Article Text

Abstract
CT-derived fractional flow reserve (CT-FFR) uses computational fluid dynamics to derive non-invasive FFR to determine the haemodynamic significance of coronary artery lesions. Studies have demonstrated good diagnostic accuracy of CT-FFR and reassuring short-term clinical outcome data.
As a prerequisite, high-quality CT coronary angiography (CTCA) images are required with good heart rate control and pre-treatment with glyceryl trinitrate, which would otherwise render CTCA as unsuitable for CT-FFR. CT-FFR can determine the functional significance of CAD lesions, and there are supportive data for its use in clinical decision-making. However, the downstream impact on myocardial ischaemic burden or viability cannot be obtained.
Several challenges remain with implementation of CT-FFR, including interpretation, training, availability, resource utilisation and funding. Further research is required to determine which cases should be considered for clinical CT-FFR analysis, with additional practical guidance on how to implement this emerging technique in clinical practice. Furthermore, long-term prognostic data are required before widespread clinical implementation of CT-FFR can be recommended.
While there are several potential opportunities for CT-FFR, at present there remain important systemic and technical limitations and challenges that need to be overcome prior to routine integration of CT-FFR into clinical practice.
- cardiac computer tomographic (CT) imaging
- advanced cardiac imaging
- coronary artery disease
- chronic coronary disease
Statistics from Altmetric.com
- cardiac computer tomographic (CT) imaging
- advanced cardiac imaging
- coronary artery disease
- chronic coronary disease
Background
Invasive coronary angiography (ICA) with fractional flow reserve (FFR) is the reference standard for detection of significant, flow-limiting, coronary artery disease (CAD) and is recommended in guidelines for coronary intervention in patients with chronic coronary syndromes.1 In clinical practice, invasive FFR is calculated by measurement of intraluminal pressure (proportional to flow) distal to a stenosis under maximal hyperaemia during adenosine administration. Large clinical studies have demonstrated that invasive FFR improves outcomes in patients with CAD considered for revascularisation.2 3
Computational flow dynamic (CFD) modelling is a mathematical field in which fluid mechanics are used to simulate fluid flow, based on solving complex formulae including the Navier-Stokes equation.4 Using CFD, CT-derived FFR (CT-FFR) can be obtained from CT coronary angiography (CTCA) data. CFD has been routinely applied to many fields of engineering such as the aeronautic and automotive industries dating back to the 1960s.
Several steps are required to derive CT-FFR. First, an anatomical construction of the aortic root, whole myocardium and coronary arteries is required for the determination of inflow and outflow modelling parameters. Second, coronary physiology modelling requires artefact-free coronary arteries to determine boundary conditions. With additional calculation of the cardiac output, aortic pressure and microcirculatory resistance, fluid dynamic modelling can be used to derive pressure and flow in the coronary arteries.5 Undertaking these analyses using three-dimensional (3D) models requires significant computational power with a computer or graphics processing unit.
CT-FFR has the potential to complement anatomical CTCA findings with physiological data regarding the haemodynamic significance of CAD. In contrast to invasive FFR, CT-FFR does not require intravenous adenosine administration, although it requires glyceryl trinitrate (GTN) for coronary vasodilatation. Once calculations are complete, a 3D map of FFR values of the entire coronary tree down to the distal vessel is generated. A typical example of a focal stenosis confirmed by CT-FFR and invasive FFR is shown in figure 1.

Case example of use of CT-FFR. 56-year-old man with atypical chest pain. Left: CT coronary angiogram demonstrated a potentially significant (50%–69%) stenosis in the proximal left anterior descendin artery (LAD) (white arrow). Middle: FFRCT analysis demonstrated value of <0.50 in the LAD. Right: the patient underwent subsequent invasive coronary angiography and percutaneous coronary intervention to the proximal LAD lesion (white arrow).
Several algorithms allow CT-FFR calculation, although there is significant variation in the degree of complexity of modelling. These are described in table 1. Due to underlying modelling assumptions, vessels with coronary stents and patients with bypass grafts and severe valve disease are not suitable for CT-FFR analysis, as these alter coronary inflow calculations or outflow conditions.
