Article Text

Abstract
Objectives The 1916 Royal Commission on Venereal Diseases was established in response to epidemics of syphilis and gonorrhoea in the UK. In the 100 years since the Venereal Diseases Act (1917), the UK has experienced substantial scientific, economic and demographic changes. We describe historical and recent trends in STIs in the UK.
Methods We analysed surveillance data derived from STI clinics’ statistical returns from 1917 to 2016.
Results Since 1918, gonorrhoea and syphilis diagnoses have fluctuated, reflecting social, economic and technological trends. Following spikes after World Wars I and II, rates declined before re-emerging during the 1960s. At that time, syphilis was more common in men, suggestive of transmission within the men who have sex with men (MSM) population. Behaviour change following the emergence of HIV/AIDS in the 1980s is thought to have facilitated a precipitous decline in diagnoses of both STIs in the mid-1980s. Since the early 2000s, gonorrhoea and syphilis have re-emerged as major public health concerns due to increased transmission among MSM and the spread of antimicrobial-resistant gonorrhoea. Chlamydia and genital warts are now the most commonly diagnosed STIs in the UK and have been the focus of public health interventions, including the national human papillomavirus vaccination programme, which has led to substantial declines in genital warts in young people, and the National Chlamydia Screening Programme in England. Since the 1980s, MSM, black ethnic minorities and young people have experienced the highest STI rates.
Conclusion Although diagnoses have fluctuated over the last century, STIs continue to be an important public health concern, often affecting more marginalised groups in society. Prevention must remain a public health priority and, as we enter a new era of sexual healthcare provision including online services, priority must be placed on maintaining prompt access for those at greatest risk of STIs.
- sexual health
- surveillance
- gay men
- ethnicity
- adolescent
Statistics from Altmetric.com
Introduction
The Royal Commission on Venereal Diseases of 1916 was established in response to widespread epidemics of syphilis and gonorrhoea in the UK.1 At that time, syphilis was considered to be a leading cause of death, stillbirths, infant mortality and blindness, and gonorrhoea was a leading cause of infertility in women.2 The subsequent passage of the Venereal Diseases Act of 1917 facilitated the provision of free, confidential, open-access STI clinics in an attempt to prevent and control these infections.1 3 While their epidemiology has changed remarkably over the last century, STIs continue to negatively impact the health and well-being of the population.4
For this reflective overview, we review and discuss STI surveillance data derived from mandatory statistical returns from STI clinics over the 100 years since the passage of the Venereal Diseases Act (1917). Data were primarily derived from aggregated statistical returns from STI clinics, but in more recent years were also derived from disaggregated electronic data from STI clinics and laboratories.5 Data on gonorrhoea and syphilis were available from 1918 and 1922, respectively. Data on causes of morbidity were collected prior to this; however, STI-related morbidity was understood to be severely under-reported: ‘Syphilis had been, and remained, the despair of the statistician … Even in death a stigma was associated with it.’2
The aggregated returns from STI clinics contain limited demographic data, but provide key insights into historical STI trends. Gender data have been available for syphilis and gonorrhoea since 1925, and high male:female ratios have been used to infer trends among gay, bisexual and other men who have sex with men (MSM). In the last 10 years, the availability of disaggregated data in some UK countries has enabled more in-depth exploration of the population subgroups affected. The results of descriptive analyses are reported, with a focus on primary, secondary or early latent syphilis (hereafter: ‘syphilis’), gonorrhoea, chlamydia and first episode genital warts (hereafter: ‘genital warts’), and first episode genital herpes (hereafter: ‘genital herpes’).
We used this review of surveillance data to compare and contrast the historical and current epidemiology of STIs, explore the factors contributing to the high diagnosis rates of STIs among select population subgroups in recent years, then discuss implications for the future provision of STI services.
