Article Text

Abstract
Objectives Do Not Attempt Cardio-Pulmonary Resuscitation (DNACPR) discussions with patients and their caregivers have been subjected to intense ethical and legal debate in recent years. Legal cases and national guidelines have tried to clarify the best approach to DNACPR discussions; however, there is little evidence of how best to approach them from the patient, family or caregiver perspective. This paper describes published accounts of patient, family and caregiver experiences of discussions about advance cardiopulmonary resuscitation (CPR) decision making.
Methods An integrative review of the UK literature between 2000 and 2016 including qualitative and quantitative studies was conducted. Worldwide, 773 abstracts were identified, and 20 papers from the UK were included in the final analysis.
Results Patient, family and caregivers prefer discussions to be initiated by someone trusted, and wishes for family involvement vary depending on the context. Timing of discussions should be individualised, though discussions earlier in the illness are often preferable. Discussions held in the acute setting are suboptimal. CPR decisions should be part of a wider discussion about future care and adequate communication skills training is important.
Conclusions The findings of this review are at odds with the current statutory framework and potentially challenging for medical professionals who are working in a stretched health service, with pressure to discuss DNACPR decisions at the earliest opportunity. With increasing focus on person-centred care and realistic medicine, patient narratives must be considered by doctors and policy makers alike, to minimise harm.
- clinical decisions
- communication
- family management
- integrative review
- resuscitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Do Not Attempt Cardio Pulmonary Resuscitation (DNACPR) decision making has been the subject of much ethical debate, legal dispute and uncertainty in the last few years. Cardiopulmonary resuscitation (CPR) is a treatment that was developed originally to save the lives of younger people dying unexpectedly from primary cardiac disease1 and it was never intended to be given to patients who are dying of irreversible underlying disease.2 3 However, CPR is often misunderstood as a procedure that can restore cardiopulmonary function and prolong life, irrespective of the underlying cause of the cardiac arrest.1
Public perception of CPR has been influenced by the media, as it is often portrayed as more effective and less harmful than in reality. This can influence care decisions made during serious illness and at end of life (EOL).4 Not only this, but there are many reasons why patients, family and caregivers (PFC) may find talking about death and dying difficult, for example, fear of: loss; their own mortality; being a burden on or upsetting family and friends and denial.5
It is well documented that medical staff find initiating DNACPR discussions with patients difficult due to fear of causing distress, time constraints1 as well as fear of complaints.6 7 However, there is genuine potential for harm when communication about CPR and DNACPR decisions is inadequate. Numerous reviews in the UK have found deficiencies in considering, discussing and implementing DNACPR discussions, resulting in either futile or inappropriate CPR attempts, poor or delayed discussion of DNACPR decisions and inappropriate withholding of other treatments.1 6 This has also been highlighted in vulnerable patient groups such as those with learning difficulties, where a poor understanding of the Mental Capacity Act (2005) by healthcare professionals as well as inappropriate or poorly documented DNACPR orders has been noted.8
Across the four countries in the UK, recent legal cases, which are outlined in box 1, have brought the DNACPR decision-making process in to the spotlight. It is now unlawful to make and document a DNACPR decision without informing the patient or those close to the patient, unless that conversation would cause physical or psychological harm9 (to the patient) or would not be practicable or appropriate (informing those close to a patient who lacks capacity). Failure to provide this information out with these circumstances is legally deemed to be in contravention of a patient’s Human Rights. National guidance in the UK from the British Medical Association (BMA), Resuscitation Council (UK) and the Royal College of Nursing (RCN) has been updated,10 including updated decision-making frameworks in an attempt to clarify the meaning of this new terminology so healthcare professionals can address this complexity (box 2).
Legal cases in the UK involving DNACPR discussions and the Human Rights Act
Tracey vs Cambridge University Hospital NHS FT (2015)
Where a Do Not Attempt Cardio-Pulmonary Resuscitation (DNACPR) decision has been made, as per the case of Tracey vs Addenbrookes in 20159, Lord Dyson stated that ‘there should be a presumption in favour of patient involvement [in the decision]. There needs to be convincing reasons not to involve the patient’. When a decision is made not to administer cardiopulmonary resuscitation (CPR) in the event of cardiac arrest, article 8 of the Human Rights Act (the right to a private and family life) is engaged because it concerns how an individual chooses to pass the closing days and moments of their life and how they manage their own death. By not informing the patient that you have made the decision that CPR would be futile, you deny them the opportunity to seek a second opinion about whether it would be futile.49 Distress is no longer reason enough to justify withholding discussions about DNACPR decisions with patients. The Court of Appeal stated that many patients may find involvement in this discussion distressing, but that unless this discussion would cause physical or psychological harm, then this is not reason enough to deny them the opportunity.
