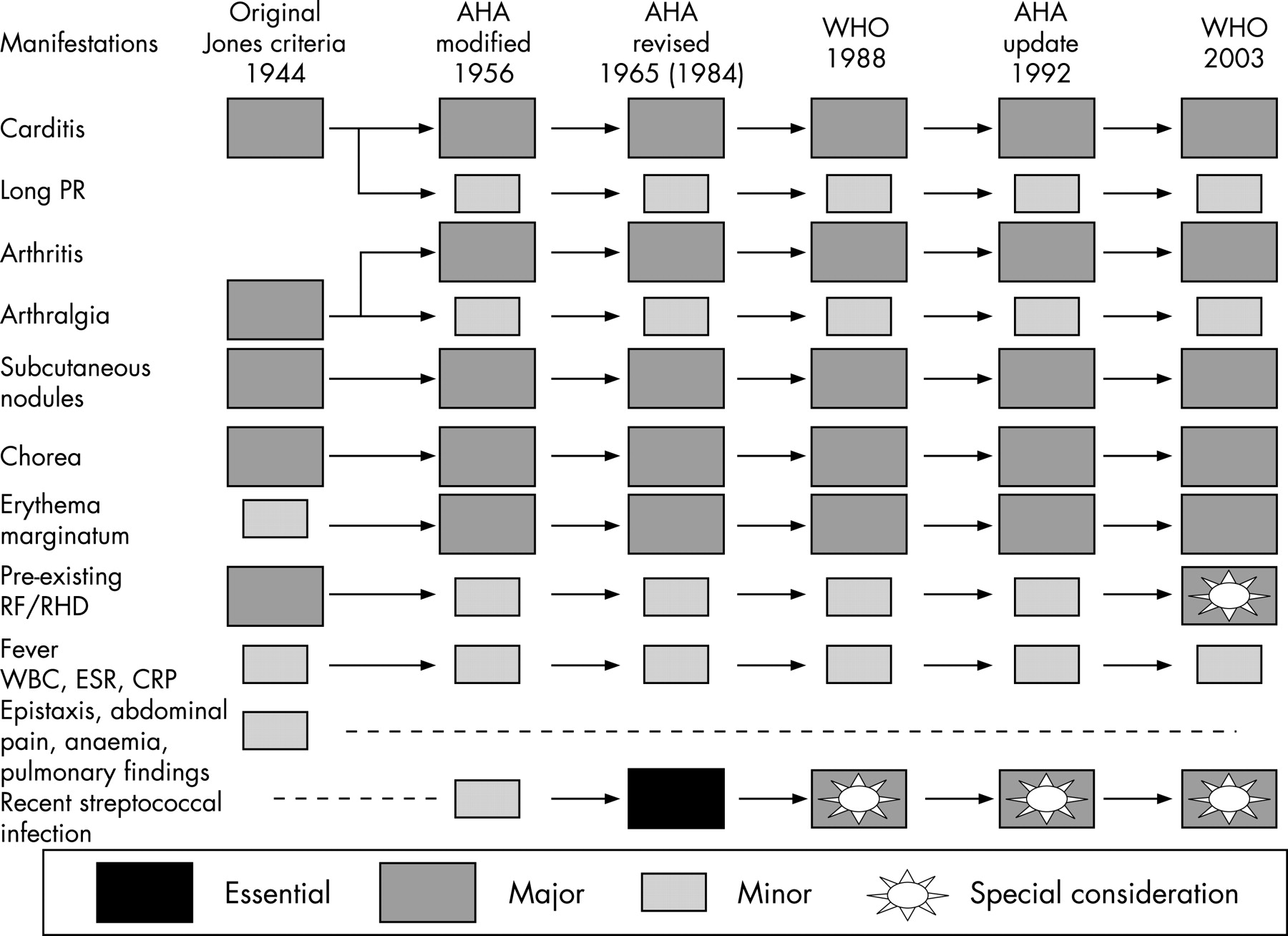
The manifestations of RF are protean and depend on the severity of the attack, the site of involvement, and time of presentation of the patient, making the clinical diagnosis difficult and challenging.13 A diagnostic guide13 based on clinical manifestations of RF was first published by Dr T Duckett Jones in the USA in 1944 to help overcome the challenges in diagnosing RF. These diagnostic criteria have since undergone modification25 and revisions26–28 in an attempt to improve their specificity in establishing the initial attack of acute RF to avoid overdiagnosis, emphasising the importance of demonstrating evidence of antecedent GABHS pharyngitis, except for late manifestations of RF. However, increasing the specificity of the criteria to avoid overdiagnosis is more suitable for developed countries where the incidence of RF is now low, and developing countries need more sensitive criteria given the high burden of disease and the dire consequences of missed disease.1 The 2002–3 World Health Organisation criteria for the diagnosis of RF and RHD based on the revised Jones criteria (fig 1) take this into account and it is recommended that they should be used in areas with populations at high risk.1 6

RHEUMATIC CARDITIS
Carditis, valvulitis in particular, is the single most important cause of morbidity and mortality in RF.29 There is evidence of cardiac involvement during the acute episode in 40–80% of cases of acute RF,30–33 but cardiac involvement almost always occurs in recurrent episodes.34 Valvular heart involvement in the attack of RF may range from mild to severe and is suspected on the basis of a murmur on physical examination or unexplained cardiomegaly or heart failure,13 but non-invasive imaging with echocardiography increases the sensitivity of diagnosing VHD since it is better than physical examination and should be used where available.1 About 90% of children who have carditis during RF episodes will develop chronic and progressive RHD from inflammation and scarring of the heart valves, which may result in haemodynamically significant valvular regurgitation and or stenosis, heart failure, and death.28 35 36
DISEASE BURDEN IN AFRICA