Trends in gonorrhoea and syphilis from 1918 to the early 2000s
As previously described,5 diagnoses of gonorrhoea and syphilis have fluctuated since 1918, reflecting social, economic and technological trends. Briefly, after the return of the armed forces to the UK at the end of World War I in 1918, diagnoses of syphilis and gonorrhoea both exceeded 35 000 annually (figure 1A,B and online supplementary appendix tables 1 and 2). This was followed by a slow decline in cases for two decades, after which the number of diagnoses of both infections increased sharply in the mid-1940s at the end of World War II. Subsequently, there was a rapid decline in both infections, facilitated by the mass production of penicillin, until the number of diagnoses of both STIs reached a nadir the decade later. However, following the period of sexual liberation of the 1960s,6 diagnoses of both infections increased, with gonorrhoea returning to levels unseen since the late 1940s. In the case of syphilis, far more cases were reported in men (figure 1C), suggesting that sex between men became the predominant route of transmission. During the 1980s, there was another precipitous decrease in cases, thought to be due to behaviour change in response to the emergence of HIV/AIDS in the 1980s, the related public health campaigns and the high case-fatality rate of HIV/AIDS at that time. While diagnoses of both STIs remained very low during the 1990s, there has been a re-emergence of both gonorrhoea and syphilis in MSM since 2000.5
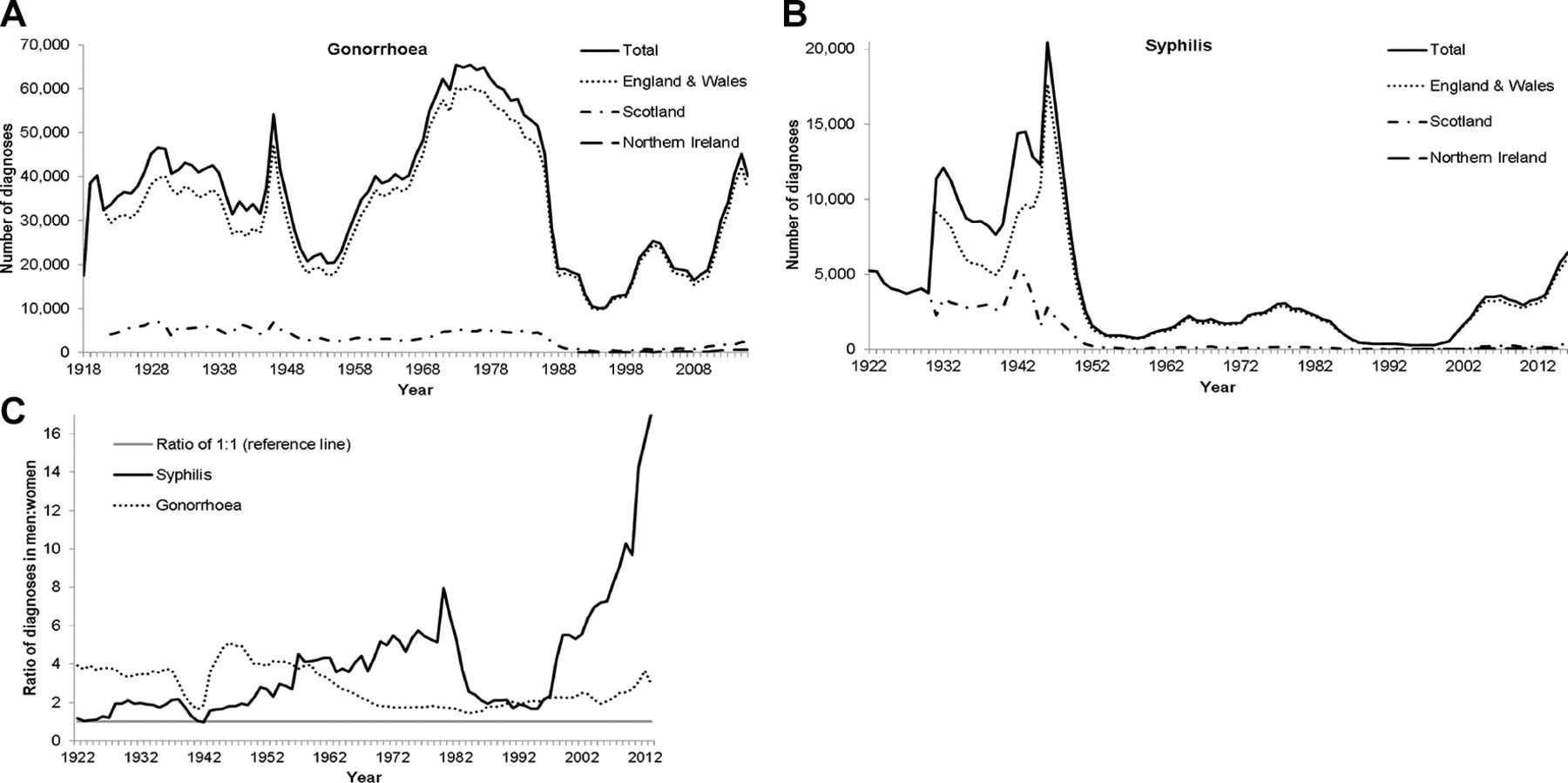
(A) Number of diagnoses of gonorrhoea, 1918–2016, (B) number of diagnoses of primary, secondary and early latent syphilis, 1922–2016, and (C) ratio of diagnoses of gonorrhoea and primary, secondary and early latent syphilis in men and women, 1925–2016; STI clinics, UK.*⁰† Different scales are used for the y-axes of each of the above graphs. *Data from Northern Ireland are available starting the year 1991. ⁰Scotland data from 1995 are unavailable. †Data from STI clinics’ routine surveillance returns and routine laboratory reporting syphilis data are only Scotland 1922–1930; England, Wales and Scotland 1931–1990; and all countries from 1991 onwards (except for 1995, which is missing Scotland data) Gonorrhoea data are only England and Wales 1918–1921; England, Wales and Scotland 1922–1990; and all countries 1991 onwards (except for 1995, which is missing Scotland data).