Montgomery vs Lanarkshire Health Board (2015)
In another relevant case regarding consent Montgomery vs Lanarkshire, 50 the Supreme Court ruled that doctors must take reasonable care to discuss with patients any material risk involved with any treatment as well as any alternative treatments (a material risk being one which the patient may attach significance to and may affect their decision to undergo that treatment). While the Montgomery case was about treatment, it must apply to investigations as well as decisions not to investigate or treat. 49
Winspear vs City Hospitals Sunderland NHS Foundation Trust (2015)
It was ruled in November that the decision to impose a DNACPR order on a 28-year-old man with cerebral palsy without the knowledge of his family was a violation of article 8 of the Human Rights Act.51 Section 4 (7) of the Mental Capacity Act 2005 provides that: ‘[The decision-maker] must take into account, if it is practicable and appropriate to consult them, the views of… anyone engaged in caring for the person or interested in his welfare.’ Mr Justice Blake said that the core principle of prior consultation before a DNACPR decision … applied in cases both of capacity and absence of capacity. In the case of persons who lacked capacity, the 2005 Act spelled out when and with whom a decision-taker had to consult. If it was not ‘practicable or appropriate’ to consult a person identified in section 4 (7) before the decision was made or acted on, there would need to be a convincing reason to proceed without consultation. If, on the other hand, it was both practicable and appropriate to consult, then in the absence of some other compelling reason against consultation, the decision to file the DNACPR notice on the patient’s medical records without prior consultation would be procedurally flawed. 52
Andrew Waters vs East Kent Hospitals NHS trust (2015)
Doctors from the East Kent Hospitals NHS trust placed a DNACPR order for this 53-year-old man, citing reasons for the decision as ‘Downs Syndrome, unable to swallow (PEG fed), bed bound, learning difficulties’.53 This DNACPR decision was not discussed the patient’s family and the form was only discovered after discharge by the patient’s carers. The family had been in regular attendance to the hospital but had never been informed of the decision. The courts found this to be a contravention of human rights for the DNACPR order to have been put in place without first discussing it with the patient’s relatives.
Decisions Relating to CPR. 3rd Edition10 (1st Revision 2016): Key Messages from the British Medical Association
Anticipatory decisions about cardiopulmonary resuscitation (CPR) are best made in the wider context of advance care planning.
If the healthcare team is as certain as it can be that a person is dying, CPR should not be attempted.
Even when CPR has no realistic prospect of success, there must be a presumption in favour of explaining the need and basis for a Do Not Attempt Cardio-Pulmonary Resuscitation (DNACPR) decision to a patient or to those close to a patient who lacks capacity.
Where there is a clear clinical need for a DNACPR decision in a dying patient for whom CPR offers no realistic prospect of success, that decision should be made and explained to the patient and those close to the patient at the earliest practicable and appropriate opportunity.
Where a patient or those close to a patient disagree with a DNACPR decision a second opinion should be offered.
Agreeing broader goals of care with patients and those close to patients is an essential prerequisite to enabling each of them to understand decisions about CPR in context.
A decision to delay or avoid communication of a decision to a patient must be based on that communication being likely to cause the patient physical or psychological harm. A decision to delay communication of a decision to those close to a patient without capacity must be based on that communication being either not practicable or not appropriate in the circumstances.
All decisions must be clearly documented in the patient’s notes.
A DNACPR decision must not be allowed to compromise high quality delivery of any other aspect of care.
Although discussions about EOL issues and anticipatory care planning (ACP) can be challenging, changing the focus of these discussions from specific treatments (such as CPR), to discussions around goals of care, acceptable health states for patients and valued life, might be more acceptable.11 A UK-wide initiative, the Recommended Summary Plan for Emergency Care and Treatment (ReSPECT) process,12 complements the process of ACP. It focuses on incorporating personalised recommendations for a person’s realistic care and treatment choices in future emergency situations, where they are unable to make or express choices, of which DNACPR decision making is one aspect. Shifting the focus from specific decisions about CPR, to making personalised plans on broader emergency care and treatment choices, may help tackle some of the difficulties clinicians face with DNACPR decision making and communication.3
It seems unfortunate that many lessons and policy-changes on DNACPR decision making in the UK have come from cases highlighting deficiencies or poor practice. Medical staff often rely on communication skills training, which is based on perceived best practice from studies examining subjective views of people who may not have actually experienced discussions about CPR. Instead, communication skills training should be informed primarily by evidence from the lived experience of patients, families or caregivers who have experienced discussions about CPR decision making.
