Article Text

Abstract
Introduction Despite preferences to the contrary, 53% of deaths in England occur in hospital. Difficulties in managing clinical uncertainty can result in delayed recognition that a person may be approaching the end of life, and a failure to address his/her preferences. Planning and shared decision-making for hospital patients need to improve where an underlying condition responds poorly to acute medical treatment and there is a risk of dying in the next 1–2 months. This paper suggests an approach to improve this care.
Intervention A care bundle (the AMBER care bundle) was designed by a multiprofessional development team, which included service users, utilising the model for improvement following an initial scoping exercise. The care bundle includes two identification questions, four subsequent time restricted actions and systematic daily follow-up.
Clinical impact This paper describes the development and implementation of a care bundle. From August 2011 to July 2012, 638 patients received care supported by the AMBER care bundle. In total 42.8% died in hospital and a further 14.5% were readmitted as emergencies within 30 days of discharge. Clinical outcome measures are in development.
Conclusions It has been possible to develop a care bundle addressing a complex area of care which can be a lever for cultural change. The implementation of the AMBER care bundle has the potential to improve care of clinically uncertain hospital patients who may be approaching the end of life by supporting their recognition and prompting discussion of their preferences. Outcomes associated with its use are currently being formally evaluated.
- Clinical decisions
- Transitional care
- Communication
- Hospital care
- Cultural issues
- Education and training
Statistics from Altmetric.com
Introduction
There is increasing recognition of the challenges experienced by patients, their families and professional caregivers when admitted to hospital with an acute exacerbation of an underlying life-limiting condition, frequently facing an uncertain outcome. Acute hospital treatment tends to focus on the immediate clinical problem with less effective case management such as recognition of transitions between clinical phases.1 A structured approach to intrateam consensus is rarely evident, and prognosis is often not discussed with patients.2 Particular difficulties are associated with the heterogeneous presentation of clinical uncertainty—the spectrum ranges from those patients with more predictable progressive disease (typically advanced cancer), to those with a less predictable course sometimes characterised by episodic acute deterioration (typified by frail older patients). The result can be delayed recognition that a patient may be approaching the end of life, and a consequent failure to provide high-quality care and convey information that gives the opportunity to focus on patient choice in the face of uncertainty and possible approaching death.3
In England, currently 53% of all deaths occur in hospital,4 despite research suggesting that most people would prefer to die at home.5 On average, 29.7 days are spent in hospital in the last year of life with repeated hospitalisations which can be a cause of distress among patients and their families. Recent reports have suggested that only 25–42% of deaths in England and Wales are unexpected.6 Moreover, a retrospective casenote review of 599 hospital deaths identified that 44% were either clearly in the last year of life, or could probably have been recognised as such and that 20–33% could have been cared for at home if excellent end-of-life care services were in place.7 It is recognised that practical considerations such as care provision at home are crucial to making this achievable and also that dying at home is by no means a universal preference. Offering patients and their families the opportunity to consider options and exercise some choice over place of care, however, is an increasing priority. There is a need for systems and training which support earlier recognition of such deteriorating patients to facilitate better communication and planning.
One of the key challenges in this area of care is the need to communicate and plan in the context of a clinical situation which may improve or may deteriorate further. This planning may include aggressive medical therapies alongside discussions about preferences for care should these not be effective. This integration of traditionally ‘active’ and ‘palliative’ approaches can lead to discord within a team and suboptimal sharing of decision-making with patients. This is now being more widely recognised with evidence accumulating through patient safety literature of the need for appropriate decision-making around ceilings of care, appropriateness of attempting cardiopulmonary resuscitation and a review of overall goals of care.8 ,9
This care planning can be complex and must be individualised. It does not simply involve de-escalation of care but must recognise when it is appropriate—according to patient wishes and clinical context—to escalate care (at a general ward level or to high dependency or intensive care units) for specific clinical situations despite underlying life-limiting diagnoses. It is no more appropriate to rule out than it is to pursue aggressive medical care without considering the overall goals of care.
In this paper we describe the design, development and implementation of an innovative care bundle, ‘the AMBER care bundle’, to improve the care for patients, in the acute hospital setting, who may be in the last 1–2 months of life and whose potential for recovery is uncertain.
What is the AMBER care bundle?
A care bundle is a set of evidence-based, or self-evident good-practice-based interventions for a defined patient population and care setting.10 It will typically consist of a small number of interventions (normally 4–5), which when implemented together, are associated with improvements in clinical outcomes11 ,12 as well as reliability, consistency and measurability of treatment. Care bundles have an inherent focus on teamwork and intrateam communication. Thus, they support consistency in structure (through agreement on a cluster of interventions) and in process (by agreement within the local team on which individual is responsible for which task and at what time point). They aim to ensure that all patients in the specific population receive the best care each time.
Scoping and development
Guy's and St Thomas’ NHS Foundation Trust has 700 adult general hospital (level 1) beds and treats approximately 110 000 adult inpatients per year. It provides both local general hospital services and specialist services in South London including for cancer care, renal medicine and cardiovascular disease. In 2010, the development period of the AMBER care bundle, 1059 adult patients died in the hospital: 49% in adult acute medical specialties (mainly general and geriatric medicine), 13% in oncology and 28% in critical care and intensive care beds for a wider population. The palliative care service is well integrated into the acute inpatient services.