In the following sections, we describe more recent trends in STIs in the UK then explore inequalities in STI distribution by population subgroups.
Recent STI trends in the UK
Currently, STI surveillance data from all UK countries are available for chlamydia, gonorrhoea and syphilis. In 2016, there was a combined total of 276 134 diagnoses of these STIs, with the most commonly reported (83.1%) being chlamydia; the majority of diagnoses of gonorrhoea (74.7%) and syphilis (94.4%) were in men, while more chlamydia diagnoses (57.2%) were in women.7 Between 2012 and 2016, there were increases in the numbers of gonorrhoea (33.5%) and syphilis (93.3%), whereas chlamydia diagnoses decreased by 5.0%. The majority (88.6%) of the overall total of these three STI diagnoses were made in English STI clinics, which heavily influences the UK-wide trends; slightly different trends were observed in the other countries of the UK.8–10
Adolescents and young adults
Teenagers and young adults experience the highest diagnosis rates of chlamydia and gonorrhoea (figure 2 and online supplementary appendix figure 1); this has been recognised at least since the 1980s, when roughly one-third and one-eighth of chlamydia and gonorrhoea diagnoses, respectively, were in those under 20 years.11 In the 1990s, women aged16–19 years had the highest diagnosis rates of gonorrhoea, chlamydia and genital warts, and the second highest rate (after women aged 20–24 years) of genital herpes.12 Currently, among those aged 15–24 years, men are 3 and women are 11 times more likely to be diagnosed with chlamydia, gonorrhoea or syphilis than their counterparts aged 25–64 years (figure 2). The age disparity in STI rates is likely due to higher partner turnover in young people. Compared with older people, those aged 16–24 years are most likely to report a new sex partner or two or more sex partners of the opposite sex in the previous year.13
Supplemental material

Rates of chlamydia, gonorrhoea or syphilis* diagnoses. †By age group and gender, 2016, UK. *Primary, secondary and early latent stages. †Data from STI clinics’ routine surveillance returns and routine laboratory reporting.