Patient-centred care is one of the visions set out for a ‘better National Health Service’ (NHS) in the UK Government’s White Paper.13 A richer understanding of patient and family experiences of DNACPR discussions will enhance our evidence base regarding CPR decision making and communication and inform educational processes and policy to guide medical practitioners on how to approach these conversations in the UK. The aim of this integrative review of the UK literature was to ascertain the experience of PFC who have experienced or expressed their preferences regarding discussions about CPR and DNACPR decisions.
Methods
Design
We conducted an integrative review of the UK literature to summarise past empirical work and identify the scope of existing best practice.14 The aim of the project was to identify research on participant experiences of CPR decision-making conversations, which we knew encompassed diverse epistemologies and methodologies. Thus, an integrative review was chosen for its inclusivity, which enabled the analysis of studies using qualitative and quantitative designs. The six main steps are shown in box 3.
Integrative review methodology14
Identifying the search terms.
Conducting the search.
Reviewing the abstracts for relevance.
Reviewing and appraising the full texts.
Refining the research questions.
Extrapolating the themes.
Data sources
Search strategy
The research team worked in collaboration with a librarian to identify appropriate search terms. The search was then conducted by the librarian and the results fed back to the research team. Queries regarding inclusion and exclusion criteria were discussed contemporaneously throughout the search period. The search was conducted in the following databases: Medline, Health Management Information Consortium (HMIC), Embase, CINAHL, PsychInfo, Web of Science, Scopus. English language papers which were published between 1 January 2000 and 15 November 2016 were included in the search. The initial search included papers from all countries, recruiting patients from all settings (ie, hospital, community, nursing home, hospice), with all diagnoses (including frailty) and family members or caregivers. Papers focusing on health professionals’ experiences of CPR conversations were excluded, unless the paper included the views of patients and carers. The search terms can be found in box 4.
Search terms
(Cardiopulmonary Resuscitation/Do Not Resuscitate/Do Not Attempt Resuscitation/Not For Resuscitation/Do Not Attempt CardioPulmonary Resuscitation).
(‘Resuscitation orders’ ‘DNR order’ ‘Allow Natural death order’).
(‘P0LST’ (Physician Order For Life Sustaining Treatment).
(‘CPR conversations’).
(‘Patient, family carers Perceptions/perspectives on CPR discussions’).
Data evaluation
After de-duplication, a total of 773 abstracts were identified. These were divided equally between the three researchers (CH, JL, EC). Abstracts were screened for eligibility according to the following inclusion criteria: Papers were included if (1) the research was conducted in the UK, (2) written in English, (3) published between 2000 and 2016 in a peer-reviewed journal, (4) primary quantitative or qualitative research, (4) included patient and carer experiences of DNACPR/CPR discussions (hypothetical and retrospective).
Data extraction and synthesis
A flow diagram of the search results can be found in figure 1. Of the 773 abstracts identified, 20 full text articles matched the criteria for inclusion. The full text articles were collated and appraised for quality using appropriate tools from CASP,15 SIGN guidelines16 or Medscape.17 A coding system of 0–10 was applied to the papers. A score of 8–10 was considered high quality, 4–7 moderate quality and below 4 was poor quality.