The estimated prevalence of RHD in sub-Saharan Africa is 5.7 per 1000 and in North Africa 1.8 per 1000 derived from all relevant population-based data from the 1980s and 1990s (table 1).4 Factoring in other large population-based surveys from the 1970s with a total of 44 818 screened school-age children from the Ivory Coast, Nigeria, and South Africa, the estimated prevalence of RHD in sub-Saharan Africa remains high at 5.1 per 1000. Determinants of the persistence of RF and RHD in Africa are poverty, overcrowding, malnutrition, low level of disease awareness in the communities, shortage of resources for providing quality care and inadequate expertise of healthcare providers,1 potentially unidentifiable or more virulent group A streptococci,37 and possible yet unexplained underlying genetic susceptibility.38 39 The decline in RF and RF mortality has been extraordinary in economically developed nations and began before the introduction of antistreptococcal agents,40 41 and was due in part to improved socioeconomics and potentially changes in the virulence of infecting GABHS.37 42 The socioeconomic, environmental and health system related shortcomings in Africa have the direct effects of increasing transmission and spread of streptococcus infections, lead to missed or inadequate diagnosis and treatment of streptococcal pharyngitis, and poor adherence to secondary prevention measures, with a sum effect of a higher incidence of acute and recurrent RF and higher incidence and prevalence of RHD.1
Data on the incidence of RF in Africa are sparse.4 The incidence of acute RF in Algeria in 1997 was 11.1 per 100 000 per year and in 2000, 6.2 per 100 000 per year.3 In Tunisia in 1990, the incidence was 30 per 100 000 per year.43 There are no studies documenting the incidence of acute RF in sub-Saharan Africa. An estimation of 13 per 100 000 per year for sub-Saharan Africa is based on incidence rates from North Africa and the Middle East.4
Capturing new cases of RF requires active surveillance programmes and these do not exist in many parts of Africa. The World Health Organisation designed a project in 1972 for the community control of RF and RHD in six centres in developing countries, which included two African countries, Egypt (Cairo) and Nigeria (Lagos). The aim was to establish RF registries each covering a limited community, register all patients with RF, screen high-risk populations (if appropriate) for rheumatic disease, encourage cooperation between hospitals, politicians, school health services, laboratories and individual doctors in the promotion of RF prevention and control, and provide health education for the general public.44 The project showed that setting up protocols for capturing cases of RF and RHD in developing countries was feasible, but that operations of such programmes were difficult, with only partial regular surveillance of identified cases.44
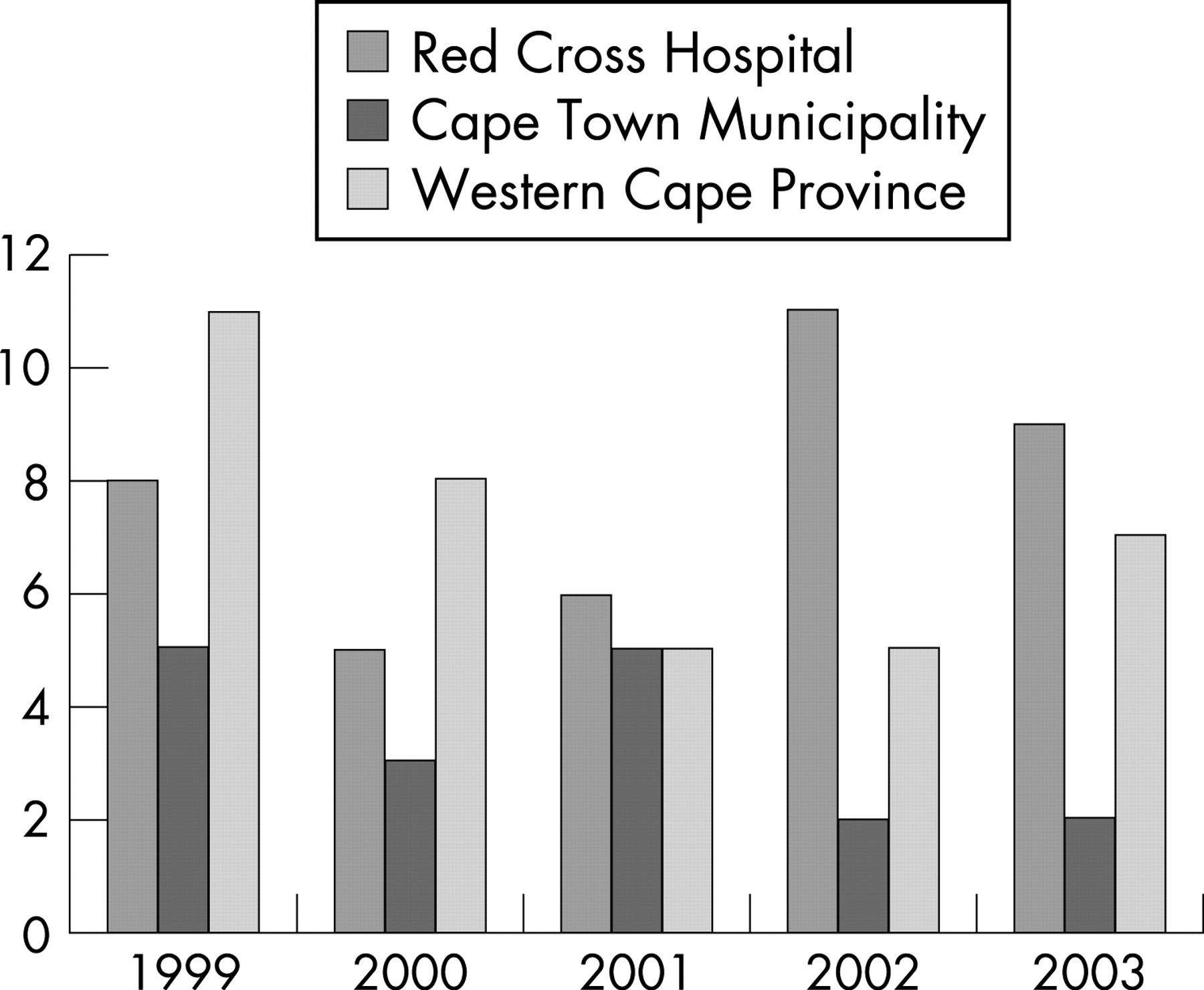