CT-FFR techniques
In the UK, HeartFlow FFRCT (named this way to distinguish from other CT-FFR techniques) was selected by the National Health Service (NHS) England Innovation and Technology Payment (ITP) programme as a diagnostic tool that warranted further clinical assessment.6 This was following the NICE medical technology appraisal committee (MTAC) report that indicated a potential saving of £214 per patient compared with standard diagnostic pathway.7 Thus, with NHS England funding, there is an opportunity to widely evaluate the real-world application of FFRCT. While this represents a potentially important step in enhancing CAD diagnosis, there is a critical need to understand the opportunities and challenges presented by this new technology before widespread adoption.
Diagnostic accuracy of CT-FFR
Several studies have been published on the diagnostic accuracy of CT-FFR compared with CTCA and invasive FFR (table 2). Compared with other imaging modalities, FFRCT outperformed CTCA and SPECT on a patient and vessel level for diagnosis of significant CAD.8 FFRCT has been shown to have superior diagnostic performance compared with PET on a vessel, but not on a patient, level.8 In comparison with static and dynamic adenosine stress perfusion CT, FFRCT was found to have comparable diagnostic accuracy.9 10 Virtual Functional Assessment Index has shown a good diagnostic accuracy compared with invasive FFR and PET-CT.11 12 To date, there has not been a head-to-head comparison of CT-FFR with stress perfusion cardiovascular magnetic resonance (CMR), which has shown a high diagnostic accuracy.13
Diagnostic accuracy compared with invasive coronary angiography and FFR
CT-FFR as a clinical decision support tool
There are emerging studies that have been performed to determine the impact of CT-FFR on clinical decision-making. In the CT-FFR RIPCORD study, data from the NXT trial were presented to three interventional cardiologists who devised a management strategy based on CTCA alone, compared with FFRCT, to determine impact on clinical decision-making.14 Furthermore, 44% of patients had management pathways altered following availability of FFRCT data, with 36% of patients assigned to either intervention or medical management having their clinical management altered in light of the FFRCT results. In 8% of patients, the culprit vessel requiring revascularisation was reclassified.14 While this was a retrospective, hypothetical study, the changes in recommendations in patient management are striking. In another study, FFRCT changed treatment decisions in 7% of patients for the Heart team reviewing patients with multivessel CAD.15
While CT-FFR may be useful in virtual planning of percutaneous coronary intervention (PCI), it is unable to provide important decision-making information during PCI, which are provided by invasive FFR. Following stent deployment and optimisation, re-checking of invasive FFR ensures immediate haemodynamic outcome of revascularisation is satisfactory. If invasive FFR has already been used as a diagnostic decision-making tool prior to stent insertion, post-stent invasive FFR measurement incurs no additional cost. Indeed, some operators use intracoronary pressure wire as the guidewire for the PCI procedure. A satisfactory increase in post-stenting invasive FFR (typically >0.90) confers a favourable long-term outcome, whereas a persistently low post-stent invasive FFR may indicate suboptimal stent deployment that justifies further stent optimisation. The latter should ideally be guided by intracoronary imaging that may reveal actionable features, such as stent under-expansion, strut mal-apposition, plaque prolapse or thrombus.16 17 Side branches may also be evaluated by invasive FFR after main vessel stent deployment, rather than relying on angiographic appearances to guide further interventions or additional stent deployments, particularly in left main stem bifurcation stenting.18
Invasive FFR allows a quantitative assessment of coronary microcirculation, through measurement of coronary flow reserve which has a diagnostic role in patients with coronary microvascular dysfunction. The index of myocardial resistance gives a readout of overall coronary microvascular resistance that is a clinically applicable biomarker for diagnosis, prognosis and stratification,19 20 which is not possible to derive from CT-FFR.