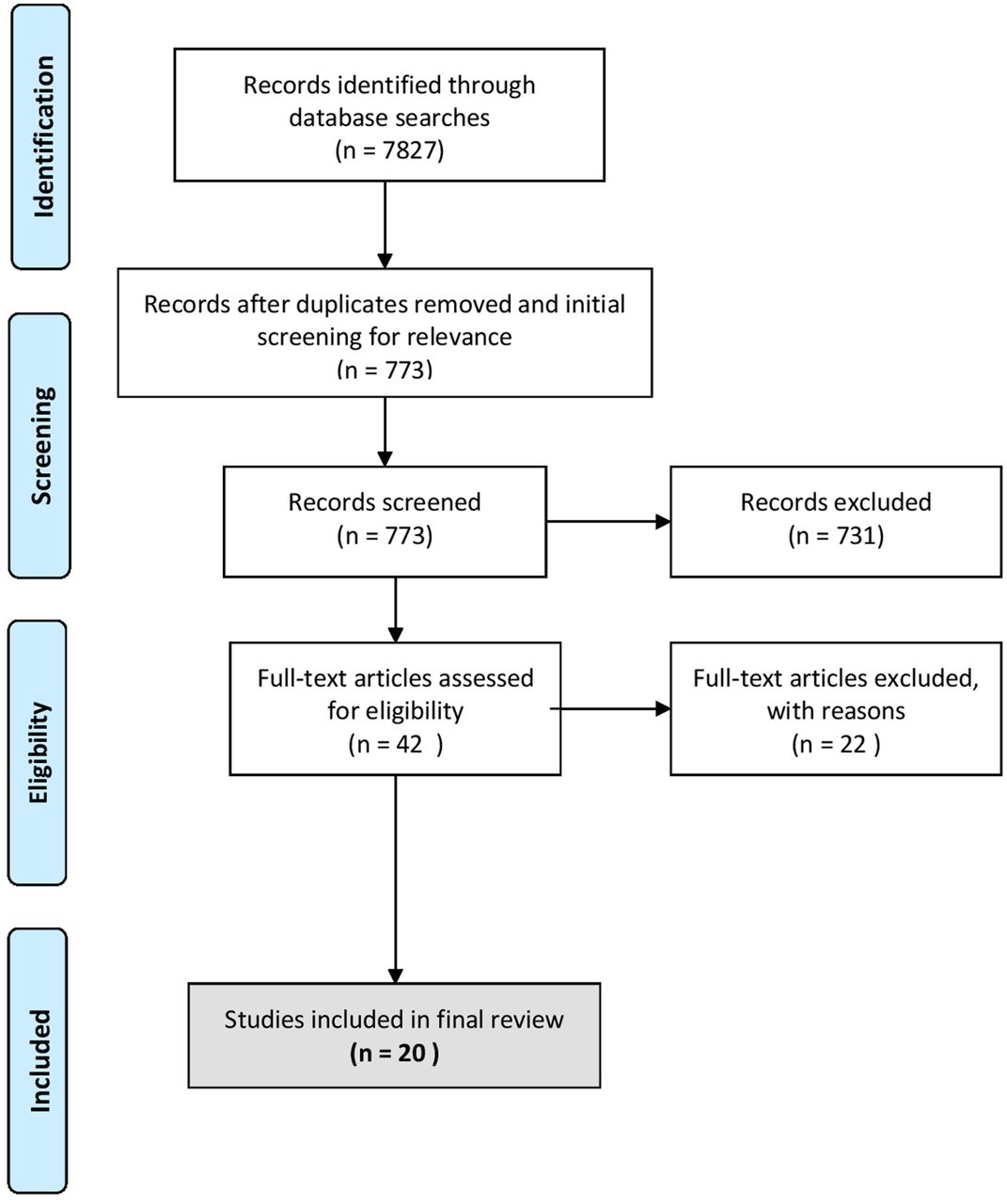
Flow diagram of the search results.
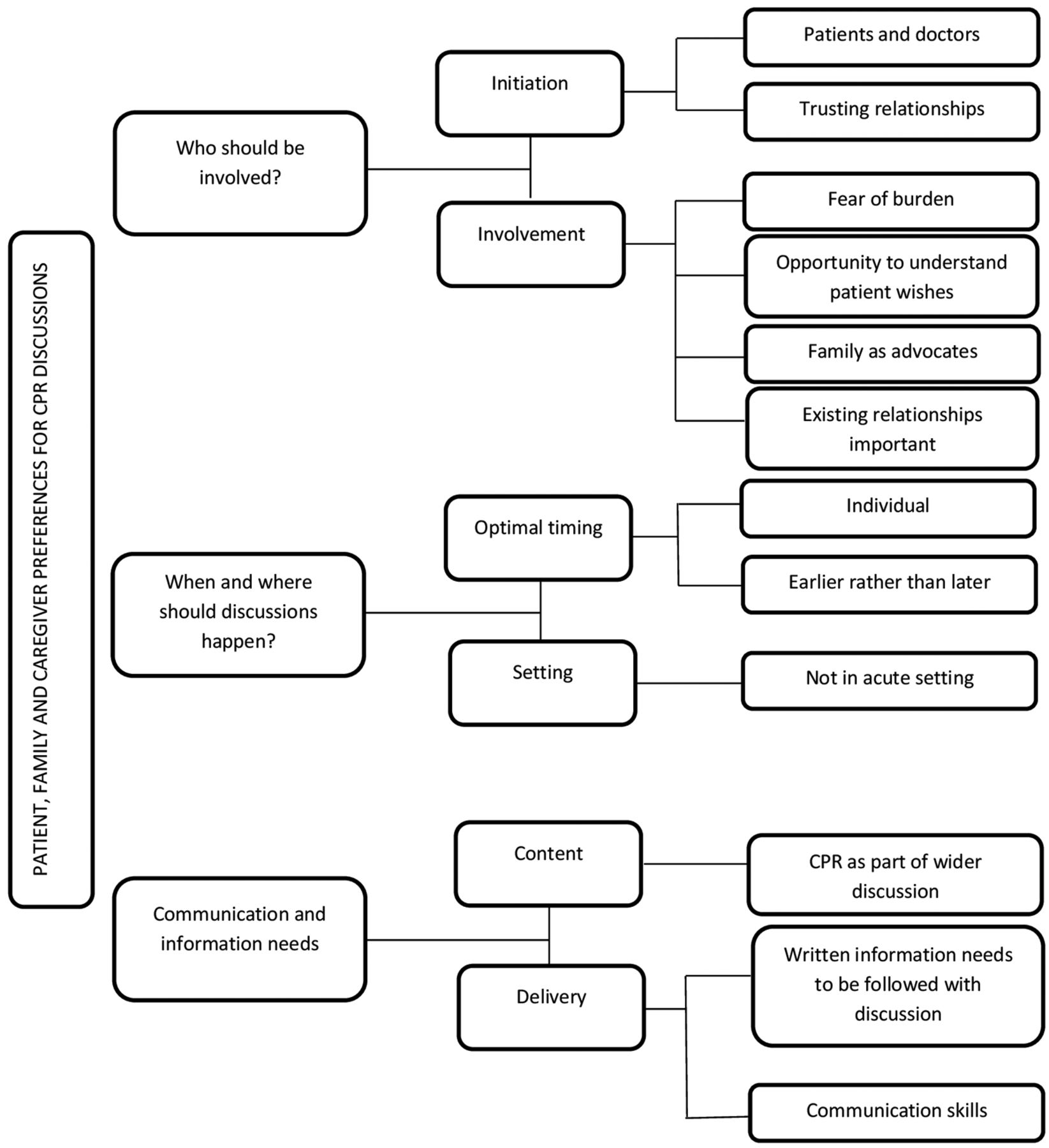
The 20 papers in the final set were read by authors EC and CH. The data extracted were: CPR-related aim, country of origin, evidence of ethical review, setting, participants, design/methods, research tools, main CPR-related findings and study limitations. Themes were identified for each article and collated in a master document. At this point, data extraction and themes were cross-checked and a detailed analysis was conducted to extract, reduce and categorise subthemes,14 using the constant comparative method18 used in qualitative research. Themes and subthemes were discussed at regular research team meetings and iteratively refined. A conceptual framework was developed (figure 2).
{kind=link}
{kind=link}
Conceptual map of the findings. CPR, cardiopulmonary resuscitation.
Results
Characteristics and quality
Twenty papers were from the UK and included in the final review. The papers are summarised in the online supplementary material. Of the 20 papers, eight were based on actual experiences of discussions as compared with nine which were hypothetical that is, what patients, family members and caregivers would want for discussions about CPR. Three studies recruited participants with and without actual experiences of discussions. A qualitative design was adopted in 13 papers; four were quantitative and three used mixed method designs. Some studies were about ACP more broadly, of which the CPR conversation is a part. The setting for 10 of the studies was in hospital, 7 in the community, 1 in hospice, 1 in a care home and 1 using a variety of settings.
Supplementary file 1
In terms of quality, 11 papers were classified as high quality and 8 were of moderate quality. No papers were classified as having poor quality. It was not possible to critically appraise one paper19 using the tools described above.
Synthesis
The main DNACPR-related findings from each paper are included in the online supplementary material. Analysis revealed themes in the following areas: (1) Involvement in discussion; (2) Optimal timing and setting; (3) Information and communication. Figure 2 presents a conceptual map of the findings.