There is a marked disproportionality in diagnosis rates by gender in those aged 15–19 years and women are now 2.8 times more likely to be diagnosed with chlamydia, gonorrhoea or syphilis than men in this age group (figure 2).11 To some extent the disparity will reflect improved access to STI testing among younger women in a range of clinical settings, including through the National Chlamydia Screening Programme (NCSP) in England,4 but it may also be due to disassortative sexual mixing patterns between young women and older male partners14 15 or greater biological susceptibility to STIs among younger women.16
Chlamydia is the most commonly diagnosed STI in the UK, and the highest diagnosis rates are reported in those under the age of 25 years.4 Testing was only readily available since the mid-1990s, and since then widespread testing, which in England was facilitated by the NCSP, led to a rapid increase in chlamydia diagnoses.17 The NCSP offers opportunistic screening of sexually active young people aged 15–24 years with the aim of increasing the detection of chlamydia and reducing the prevalence of associated sequelae. Chlamydia screening programmes have not been implemented in other countries of the UK.18 However, widespread chlamydia testing in Scotland was driven by changes implemented following the publication of the Scottish Intercollegiate Guideline Network guidance in 2000; this recommended urine sampling and the use of sensitive, specific nucleic acid amplification tests.19
Historically, young women have also experienced much higher rates of genital warts than older women,12 but recent years have seen marked declines in the younger age groups (online supplementary appendix figure 2), likely associated with the introduction of the UK schools-based human papillomavirus vaccine (HPV) programme in 2008.20 In England in 2016, the diagnosis rate of genital warts in girls aged 15–17 years, most of whom would have been offered the quadrivalent vaccine when aged 12–13 years, was 121.5 per 100 000 population, a 72% decrease relative to 2009. There has been a 62% decrease in the diagnosis rate of genital warts in boys aged 15– 17 years over the same time period, providing evidence of herd protection from the high-coverage female HPV vaccination programme.4 Similar reductions have not been seen in older age groups. This school-aged vaccination programme offers no protection to MSM so a targeted HPV vaccination programme for MSM will be introduced in England in April 2018 following an initial pilot that ran from 2016.21 HPV vaccination has been offered opportunistically to MSM in Northern Ireland since October 2016 and Scotland since July 2017. HPV vaccination of MSM will provide direct protection against HPV infection with the aim of reducing the incidence of genital warts and HPV-related cancers.
Supplemental material
Gay, bisexual and other MSM
In the last decade, MSM have continued to be disproportionately affected by STIs including HIV, as well as bloodborne infections, such as hepatitis B and C, and sexually transmissible enteric infections, such as Shigella flexneri.5 22–28 While only 11% of all attendances at English STI clinics in 2016 were by MSM, 53% of all gonorrhoea and syphilis diagnoses were made in this group. The number of diagnoses of these bacterial STIs in MSM in England has risen threefold to fivefold over the last decade (figure 3). In 2016, the total number of syphilis diagnoses at STI clinics in England increased to 5920, the largest number reported since 1949; the majority (81%) were in MSM. Similarly, in Scotland, syphilis diagnoses have doubled since 2014 to 356 in 2016, the largest number recorded since 1951; the majority (83%) were made in MSM.29

Number of new diagnoses of selected STIs in men who have sex with men attending STI clinics†, 2007–2016, England. Different scales are used for the y-axes for (i) chlamydia and gonorrhoea and (ii) genital herpes, genital warts and syphilis. *First episode. **Primary, secondary and early latent. †Data from routine specialist and non-specialist sexual health services’ returns to the Genitourinary Medicine Clinic Activity Dataset surveillance system.