Outcome and prognostic data for FFRCT
There is emerging evidence regarding outcome and prognosis in patients following FFRCT with low event rates at 90 days21 and 1 year.22 Importantly, no major adverse cardiovascular event (MACE) occurred in individuals in whom a planned ICA was cancelled on the basis of FFRCT findings.22
In the ADVANCE registry, there were no deaths or myocardial infarction (MI) in patients with FFRCT >0.80 and 0.6% MACE rate at 90 days.23 At 1 year, there was a non-significant trend for lower MACE in patients with FFRCT >0.80 compared with FFRCT ≤0.80, with significant lower risk of cardiovascular death or MI.24 Reassuringly, there were no adverse events in those with an FFRCT >0.90. Another study demonstrated a comparable rate of adverse cardiovascular events at 2 years in patients with minor CAD on CTCA and those with moderate disease with an FFRCT >0.80 on optimal medical therapy.25
The 5-year follow-up study of the NXT trial demonstrated that patients with FFRCT >0.80 had significantly lower primary outcome of death, MI and revascularisation, and MACE compared with patients with FFRCT ≤0.80.26 However, the primary outcome was mainly driven by need for revascularisation, and there was no statistical difference for death, cardiac death or non-fatal MI.26 Nevertheless, there are signals from this study that indicate the long-term safety of a FFRCT >0.80, as there were no MI or death in patients with a negative FFRCT. To date, there have been no large-scale, randomised studies of clinical outcomes following a CT-FFR-based strategy to guide revascularisation, as has been with invasive FFR or perfusion CMR.27
Challenges in CT-FFR
Image quality
CT-FFR relies on high-quality imaging, and there are a significant proportion of patient datasets that have been found unsuitable for CT-FFR evaluation in clinical studies. In the NXT28 and PLATFORM studies,21 approximately 12% of cases were rejected from analysis and 33% of CTCA datasets rejected from analysis in the substudy of the PROMISE trial.29 However, the latter trial was a retrospective analysis, and the original study did not intend to derive FFRCT analysis.
The rejection rate of CTCA data for FFRCT analysis was 2.9% in the ADVANCE registry and 8.4% in a large clinical cohort.30 These rejection rates are lower to that previously reported in large multicentre studies which may relate to greater use of dual-source technology30 and improved algorithms. The major determinant for inadequate image quality was motion artefact in approximately 80% of cases that were rejected.30 Multivariate analysis demonstrated various factors independently associated with rejection: these included patient factors (smoking, higher heart rate), scanner/technical factors (detector coverage <16 cm, temporal resolution >100 ms, high tube voltage >120 kVp, aorta contrast opacification) and reconstruction factors (wide field of view and section thickness).
Patient preparation is of paramount importance, and beta blockers and GTN enhance specificity of diagnosis.31 Phase alignment (step) artefacts reduce sensitivity and overall accuracy of CT-FFR,31 32 and these artefacts are reduced with slower, more stable heart rates or larger z-axis coverage. Prior to CT-FFR implementation, an understanding of these factors is required to ensure data acquisition is optimised and will help guide clinicians as to whether CT-FFR analysis is appropriate or technically feasible.
Coronary artery calcification
Coronary calcification has potential to obscure the coronary lumen and blur boundaries for CFD analysis. The higher the Agatston score, the more likely the lumen may be obscured. Equally, lower calcium scores that obscure the lumen may be inappropriate for CFD assessment. In the NXT subanalysis, there was a non- significant trend for decline in diagnostic accuracy with greater Agatston score.33 However, the proportion of patients with very high Agatston score was low, and the study may have been underpowered to detect a significant difference. Thus, the evidence base for diagnostic performance in patients with greater coronary calcification is limited. The factors that impact on image quality for CT-FFR analysis are summarised in table 3.
Reasons for FFRCT data rejection and factors that impact analysis
Interpretation of CT-FFR findings
There are differences between CFD-derived CT-FFR and invasive FFR values. In interventional cardiology, there are well-established cut-off values for haemodynamically significant coronary lesions, with an FFR ≤0.80 used to guide coronary intervention.2 3 FFR range 0.76–0.80 is the ‘grey zone’ which represents an area of clinical uncertainty and challenge in determining the most appropriate clinical management.34 At present, clinicians extrapolate thresholds from invasive FFR to CT-FFR.