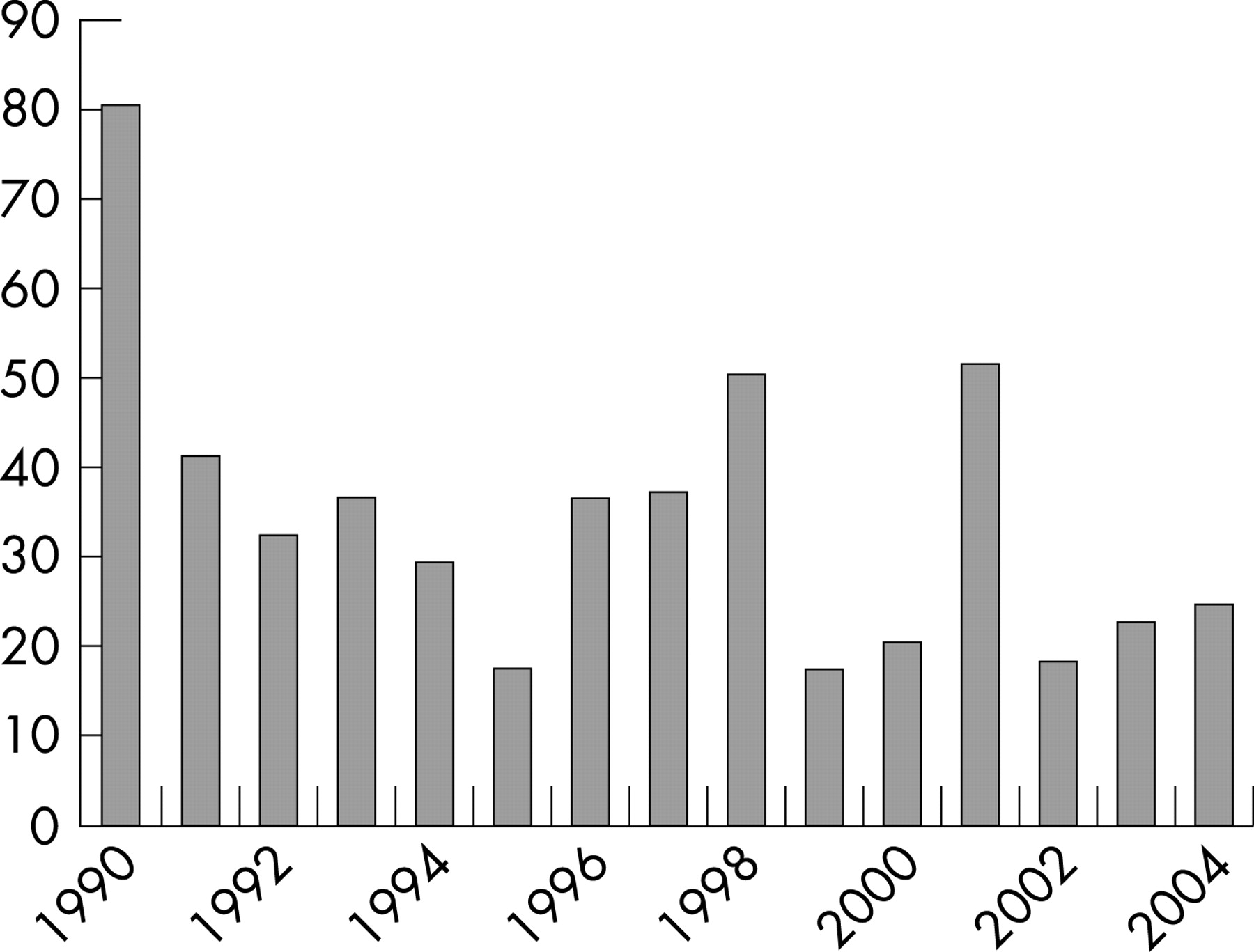
Even in the more industrialised countries in Africa, such as South Africa, active surveillance of RF remains a challenge. A comprehensive audit of the number of RF cases notified each year in South Africa since official notification of RF began in 1990 was published recently.45 Key findings were a fall in the number of RF cases over a 15-year period, but also poor and underreporting of cases by health administrators at all levels of the health system (in the Western Cape), suggesting that the observed decline in the number of cases may be related to significant undercounting (figs 2 and 3).45 Case reporting from the Western Cape to the National Department of Health is also consistently disproportionately higher than in other provinces in South Africa that are more densely populated, poorer, have a higher burden of cases of RHD and therefore are expected to have a higher incidence of RF.42 46

Consistent with observations elsewhere in the world, a few studies in Africa have shown that the distribution of RF and RHD is shifted towards the poor, and is more common in rural than urban areas, except in slum conditions.4 In a survey of RHD in school children of Kinshasa town in the Democratic Republic of Congo, of the 4848 school children aged 5–16 years screened, the prevalence of RHD was 14.03 per 1000, but the prevalence was significantly higher in slum schools (22.2 per 1000) than in urban schools (4 per 1000).47 Other risk factors that predicted RHD were low birth weight, low socioeconomic status and household overcrowding.47 The prevalence of RHD confirmed by echocardiography in school children attending grades 7 and 8 in Addis Ababa, Ethiopia, was 6.4 per 1000, but was distributed unevenly between those in lower socioeconomic groups (7.1 per 1000) and high socioeconomic groups (1 per 1000).48 In South Africa, RHD affects principally black children and young adults as a consequence of the deleterious socioeconomic policies under apartheid.46 49–52
CLINICAL COURSE
A systematic review of the hospital-based and cause of death studies in Africa relating to RHD highlights RHD as the main cause of cardiac morbidity and mortality in children and young adults.3 The clinical course of acute rheumatic carditis in Africa runs a fulminant course and seems more malignant.50 53–55