Several factors likely explain these increases. Studies suggest that increased frequency of condomless anal intercourse (CAI), sometimes associated with HIV seroadaptive behaviours, group sex facilitated by geosocial networking applications and ‘chemsex’, may play a role.30 31 The sevenfold rise in gonorrhoea diagnoses among MSM in England between 2007 and 2015, which has been mirrored in Wales and Northern Ireland,9 10 and to a similar extent in Scotland based on male rectal diagnoses,8 may also be partly explained by increased detection following the change in the national gonorrhoea testing guideline to include asymptomatic screening at extragenital sites in MSM using highly sensitive nucleic acid amplification tests.32–36 In England, after years of successive increases since 2008, the number of gonorrhoea diagnoses in MSM decreased 22% to 17 584 between 2015 and 2016. This decline coincided with reductions in HIV diagnoses which have been associated with improved HIV testing uptake at STI clinics, including repeat testing; prompt initiation of antiretroviral treatment following diagnosis and irrespective of immune status to prevent onward transmission (‘treatment as prevention’); and private access of HIV pre-exposure prophylaxis.37 38 Increased STI testing uptake at STI clinics occurred in parallel and may have helped facilitate prompt identification and treatment of asymptomatic infection, reducing the likelihood of secondary transmission. More targeted, quarterly syphilis testing, especially in HIV-positive MSM, may be required to effect a reduction in syphilis incidence.39 40
Black minority ethnic populations
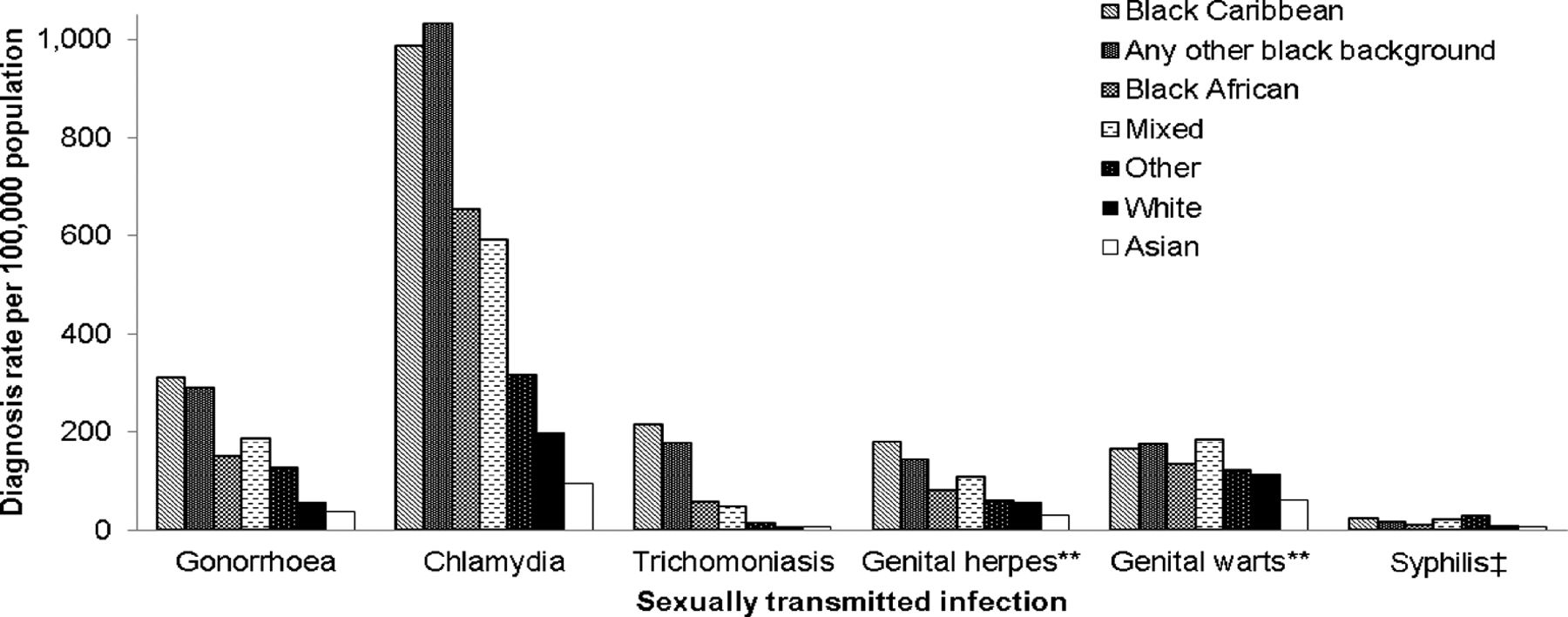
In 2016, data from England showed that diagnosis rates of chlamydia and gonorrhoea in black Caribbean populations were four times those of the general population. Similarly, in Wales in 2015, the gonorrhoea diagnosis rate in black populations was three times that of white populations.9 The ethnic disparity in poor sexual health is even starker in the case of trichomoniasis where, in 2016 in England, the diagnosis rate in black Caribbean women was 14 times that of all women. There is considerable heterogeneity in STI diagnoses among black ethnic minority (BME) groups: black Caribbean and black non-Caribbean/non-African people (hereafter: ‘any other black background’) have the highest diagnosis rates of many STIs of all ethnic groups, while black Africans have relatively lower rates (figure 4).41 42
{kind=link}
![[SP3.jpg]](https://sti.bmj.com/content/sextrans/94/8/553/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
![[SP4.jpg]](https://sti.bmj.com/content/sextrans/94/8/553/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Rates of selected STI diagnoses* by ethnic group and STI, 2016, England. *Data from routine specialist and non-specialist sexual health services’ returns to the Genitourinary Medicine Clinic Activity Dataset surveillance system. **First episode. ‡ Primary, secondary and early latent.