Involvement in discussion
Who should initiate discussions?
Overall, the studies concluded that patients were willing to have a conversation about CPR or ACP and that doctors were perceived as best placed to have the discussion.20–22 Initiating the discussion was discussed in 6 of the 20 studies.23–28 Pollock et al’s 21 case studies with patients showed that both patients and health professionals can initiate conversations about ACP, but an existing relationship is required, and patients rarely do initiate these conversations.23 In addition, there was no documented ACP discussion in 9 of the 21 case studies. Pollock et al also found that it was often General Practitioners (GP) who initiated discussions.23 This is encouraging, since the findings show that patients valued having the discussion with someone they trusted, who was known to them.24–27
In Seamark et al’s (2012) study, patients with chronic obstructive pulmonary disease (COPD), who had recently been admitted to hospital for an acute exacerbation, described that a consultant or specialist nurse could initiate a discussion about CPR, but they would not necessarily have the personal relationship that the patients desired.27 Similarly, Vandrevala (2002) found that older adults living in the community, when asked about EOL decision making, felt that doctors were the right person to give a clinical diagnosis, but not necessarily to discuss sensitive issues. Reasons given for this included doctors’ non-acceptance of death as a reality, the focus on cure within Western medicine and that doctors do not want to upset them so may water down the information provided.28 Conversely, Seamark (2012) noted that patients may avoid discussions as they are seen as potentially distressing and emotional.27 Ray et al (2012) highlighted the need for health and social care workers to have advanced communication and mentoring skills to build trust and facilitate ongoing conversations around planning for death and dying.29
Who should be involved in discussions?