Ransome and Roode described 46 children with acute RF admitted to Coronation Hospital, Johannesburg, South Africa between April 1981 and December 1984.55 The young age of the patients is highlighted and ranged from 4.5 to 12.4 years. Carditis was present in 26 cases (57%), but 35 cases (76%) developed RHD (all had mitral regurgitation). Mortality was 6.5% (three patients died) and three patients underwent emergency valve replacement for intractable cardiac failure.55
A prospective study of 80 children in Nigeria with a mean age of 8.8 years (34 had acute RF and 18 had recurrent RF) showed a high cumulative mortality of 20% at 6 years attributable to heart failure and infective endocarditis.56
A retrospective study (January 1993 to December 1996) carried out by Kimbally-Kaky and colleagues described the epidemiology, diagnosis, evolution and treatment of RF during childhood in the Teaching Hospital of Brazzaville, Congo. The study included 56 patients (36 girls and 20 boys) with a mean age of 10 years 8 months. There was a past history of a sore throat in 27 cases (48.2%) and 11 cases (19.6%) had recurrent RF. Carditis was present in 49 patients (87.5%) and mitral regurgitation was the most common cardiac lesion. Heart failure was diagnosed in 25 patients (44.6%). Twenty-two patients underwent surgery, which included, in decreasing frequency, mitral valve bioprosthesis, valvuloplasty, aortic valve prosthesis and tricuspid valve commissurotomy. Mortality was high at 10.7% (six patients died) and the leading cause of death was heart failure, followed by infective endocarditis, and probable mechanical aortic valve thrombosis.54
In a retrospective study of deaths between 1995 and 2001 at the Tikur Anbassa Teaching Hospital, Addis Ababa, Ethiopia, Oli and Asmera reported that 26.5% of the cardiovascular deaths were due to RHD and 70% of patients with RHD died from congestive heart failure at a mean age of 25 years (11% died from systemic embolisation and comorbid conditions). The majority had combined mitral and aortic valve regurgitation, and isolated mitral regurgitation or stenosis was relatively uncommon.53
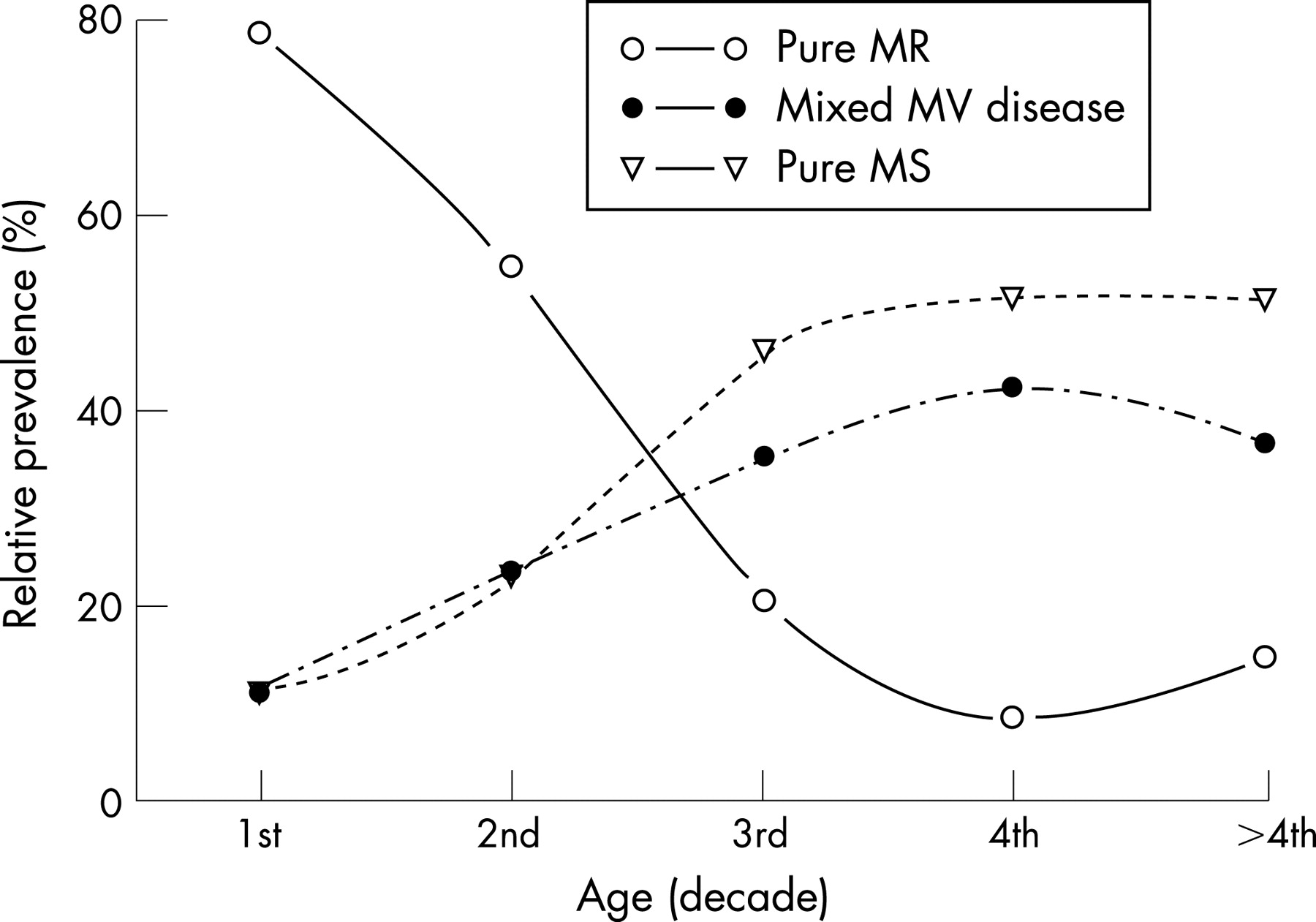
Heart failure is the predominant mode of death in rheumatic carditis and the persistence of the epidemic of RF in Africa has led to important observations that explain the high early mortality rate among young patients with acute rheumatic carditis.50 57 It has been determined that left ventricular dilatation and heart failure rarely occur in the absence of mitral regurgitation with or without aortic regurgitation, and that only surgical correction of valvular regurgitation leads to left ventricular reverse remodelling and improvement in heart failure, arguing against a myocardial factor or myocarditis as the cause of heart