Disproportionately higher rates of gonorrhoea in black Caribbean people in urban areas have been recognised since the 1950s and have persisted to the present day.42–47 Since the mass wave of migration of people from the Caribbean and elsewhere in the British Commonwealth to the UK after the British Nationality Act of 1948,48 most black Caribbean and other BME people have resided in the most deprived urban areas of England.42 There is an inextricable link between the socioeconomic context of neighbourhoods and the health outcomes of their residents.49 Sexual health is no exception, and evidence suggests that socioeconomic deprivation plays a role in ethnic disparities in STI diagnosis rates, although it does not fully explain it.42 Behavioural factors, which are themselves influenced by socioeconomic environment, likely contribute. The findings of a national probability sample indicate that men of black Caribbean or any other black backgrounds are most likely to report higher numbers of recent sexual partners and concurrent partnerships which, coupled with assortative sexual mixing patterns, may be maintaining endemic levels of gonorrhoea transmission in these communities.50 Data from England also suggest that BME MSM are more likely to be diagnosed with a bacterial STI and are at greater risk of HIV than white British MSM, a disparity which may be explained by differences in health-seeking behaviour or sexual mixing patterns.51 52
Discussion
Since the introduction of the Venereal Diseases Act (1917) 100 years ago, the complex interplay of historical events, changes in cultural mores, and technological and service developments are clearly reflected in the STI surveillance data presented.5 More recently, there has been a re-emergence of gonorrhoea and syphilis among MSM, likely associated, at least in part, with increasing CAI as a result of HIV treatment optimism.30 53 54 The rise in gonorrhoea diagnoses is of particular concern given the propensity of Neisseria gonorrhoeae to develop resistance to successive antimicrobials used for treatment.55 56 However, there have also been notable successes in STI prevention in the last decade: following the implementation of the national HPV vaccination programme in school-aged girls, diagnoses of genital warts have declined markedly in young adults, and future reductions in HPV-related cancers are anticipated. w1 2
Accurate and easy-to-perform diagnostic tests are fundamental for early diagnosis and effective treatment, as well as informing our understanding of the epidemiology of STIs. The key development in the last 100 years was a shift in the method of confirming a bacterial STI diagnosis from one based on symptoms to one of defining asymptomatic people as carriers of a pathogen. For example, in 1917 syphilis diagnosis depended solely on microscopic identification of the organism but, with advances in immunological techniques, serological assays were used routinely to provide more accurate results by the 1930s. In the 1970s the creation of monoclonal antibodies allowed the production of highly specific methods of testing patients for infections. w3 The development of nucleic acid testing in the 1990s led to accurate, high-volume, low-cost tests which are now routinely used in the UKw4 5 and are likely to have contributed to the sharp rise in gonorrhoea diagnoses in England after 2010.w6
Regular testing for STIs, especially in those individuals at higher risk of infection, has been promoted through both targeted, public facing campaign work and changes in clinical and diagnostic practice. For example, clinical recommendations that MSM should test regularly for HIV (and thus, by extension, STIs) have been reinforced by promoting testing among MSM through campaigns such as National HIV Testing Week in England and the European HIV-Hepatitis Testing Week. National provision of pre-exposure prophylaxis for HIV (PrEP) has been forecast to reduce STIs in MSM due to the increased STI screening required for PrEP management.w7 This has not yet been observed in practice, but the National Health Service-funded HIV PrEP programme in Scotland and national implementation trials in Wales and England will provide a unique opportunity to assess this on a national scale.w8-10