The participation of family at the discussions was largely viewed as positive. For example, Gorton et al (2008) showed that 87% of general outpatients would like their relatives to be involved in their decision about resuscitation status, if they were unable to hold a discussion due to critical illness.21 Likewise, Ackroyd and colleagues (2007) found that most patients with cancer in this study wanted their family involved.30 In the care home setting, an intervention to improve ACP discussions and documentation, led to relatives feeling more satisfied with EOL care and better supported.31 Older people largely assumed that family would be responsible and able for decision making if they became incapacitated and that this would increase the chances that their wishes were met.25 32 In some cases, it was described as appropriate to hold a discussion with the family alone. For example, a case note review of patients admitted to an acute ward conducted by Cohn et al, found that 30 of 43 discussions were held with relatives alone due to ‘poor comprehension’ of the patient (including confusion, delirium and dementia).20
When describing their views on Family Witnessed Resuscitation (FWR), patients felt that relatives would be able to act as advocate. Both patients who had been through a resuscitation and controls (emergency cases who had not), felt it may also benefit the family, particularly if there are concerns around the care received.33
From the point of view of relatives themselves, Higginson et al’s (2016) ethnographic study of patterns and conflicts in care and decision-making trajectories, described that families did not necessarily want to make decisions because they felt ill prepared. Decisions were easier to make when patients switched from curative to comfort care. Preferences for the level of involvement varied, but generally families wanted information and to understand the process.34 The relatives of patients with stroke in Cowey et al’s (2015) study expressed most dissatisfaction and discomfort when they were excluded from making decisions, but at the same time felt responsible for making the ‘right’ choice.35
Relatives’ involvement in discussion and decision making were often perceived as burdensome by patients. For example, Vandrevala (2002) found that patients were concerned about involving family in EOL decisions, for fear of being a burden on them—particularly when there had been no prior discussion within the family.28 Advance statements were described by PFC as a way of relieving families of the burden they may feel as a result of decision making.25 Vandrevala (2006) described that involving families in decisions about EOL care could be both a burden for relatives, or in some cases a relief, particularly if it resulted in a better understanding of the ill person’s wishes.32 Cox (2007) also reported that patients recognised that the conversations about resuscitation and EOL enabled them to discuss their wishes with their families.26
Seymour et al (2004) noted that families and patient’s decisions were made in the context of their relationships—particularly as patients thought about how their families would be feeling and behaving when they were at EOL.25 Vandrevala (2006) also noted that deciding who should specifically be involved in the discussion was based on personal circumstances.32 Seamark et al (2012) described that participants with severe COPD imagined that EOL discussions would involve their family and that these discussions would be beneficial, but joint interviews with spouse and patient revealed differing agendas about the future.27 Livingston (2010) and McMahon-Parkes (2009) also noted that although consulting with families could be helpful, difficulties arose when there were disagreements or conflicts of interests.33 36
When and where
Optimal timing
There was overall consensus across the papers that advance CPR decisions should be discussed with all patients,21 22 but optimal timing was dependent on the individual.26 There was variance around when in the illness trajectory discussions should take place. Gorton et al (2008) found that of the 364 patients who completed a questionnaire about attitudes towards DNAR discussions, 14% would like to have the discussion after they became critically unwell, 33% during an outpatient clinic appointment, 37% on admission to hospital and 16% before surgery.21 Albarran et al (2009) also suggested that patients should be asked about FWR on admission to hospital.37 Johnson et al (2008) suggested that distributing a leaflet about DNACPR during the first admission or day care visit to the hospice was appropriate, but had to be followed up with a discussion.24 Cox et al (2007) also highlighted the importance of postdiscussion support, particularly when discussions had been distressing.26