failure in rheumatic carditis and against a major role for steroids in management.58 Also, the pathophysiological mechanism of mitral regurgitation during active carditis has been determined to be related to annular dilatation, chordal elongation and anterior mitral leaflet prolapse.50 59 Pure mitral valve regurgitation without stenosis causing heart failure is common in the young who have severe active rheumatic carditis, and the relative prevalence of mitral stenosis from chronic rheumatic valvulitis increases with age (figs 4 and 5).50

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rheumatic valvular diseases complicate pregnancies in young women in Africa.60–66 Rheumatic mitral valve disease accounted for 89.5% of cardiac diseases associated with pregnancy (mean (SD) age of patients 25 (5.5) years) during an admission period of 12 months (October 2003 to October 2004) at the high-risk pregnancy unit at Mansoura University Teaching Hospital, Mansoura, Egypt, with a maternal mortality of 1.16% (one patient died out of 86 patients included in the study).65 el Kady and colleagues reported that rheumatic valve disease was responsible for 35% of the 385 maternal deaths that occurred between 1981 and 1983 in the Menoufia Governorate, Egypt.64 In South Africa, rheumatic valvular disease complicates 0.6% of pregnancies of black women from low socioeconomic background, with a maternal mortality rate of 9.5%.67
When maternal deaths that occurred in South Africa in 1998 (565 cases) were reported to the “South African National Committee on Confidential Enquiries into Maternal Deaths” (NCCEMD), allowing for a population-based assessment of maternal deaths (although there is potential under-reporting and the actual number of deliveries is unknown), it was found that over half of the 10.4% deaths due to pre-existing medical conditions were due to pre-existing cardiac disease—namely, rheumatic valvular disease.68 Preventable factors identified to have contributed to these maternal deaths were not only patient-attributed such as lack of antenatal care and delay in seeking attention, but also healthcare system-attributed such as accurate assessment of severity of conditions, failure to act on the severity of the condition, uncontrolled fluid infusion and failure to recognise risk during the postpartum period.66 The fetus is also at risk and antenatal management concerns are complex and include risks to both mother and fetus with regard to optimal medical treatment, anticoagulation treatment69 and timing of valve surgery or mitral balloon valvotomy.