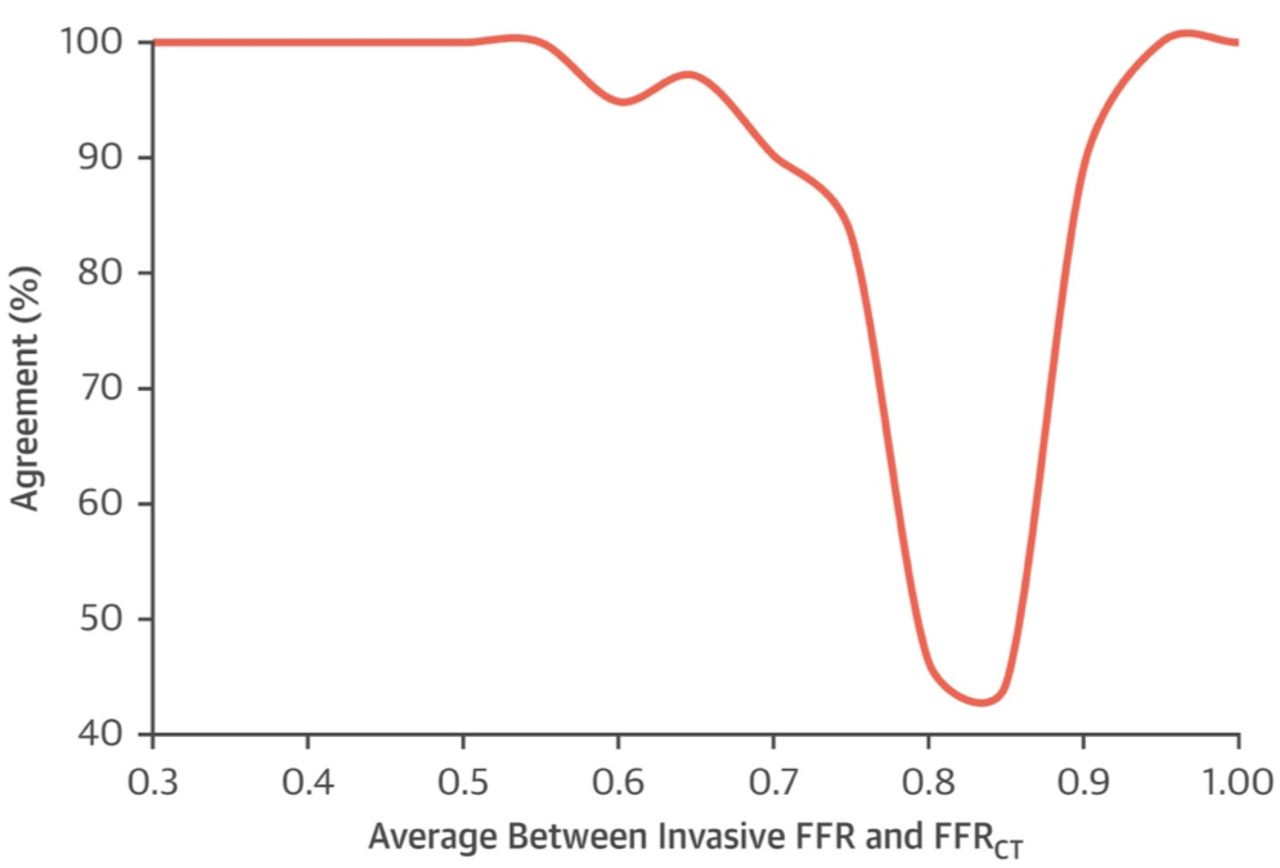
A recent meta-analysis demonstrated a good agreement of invasive FFR with FFRCT values >0.82 and ≤0.74 although poorer agreement in the grey zone (figure 2).35 The variation in diagnostic performance at different FFRCT ranges is not well understood and requires clarification in future studies. However, part of this variation may be the inherent standard deviation in test–retest values of both invasive FFR and CT-FFR values, with reduction in measurement certainty in the grey zone where the impact of this variation in continuous variables becomes important against a binary threshold.36 37

Agreement between invasive fractional flow reserve (FFR) and CT-derived FFR at the different FFR thresholds. Reproduced with permission from Celeng et al.35
CT-FFR has been validated against invasive FFR, which in turn was validated against exercise ECG, SPECT and stress echocardiography.38 CT-FFR is not the ‘ground truth’ and must be interpreted in light of the anatomical findings on the CTCA and clinical scenario. As such, unexpected results from CFD analysis need careful interpretation and awareness of challenges before determining subsequent clinical management and considering whether a repeat analysis should be considered.