There was agreement, particularly in more recent studies, that discussions should not be conducted during an acute admission to hospital23 25 27 28 30 or at diagnosis.26 However, they should occur earlier in the illness trajectory rather than later.27 29 For example, Ray et al (2012) suggests that EOL discussions for patients with motor neuron disease (MND) need to begin early in the disease progression and continue throughout the course of the disease. In this way, discussions can enable people with MND and their family members to reconstruct normality, to include dying as part of life and enable the development of a sense of control over care in an uncontrollable disease.29 Seymour et al (2004) suggested that discussions should not take place too close to death,25 but Pollock et al’s (2015) case studies revealed that this frequently happened. Reasons included lack of opportunity to have a discussion earlier and issues around communication. Pollock et al (2015) described a case, where, despite the presence of long term illness, DNACPR was completed 3 days before death. This is because the patient did not want to engage in ACP when he was well, despite efforts made by professionals.23
Two studies noted the potential vulnerability of patients at EOL. Seymour found that patients worried about making the ‘wrong’ decision if they responded when they were ill. Ackroyd et al (2007) suggested that as a result of being ill and vulnerable, discussions about CPR need to be handled sensitively and important information may not be well received or understood when discussed during admission.25 30 This is supported by Cox et al (2007) who reported that discussions should be conducted when patients are feeling well, so they can take in the information and act on it.26 Seamark et al (2012) found that patients with COPD were usually admitted with an acute exacerbation, which limited the opportunity for discussion about EOL.27 Further to that, relatives and patients may be at different points in the process and thus have different needs.38
Setting
Only two papers mentioned the optimal setting for the discussion. Seamark et al (2012) suggested that discussions were best conducted by the GP, in the surgery, in the time period after acute admission.27 Similarly, Cox et al (2007) found that there were fewer negative comments about conversations when they had taken place in the outpatient department as compared with the ward—which was perceived as too public.26
Information and communication
Delivery and content
Discussions should be individualised,24 26 34 empathetic, honest, straightforward and balanced.26 The use of vague language was found to be frustrating for patients in Pollock et al’s study.23 Good communication skills and consideration of the levels of education and literacy are required.29 34
Conversations should aim to deliver information on risks involved in CPR and the low chances of success24 and should aim to elicit patient preferences and goals, as opposed to process decisions about care.34 This should include gaining a shared understanding between clinician and PFC of prognosis and quality of life—which was seen as a key factor in the decision making process.32 36
Fritz et al (2015) and Obolensky et al (2010) both support a move from away from the DNACPR form to consider treatment more generally as is illustrated in Fritz et al’s paper about the development of the Universal Form for Treatment Options (UFTO)—a two-page form which is universal, simple, contains guidance about treatment options, resuscitation decision and has the potential for patients’ wishes to be incorporated.19 Patients in Obolensky et al’s (2010) study found discussing a ‘Treatment Escalation Plan’ (TEP) caused no excess anxiety and patients reported feeling ‘looked after’ ‘reassured’, and it enabled them to ‘to face reality’ and ‘put things in to perspective’.39
The delivery of information in a written format (leaflet) was not considered useful in a study with relatives of patients with a stroke. In fact, relatives reported seeking information in other ways.35 Likewise, Johnson et al (2008) found that a leaflet on DNACPR policy was not effective in isolation and had to be followed up by a discussion, but it was acceptable to patients in the context of their illness understanding.24
Discussion
The results of this review identified that there is a lack of empirical research on the preferences of PFC regarding discussions around DNACPR. The findings show that some preferences of PFC are at odds with the guidance and statutory decision-making frameworks which guide clinicians in the UK. For example, there is a desire by PFC for discussions about CPR to be held by someone with whom they have a strong or established and trusting relationship. In several papers, this was the GP.23–27 However, by law it is now a necessity to discuss DNACPR decisions at the earliest practicable and appropriate opportunity, meaning that more and more discussions about CPR are being held with patients at, or soon after the point of acute admission to hospital, by doctors the patients are unlikely to have ever met. Although many DNACPR discussions are held in the community, it is unrealistic to expect every discussion to be held by a patient’s ‘known/trusted’ GP. The very nature of the decision-making process is that these discussions are often triggered by an acute deterioration, followed by an admission to hospital. Not every disease trajectory allows for a predictable deterioration and clearly signposted opportunities for ACP discussions; however, work is ongoing to clarify best approaches for each trajectory.40 The literature highlighted that for most illness trajectories, an earlier discussion was preferable than later, and leaving discussions too close to death is suboptimal.