Mitral stenosis is a particularly common rheumatic valve lesion in pregnant women and it is not uncommon for diagnosis of valve disease to be made for the first time late in pregnancy.70 Mitral balloon valvotomy is a favoured procedure to treat mitral stenosis. The African experience with this technique has been reported from several centres and emphasises the feasibility of the technique during pregnancy and also the potential risks and complications such as maternal death (<1%), systemic embolisation (0–2%), cardiac tamponade (0–0.7%) or the development of severe mitral regurgitation (0–8%).71–75 The report on the North African experience in Tunisia describes long-term outcomes of mitral balloon valvotomy, where 463 consecutive patients with mitral stenosis (11.7% of them were pregnant at the time of the procedure) underwent balloon valvotomy and were followed up for up to 6.8 years with only eight patients lost to follow-up.73 Compared with baseline, functional class was markedly improved at the 6-month follow-up (class III–IV 69% baseline vs 4% at follow-up) and 77% were in class I. Mitral restenosis, defined as mitral valve area <1.5 cm2 by echo-planimetry, occurred in 45 patients or 10.4%. Freedom from restenosis was 98% at 1 year and 92% at 3 years; an echocardiographic score >876 and calcification by fluoroscopy were major determinants of restenosis.73 These results are comparable to other long-term reports from other parts of the world.
RHEUMATIC VALVE DISEASE AND INFECTIVE ENDOCARDITIS
Infective endocarditis in Africa remains a disease of the young and RHD is the main predisposing factor.1 77 However, only a few large epidemiological studies have been performed in Africa to document the relationship of rheumatic valvular disease and infective endocarditis.3
A retrospective study based on 157 cases of infective endocarditis observed in the Cardiology Department of Ibn Rochd Hospital, Casablanca, Morocco, covering January 1983 to December 1994, was reported by Bennis and colleagues.78 The mean age of the patients was 27.5 years (range 11–65) with a male predominance (62.8%). Infective endocarditis was secondary to rheumatic valvular disease in 63% of patients and was primary in 29.9%. Mortality was 28.7%, mostly related to refractory heart failure.78
A retrospective study (January 1982 to December 1989) of infective endocarditis in 32 paediatric cases from Ahmadu Bello University Teaching Hospital, Zaria, Nigeria, found underlying heart disease in 30 patients (90%), where 21 cases (66%) had RHD and nine cases (28%) had underlying congenital heart diseases. Overall mortality was 47% due mostly to heart failure and neurological complications.79
A 3-year (1997–2000) prospective epidemiological study of infective endocarditis was carried out at the University of Stellenbosch and Tygerberg Academic Hospital, Cape Town, South Africa and reported by Koegelenberg et al in 2003.77 The study included 92 patients referred with probable infective endocarditis, but only patients with an audible murmur were included. The mean age was 37.7 years with a 1.6:1 male predominance. Duke criteria80 were used to diagnose endocarditis and transoesophageal echocardiography was used to complement transthoracic echocardiographic findings. Definite infective endocarditis was present in 47 patients, where RHD was the major predisposing underlying condition present in 36 (76.6%) and eight (17%) had previous prosthetic valve placement. Degenerative VHD or intravenous drug use or HIV infection were not important risk factors for infective endocarditis. New or worsening heart failure was diagnosed in 76.6% of the patients and, overall, 44.7% needed valve replacement.77 Six-month mortality was 35.6%. The proportion of “culture-negative” infective endocarditis was high at 55.3%, but this could be explained as due to exposure to antibiotics before blood culture sampling.77 81 Interestingly, the leading alternative diagnoses where the diagnosis of infective endocarditis was rejected were chronic RHD and acute RF.77
Although the microbiological features of infective endocarditis in Africa are similar to those of economically wealthier nations of the world (Bartonella quintana seems to be an important agent in “culture-negative” infective endocarditis82–84), other major aspects of the epidemiology of infective endocarditis in Africa are reminiscent of the experience of wealthier nations such as the USA and Western Europe before the antibiotic era77 85—namely, that infective endocarditis remains a disease of the young, predisposed by underlying rheumatic valve disease, with high morbidity and mortality.56 77–79 82 86–90 In addition, underlying congenital heart diseases remain an important risk factor for endocarditis,91 92 and risk of nosocomial infections has also been previously highlighted.93 The series of 12 cases of tricuspid valve endocarditis, 11 of them after “clandestine” abortions, collected over a period of 8 years reported from Brazzaville, Congo, draws attention to other causes of infective endocarditis.94
VALVE SURGERY
Problems related to valve repair or replacement for RHD with or without infective endocarditis in young economically disadvantaged patients are numerous. The fulminant course of RF, RHD and infective endocarditis coupled with delayed patient presentation results in a high incidence of heart failure at presentation,95 associated with high in-hospital and late mortality even with surgical intervention.96–98 An overall 3-year actuarial survival of 52% was reported by Louw and colleagues in South Africa in a group of 170 patients undergoing emergency heart valve surgery.97 Fradi et al in Tunis, Tunisia, observed a decline in mortality from infective endocarditis from 41.8% between 1981 and 1991 to 8.9% in the time period 1992–2004 at Rabta University Hospital,98 which is reassuring, but this is probably not a continent-wide trend.