Invasive FFR requires pressure readings 20 to 30 mm distal to the stenosis being assessed, at which point post-stenotic laminar flow is restored, avoiding flow eddies and pressure recovery phenomena39; however, the most reliable site of FFRCT measurement is suggested as 10.5 mm distal to the stenosis.40 The reasons for this discrepancy is not clear. In contrast to invasive FFR, CT-FFR provides imaging-derived data on the pressure drop through the course of the entire coronary tree. These FFR values throughout the entire coronary tree may not be intuitive to cardiologists, as it is not common practice to undertake invasive FFR sequentially throughout the entire course of the coronary tree. Importantly, validation studies of CT-FFR were undertaken with a reference standard invasive FFR of specific lesions, rather than every single anatomical point of the coronary tree, as is displayed anatomically in a 3D model from FFRCT. Thus, the validity of the CT-FFR readings through the entire coronary tree remains unknown.
Vessels without focal stenosis on angiography, but with diffuse coronary atherosclerosis, have been shown to have a positive invasive FFR.41 This likely signifies the presence of diffuse atherosclerosis which accumulates along the length of a coronary vessel which causes a pressure drop towards the distal end (figure 3). There are no guidelines that recommend how to manage non-obstructive coronary disease without focal stenosis and positive CT-FFR or invasive FFR. How clinicians should interpret and action these findings on CT-FFR is unclear given the lack of evidence for similar invasive findings. Finally, the use of CT-FFR in serial stenoses is not well understood, and conventional FFRCT and invasive FFR pullback has been found to significantly underestimate true stenosis contribution in serial CAD.42

{kind=link}
{kind=link}
{kind=link}
Case example using CT-FFR. 60-year-old man presenting with atypical chest pain. Calcium score revealed an Agatston score of 582. CT coronary angiography shows multifocal mild stenosis in the left anterior descending and left circumflex artery (A and C). None of these demonstrate significant stenosis, yet there is a sustained and progressive FFRCT drop-off with the distal vessels falling to <0.80 (B and D).
Myocardium at risk and viability
While CT-FFR can provide information on functional significance of coronary artery lesions, the impact of downstream effects on myocardial tissue, in particular ischaemic burden or area at risk, is not available. There are two indications for revascularisation: symptom relief from angina and/or if the myocardial ischaemic burden is prognostically significant. Myocardial ischaemic burden cannot be derived from CT-FFR and requires functional imaging such as SPECT, PET-CT, CMR or stress echocardiography. Furthermore, CT-FFR does not provide information on viability that may help to guide which patients should be considered for revascularisation. Without these important data, it is difficult to determine suitability for revascularisation without recourse to a secondary functional test, which may negate the value of CT-FFR.
Implementation into clinical practice
Little guidance exists on how CT-FFR should be used in the clinical workflow or the true impact on downstream investigations. However, the ability to acquire anatomical and physiological information from a single scan opens up the possibility to develop a ‘one-stop-shop’ for assessment of patients with suspected CAD. Such a pathway may involve clinic consultation, patient preparation, image acquisition, post-processing and CT-FFR analysis and a management plan with medical therapy and options of revascularisation discussed with clinical decision-makers. This has potential to reduce downstream use of healthcare resources through reduced secondary investigations and ICA, reduce hospital visits and improve clinical outcomes through earlier initiation of treatment.
Such a model requires co-ordination between radiologists and imaging/interventional cardiologists with an understanding of the clinical scenario, image optimisation and appreciation of limitations of CT-FFR in order to make informed decisions with patients. Cases may need to be discussed at multidisciplinary meetings, or alternatively, with close collaborative interaction between clinicians during patient visits. CT-FFR may be used to provide timely diagnostic information, institute timely medical therapy and plan appropriate revascularisation in those with the high risk lesions.
HeartFlow recommends FFRCT in lesions with a 30%–90% luminal stenosis. However, the authors’ experience is that appropriate clinical use should consider factors beyond just that of degree of stenosis. CT-FFR may be best served in lesions with intermediate, or greater, stenosis (ie, >50% luminal stenosis on CTCA) and possibly those with 30%–50% luminal narrowing with additional high-risk features, such as adverse plaque characteristics (positive remodelling, low attenuation plaque) or where the lesion length may lead to functional significance (approximately 15–20 mm).43 Clinicians need to consider location of lesions, as small distal lesions may not be amenable to PCI or surgery and therefore CT-FFR would not change clinical management. Considering the recent ISCHEMIA trial data,44 OMT may be all that is required as an initial strategy for all but significant left mainstem, proximal LAD and multi-vessel disease. As with functional imaging, it may be that CT-FFR may be best to determine correlation of anginal/chest pain symptoms with the flow consequences of any given lesion, but not necessarily be optimal to guide revascularisation strategies. Further studies are required to evaluate this in more detail.