These PFC views add important evidence to the clinical opinion that there are potential opportunities for discussions about future care preferences which are being missed.41 42 There is evidence in the literature that PFC advocate a move towards CPR discussions becoming part of a wider discussion about realistic care and treatment options that includes a patient’s broader life values and goals of care. PFC prefer these discussions to be held in non-acute or outpatient/community settings, by someone known, when the person is more ‘well’ and less ‘vulnerable’. This finding would support the implementation of recognisable processes which can be used to facilitate such discussions in any care setting (eg, ReSPECT process http://www.respectprocess.org.uk). Such initiatives encourage specialists and generalist services to structure outpatient clinics to enable and facilitate discussion about future preferences for care as a core part of their review process.42 43 Electronic palliative care summaries may facilitate communication between specialist and generalist services and sensitive communication with patients on admission to hospital.44
Adequately resourced advanced communication skills education, for all generalist and specialist clinicians with opportunity to support these discussions, is a necessity. The fact that some PFC feel doctors are not always the best people to discuss sensitive issues with, should encourage and empower nurses and Allied Health Professionals (AHPs) in care homes and the community, to take forward these discussions with their patients. Community teams could use this evidence in support of proactively following up patients after discharge home following acute admissions, as described by Seamark et al (2012).27
As well as revealing some significant differences between PFC views and current practice, the findings also provide a rich opportunity for educators, policy makers and healthcare professionals to try to find ways of bridging some of these gaps between expectation, resource and reality. Table 1 summarises the opportunities and challenges of bridging such PFC expectations. We have provided suggestions for incorporating our findings in to practice and how the shape of future care in the UK might change. Undoubtedly incorporating change within a healthcare system with limited resources will create challenges both for primary and secondary care teams, but a deeper understanding of why change is happening and the potential benefits in terms of person-centred care is often helpful.45 Quality Improvement Methodology including the Plan, Do, Study, Act (PDSA) model for improvement is a fast and effective way of introducing change and is strongly advocated for use within the NHS.44 46
Bridging some of the expectations: challenges and opportunities
The Chief Medical Officer for Scotland set out her vision for the future of healthcare in her report Realistic Medicine, that we need to find ways to encourage clinicians to put the person receiving healthcare at the centre of the decision-making process and create a personalised approach to their care.47 The PFC experiences presented in the this review, along with the opportunities and challenges they present, must shape the way we manage these potentially challenging discussions in the future. Patient and family experience of ACP discussions should be evaluated alongside the introduction of any regional or national ACP process, to inform best practice approaches to communication.
Strengths and limitations
International papers were excluded due to the specific nature of the legal and statutory framework for discussing DNACPR in the UK, as outlined in the introduction to this paper. In so doing, findings from those studies may have been missed. Of the 20 papers included in the final review, nine papers were on hypothetical views about CPR decision making as opposed to actual experiences. This highlights the need for prospective primary research with patients and their families who have been involved in discussions about ACP and DNACPR. The studies were conducted in a variety of community and hospital settings which is a strength. However, only one study recruited participants from a care home which is a limitation. There was also good representation from patients and families. In terms of study design, there were no randomised control trials and only one case-control study which is a limitation. The qualitative papers exhibited a good range of methods, including ethnographic observation in one study, but often the number of participants was small and therefore the result not immediately generalisable.
Conclusion
The findings from this integrative review of the literature on PFC experience of CPR decision-making discussions are at odds with the current legal state in the UK and are potentially challenging for health professionals, who are required to discuss DNACPR decisions at the earliest opportunity. The educational elements needed are comprehensive, for example, advanced communication skills training, which commences in undergraduate training, and extends to higher specialist medical training, as well as ongoing training and regular review at consultant level. There is also evidence to suggest that the empowerment and extension of the role of nurses and AHPs is necessary to meet the preferences of PFC, particularly around initiating discussions about future care needs and wishes and planning future care. The views of these UK PFC should form a critical part of the evidence base for the person-centred approaches of future care planning policies, both at local and national levels. For healthcare to genuinely move towards a ‘realistic medicine’ approach, we need to acknowledge and balance the wishes and experiences of patients with the resources, legalities and processes of our healthcare system.
Acknowledgments
The authors would like to acknowledge the work of Alison Bogle, Health Management Library, National Services Scotland. Thanks to Dr Beci Evans who was involved in extracting data from a subset of papers.
References
Footnotes
Contributors CCH, EC, JAS and JL designed the project. CCH, JL and EC reviewed the abstracts and extracted data from the papers. EC and CCH reviewed the papers for quality. EC and CCH drafted the final manuscript. All authors approved the final draft.
Funding Funding for the project was received from the Scottish Government. The posts of JAS and EC are supported by Marie Curie.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no unpublished data.