Promoting condoms, early diagnosis, access to effective treatments and effectual partner notification are key components of the prevention and control of STIs by interrupting onward transmission of infection, especially in high-risk groups.38 Access to STI clinics has improved over the last 10 years, and there are now >4 million attendances at STI clinics annuallyw11 and this marked improvement is in part due to the introduction of access targets for STI clinics in England in 2006.w12 Although in 2011 nearly everyone (99.9%) was offered an appointment within 48 hours,w13 there has since been a worrying worsening of service access, especially for symptomatic patients and women.w14 Ensuring prompt access to those in need should remain a priority, especially given significant reorganisations in sexual health service provision and reductions in spend on services.w15-17
In the current climate of reduced funding, cost-saving measures, such as the scale up of online service provision using STI self-sampling kits, are being pursued.w17 w18 An objective of a new service model for London residents is to direct patients to online services rather than attending terrestrial STI clinics.w18 This has the potential to increase access to testing,w19 but care must be taken to avoid exacerbating sexual health inequality through the digital divide;w20-22 this is of particular concern for BME people from socioeconomically deprived areas, who experience disproportionate sexual ill-health.42 It is vital that STI surveillance systems continue to adapt to capture this shift in service provision and thereby enable evaluation of its real-life impact.w23
There are promising developments on the horizon. Recently published case–control data from New Zealand provide evidence of a protective effect of group B meningococcal vaccine for gonorrhoea;w24 25 if this is corroborated by robust clinical trial data, improved control of gonorrhoea is potentially within reach. Furthermore, the widespread use of geosocial networking applications presents novel opportunities for both sexual health education and promotion.w26 New developments in STI prevention should supplement more traditional approaches: condom use is a highly effective intervention to control the transmission of STIs and should continue to be promoted.w27
Despite the myriad economic and societal changes over the last century, STIs continue to be associated with stigma, discrimination and socioeconomic inequality. The means to prevent and control STIs are readily available, and in the UK the key mechanism for their delivery is through open-access clinics. As we enter a new era of sexual healthcare provision, we must ensure that innovation in interventions and their delivery continue to meet population needs as well as reduce health inequalities.
Key messages
STIs are a major public health concern and disproportionately affect men who have sex with men (MSM), black ethnic minorities and young people.
Gonorrhoea and syphilis diagnoses have fluctuated considerably over the last century but have recently re-emerged especially among MSM, in part associated with HIV seroadaptive behaviours.
STI interventions including the promotion of risk reduction, increased and improved testing, and vaccination have led to improvements in sexual health.
As originally envisaged in 1917, there is a need to maintain free, confidential, open-access sexual health services for those in need.
Supplemental material
Supplemental material
Supplemental material
Acknowledgments
The authors acknowledge the contribution of all sexual health services to the surveillance of STIs since the inception of these surveillance systems. They also thank Ian Simms for his insight on the history of the UK’s STI surveillance systems and Peter Kirwan for further editorial input.
References
Footnotes
Handling editor Jackie A Cassell
Contributors HM, PB and GH designed the data analysis plan. HM, PB, DO, SD and MC performed the data analysis. HM wrote the first draft of the paper, which was reviewed and edited by all coauthors.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval As GUMCAD is a routine public health surveillance activity, no specific consent was required from the patients whose data were used in this analysis. In its role providing infectious disease surveillance Public Health England it has permission to handle data obtained by GUMCAD under Regulation 3 of the Health Service (Control of Patient Information) Regulations 2002. Public Health Wales, the Public Health Agency and Health Protection Scotland have a statutory function to carry out surveillance of communicable disease.
Provenance and peer review Commissioned; externally peer reviewed.