Several questions remain unaddressed with regards to CT-FFR. These include, but are not limited to, the following: What additional training is required to interpret CT-FFR and communicate these succinctly to referring physicians to aid clinical decision-making? Who will be the gatekeeper of this technology and decide on appropriate referrals? What is the appropriate cut-off for referral for CT-FFR? Who should integrate CT-FFR into the CTCA report—radiologists, cardiologists or both? How should the reporting physician deal with discrepant findings from CTCA and CT-FFR? Currently, there are no recommendations to address these issues and they need to be considered carefully before implementation of CT-FFR into wider clinical practice.
In England, there is a major potential challenge when the NHS England ITP funding ceases on 31 March 2020. The current payment for a CTCA under the NHS payment scheme is £277, while FFRCT analysis costs £530 for analysis. Individual departments will therefore face a shortfall in reimbursement from April 2020, if requesting FFRCT, when the ITP ends, despite projected cost-saving across the whole patient pathway as determined by NICE MTAC and PLATFORM study.22 CTCA is commissioned locally and local funding agreements will be required prior to routine implementation of FFRCT in most NHS institutions. At present, there is little available hard evidence that demonstrates the reality of reduced downstream savings. This is an area that requires further research, but this will likely not be available prior to the end of the NHS England ITP funding.
Future applications
FFRCT may be used to derive pre-stenting and post-stenting FFRCT values through virtual modelling.45 As such, FFRCT with virtual planning may have further potential as a clinical decision-making tool to guide treatment planning prior to planned ICA and revascularisation. While not available for use in clinical practice, HeartFlow technology does include algorithms that allow the ability to virtually remodel the lumen (online supplementary video 1, Courtesy of HeartFlow).
Supplementary video
CT-FFR may be integrated with plaque markers associated with adverse outcome such as positive remodelling,46 low-attenuation plaque,47 perivascular fat48 and automated quantitative plaque analysis.49 CT-FFR may be integrated with other parameters such as wall shear stress and axial plaque stress to risk stratify and guide therapeutics at a lesion, vessel and patient level. This has recently been demonstrated in a study in which adverse plaque characteristic and adverse FFRCT had significantly higher risk of a culprit vessel for an acute coronary syndrome.50 Larger-scale studies may determine if the combinations of additional CT biomarkers have the potential to elevate coronary CFD to a predictive tool, rather than a diagnostic tool that provides a relatively limited and binary CT-FFR result.
Finally, deep learning may be applied to CTCA and CT-FFR combined with clinical patient data in order to enhance diagnostic accuracy, predict cardiovascular outcomes and guide therapeutics.
Summary
CT-FFR is a potentially valuable and cost-saving adjunct to CTCA in intermediate coronary stenosis. Given the primacy of CTCA as first-line test in NICE chest pain guidelines, and prominent inclusion in recent European Society of Cardiology (ESC) chronic coronary syndrome guidelines, CT-FFR has potential to expand the role of this simple imaging technique. While it remains an exciting opportunity to obtain anatomy and estimated physiology from a single study, high-quality images from adequate patient preparation and high-calibre image acquisition are a prerequisite. Challenges remain for clinical interpretation and communication to patients and physicians. For healthcare systems to embrace this technology, the integration into the clinical workflow needs to be properly understood and financial limitations need to be overcome. Furthermore, there is a clear need for long-term clinical and economic outcome data, which will be the focus of future research. This will determine whether CT-FFR will become a routine adjunct to CTCA or become an integral component of clinical pathways in patients with suspected CAD.
References
Footnotes
Twitter @jweirmccall
Contributors MSN and EDN conceived the idea of the manuscript. MSN drafted the initial manuscript. TKM, JW-M, KN, KC and EDN all critically revised the manuscript. All authors read and approved the final manuscript.
Funding MSN is funded by a Clinical Lecturership awarded by the UK National Institute for Health Research.
Competing interests KN declares unrestricted, institutional research support from Siemens Healthineers, Bayer Healthcare and HeartFlow Inc.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Obtained.
Provenance and peer review Commissioned; externally peer reviewed.