Mitral valve annuloplasty in acute carditis is suboptimal99 and more complex repair is associated with an operative mortality of 2.6% and a late mortality of 15% when followed up for up to 132 months, with a reoperation rate of 27%.100 In general, mitral valve repair is preferable to prosthetic mitral valve replacement in patients with rheumatic carditis and long-term results are comparable in developing countries.101–104 Mitral valve repair for rheumatic carditis is much less common in developed countries,105 106 but is also associated with a hospital mortality of 2% and an actuarial survival of 82 (19)% at 10 years.106 The actuarial rate of reoperation is 2% patients per year where repair of the mitral valve at the acute phase of the inflammatory process is similarly associated with a higher reoperation rate.106
Bioprostheses are associated with rapid deterioration in young patients, and mechanical prostheses are complicated by potentially lethal thromboembolic events, haemorrhage and infective endocarditis.107 Antunes reported on 135 patients, mean (SD) age 13.7 (3.5) years, who had isolated mitral valve replacement with tissue prostheses for New York Heart Association class III and IV heart failure (22 had acute rheumatic valvulitis).107 Early mortality was 4.4% and late mortality was 10.7% per patient-year after a cumulative follow-up of 356 patient-years. Structural valve failure occurred in 80 patients during follow-up and actuarial survival at 7 years was only 50%, confirming the high failure rate of bioprosthesis in children and young adults.107 With respect to mechanical prostheses, freedom from valve-related mortality of 92 (2)% at 5 years, and corresponding freedom from systemic thromboembolism, thrombotic obstruction and prosthetic valve endocarditis of 85 (2)%, 95 (1)% and 97 (1)%, respectively, were reported by Antunes and colleagues in a study of 1000 mechanical Medtronic Hall valves in South Africa.108 Compliance with close follow-up of anticoagulation status is low and erratic, but fixed-dose warfarin treatment does not obviate the need for close monitoring109 and is associated with an increased risk of thromboembolic events.110–112
Many African communities are not equipped with the resources and medical or surgical expertise to manage valvular diseases. An illustrative case of this dilemma is described by Weidenbach et al in Mozambique where a previously healthy 14-year-old girl presented with a 3-week history of high-grade fever and dyspnoea and was diagnosed with severe heart failure.113 No laboratory investigations could be performed because of the lack of resources and therefore no organism was isolated. A portable hand-held echocardiogram showed destruction of the aortic valve with severe aortic regurgitation and extension of infection with two periaortal abscess cavities. The patient’s clinical condition deteriorated despite treatment with antibiotics but no surgery was performed because no cardiac surgery was available in Mozambique. After 2 weeks in the hospital, the parents took the girl home where she presumably died.113
How often this scenario is repeated in Africa is unknown. Some African countries have approached the mismatch between the need for valve surgery and resource availability by referring cases to Europe under the auspices of the Terre des Hommes Association or are visited by Chain of Hope missions, drawing attention to the role of humanitarian efforts.114 Others are trying to set up heart valve banks from cadavers,115 while there is an advocate for alternative cheaper surgical techniques and equipment.116 Overall, however, the role of valve surgery in combating the epidemic of VHD in Africa is limited and has been described as “attempting to mop up the water on the floor while leaving the faucet open”,117 and the situation is not improving owing, in part, to competing and or conflicting medical, socioeconomic and political needs.116 118 119
NON-RHEUMATIC VALVE DISEASE
The epidemiology of non-rheumatic valve diseases in Africa is also poorly defined. Myxomatous mitral valve disease associated with mitral valve prolapse was first described in South Africa by Barlow and Bosman in 1966,120 but is an uncommon cause for mitral valve surgery in African surgical series compared with rheumatic valve disease.99 100 107 108 112 118 121 Congenital subvalvular aneurysms below the mitral and aortic valves are rare forms of VHD and were also first described in Africa.122–127 Their aetiology is thought to be related to congenital weakness between the muscular ventricular wall and fibrous skeleton of valve annulus.124 Submitral aneurysms typically occur below the posterior leaflet, whereas subaortic aneurysms occur in association with the left aortic sinus.128 These congenital subvalvular aneurysms may be associated with varying degree of valve regurgitation, may rupture or compress the coronary arteries or may predispose to infective endocarditis or thrombus with systemic embolisation. Some submitral valve aneurysms may be related to tuberculosis.129 Valve diseases associated with aging or with endomyocardial fibrosis impose an additional burden of VHD in Africa, but constitute a much smaller portion of the reported cases needing valve surgery.130–133
PREVENTION OF VALVE DISEASE AND INFECTIVE ENDOCARDITIS
An estimated 42% of the 2.4 million children with RHD live in sub-Saharan Africa.4 It has been known for some time that prevention of the bulk of VHD and infective endocarditis in Africa can be achieved through the control of RF.1 44 Effective methods of controlling RF and RHD are known134—namely, prompt adequate treatment of suspected or confirmed GABHS pharyngitis with intramuscular or oral penicillin before the occurrence of RF (primary prevention),135 and long-term regular administration of penicillin to prevent recurrent RF (secondary prevention),136 since the majority of RHD are a result of recurrent RF.134 Duration of secondary prophylaxis is tailored to the presence and degree of VHD according to the World Health Organisation recommendations.137 Vaccines against RF will not be clinically available any time soon134 138 despite tremendous modern insights into the immunology of RF.
Diagnosis of GABHS pharyngitis requires laboratory confirmation where the “gold standard” remains a throat swab cultured on blood agar.1 Commercially available rapid diagnostic kits vary in sensitivity from 31% to 95%, and negative results require confirmation with laboratory culturing.1 139 140 Laboratories for bacterial culture and rapid diagnostic kits are not readily available in most developing countries or have not been adequately used where available,117 and clinicians have to rely on clinical guidelines for presumptive diagnosis and treatment of streptococcal pharyngitis. The World Health Organisation Acute Respiratory Infection Guideline141 attempts to maximise the diagnostic yield of clinical findings to help in the initial diagnosis of streptococcal pharyngitis, but the requirement of both pharyngeal exudate and tender, enlarged lymph nodes for the diagnosis of acute streptococcal pharyngitis was found to have a sensitivity of 12% and a specificity of 94% in a prospective study of the guidelines in Egypt.142–145 The low sensitivity of the guidelines, therefore, does not correctly identify a high number of children at risk of developing RF,142 suggesting a need for modification of the guidelines.
Primary and secondary prevention strategies have not been implemented fully in Africa and previous attempts by the World Health Organisation146 in limited number of African nations have not been sustained owing to the lack of funding.134 There is now renewed interest in RF and RHD given their persistence and enormous socioeconomic burden.3 The World Health Organisation proposed guidelines in 2004 for the control of RF and RHD1 and in response the Pan African Society of Cardiology (PASCAR) convened the first All Africa Workshop on RF and RHD on 15–16 October 2005, held in South Africa, for the purpose of formulating a road map and action plan for the prevention of RF and RHD in Africa.147 148 The adopted action plan was called the Awareness Surveillance Advocacy Prevention (ASAP) Programme, which is meant to be simple, yet comprehensive, to be adopted in part or whole by the continent’s national departments of health or non-governmental organisations.149 The ASAP Programme, while recognising the barriers to implementation, aims to apply best known practices of what works by (a) raising awareness150 151 about the disease among child caregivers, teachers, and healthcare workers; (b) establishing surveillance systems modelled after the “WHO STEPwise approach”152 used to collect epidemiological data on risk factors for non-communicable diseases in developing countries; (c) championing advocacy for RF and RHD, which have been neglected because of their virtual disappearance in wealthier countries; and (d) implementing primary and secondary prevention strategies that have been proved to be effective.
New guidelines for the prevention of endocarditis were published recently and contain substantive changes in recommendations for infective endocarditis prophylaxis.153 The guidelines limit types of procedures for which antibiotic prophylaxis is recommended and limit antibiotic prophylaxis to only certain cardiac conditions not including RHD (table 2).153 The reasons for the changes (table 3) are discussed at length in the guidelines.153 Studies on the prevention of endocarditis in patients with RHD in Africa are needed since RHD would qualify as cardiac conditions associated with the highest risk of adverse outcome from endocarditis.
CONCLUSION
Unlike economically wealthier nations where RHD are rare and valve diseases are mainly related to aging,154 RHD predominate in Africa and their true prevalence may potentially be higher than currently estimated. Challenges to controlling the epidemic of valve diseases in Africa are many, but not insurmountable, since proven cost-effective means of controlling the problem exist. Governments in developing and industrialised countries, funding agencies and other international bodies have recently been invited by the World Heart Federation Scientific Council on RF and RHD to participate in a global strategy for the control of this epidemic.134
Addendum
After acceptance of this paper for publication, Marijon and colleagues164 published a study showing very high prevalence of RHD of 30.4 per 1000 detected by echocardiographic screening of 2170 school children aged 6 to 17 years in Maputo, Mozambique, sub-Saharan Africa. This is in stark contrast to the estimated prevalence of 5.1 or 5.7 per 1000 and underscores the high burden of RHD in Africa, the need in Africa for more precise epidemiological data, and the important role of echocardiography in the detection of RHD.
REFERENCES
Footnotes
Conflict of interest: None.
- Abbreviations:
- GABHS
- group A β-haemolytic streptococcus
- RF
- rheumatic fever
- RHD
- rheumatic heart disease
- VHD
- valvular heart disease