The AMBER care bundle was developed by a multiprofessional team involving those from Geriatric Medicine, Palliative Care and an Improvement Science background. In addition, an extended team of clinical and non-clinical community and hospital staff as well as service users were actively involved.
The process involved the following. First, a scoping exercise to identify clinical management and healthcare system issues around patient care towards the end of life. A retrospective casenote review was carried out on a cohort of consecutive adult inpatient deaths (N=14). This review demonstrated issues around:
-
Delayed recognition of end-of-life care needs.
-
Variable involvement of patient and family in planning and decision-making.
-
Inconsistent management of clinical uncertainty/when potential for recovery is uncertain.
-
Suboptimal team work and decision-making, particularly regarding escalation of type or place of care.
The team was then tasked with developing a tool that could be swiftly and consistently understood and implemented by clinical staff. We recognised that such a tool must fit within existing ward practices and culture in order to produce benefits meaningful to patients. We also put at the heart of our development work the principle of minimising variability in care and enhancing consistency and transparency.
The decision was made to develop a care bundle to address the needs of this vulnerable and clinically challenging population. It was named ‘The AMBER care bundle’ to reflect the need to stop and reassess the patient's needs at a time of clinical uncertainty. AMBER stands for:
-
Assessment
-
Management
-
Best practice
-
Engagement (with patient and carer) for the
-
Recovery uncertain patient.
The AMBER care bundle provides a systematic approach to managing the care of hospital patients who are facing an uncertain recovery and who are at risk of dying in the next 1–2 months—but who are not clearly in the last few days of life—and for whom active medical management may still be appropriate. It is an intervention that can fit within any care pathway or diagnostic group for patients whose recovery is uncertain (see figure 1).
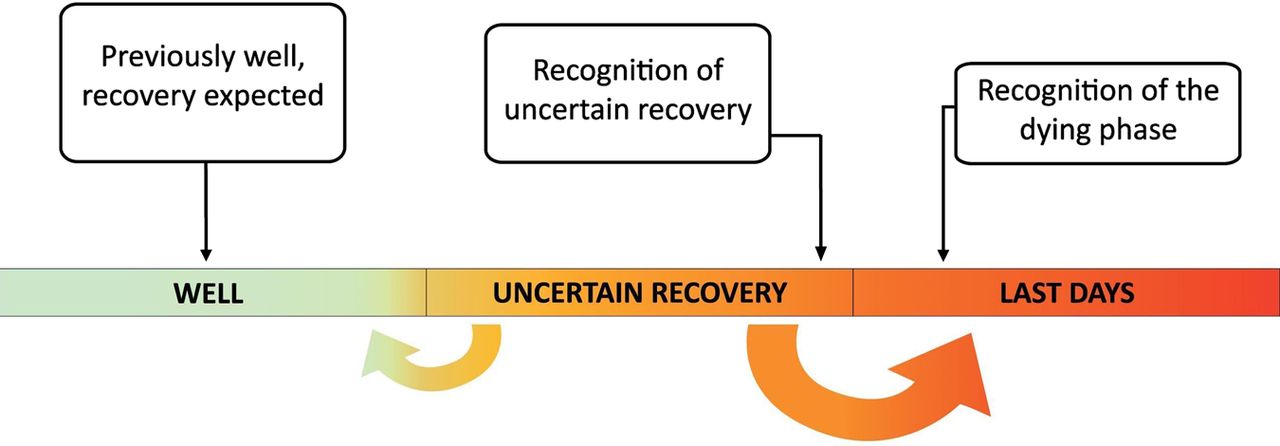
Identifying patients whose recovery is uncertain.
In order to develop the components of the AMBER care bundle, ‘Plan Do Study Act’ (PDSA) testing cycles of change outlined in the model for improvement were adopted.13 This process encourages the implementation of changes initially on a small scale, towards a specific aim, incorporating a process of planning, change, observation and modification where necessary. These cycles are repeated until the desired aim is achieved. Our aim in this case was the development of a maximum-5-component care bundle which incorporates the care elements deemed essential for this cohort of patients, which could be built into ward processes and is acceptable to the staff.
Identification questions
Identification questions were specifically designed for the AMBER care bundle to enable a simple algorithmic implementation. Exploration regarding these questions was conducted in order to ensure that terms were commonly understood and were free of any ambiguity across multiple clinical settings.14 Early trials using a modified ‘surprise question’ (would you be surprised if this patient died within the next 1–2 months?) were not successful. Staff reported both confusion and discomfort with the term ‘surprise’, preferring what they viewed as more objective clinical terminology related to risk.
Throughout testing and in later implementation, it was emphasised that the intention is to identify a patient cohort at risk and most likely to benefit from this intervention. It is not intended as a prognostic tool.
After further cycles, using the PDSA model, two identification questions were selected and were found to be clinically relevant and easy to use:
-
1. Is the patient deteriorating, clinically unstable and with limited reversibility?
-
2. Is the patient at risk of dying within the next 1–2 months?
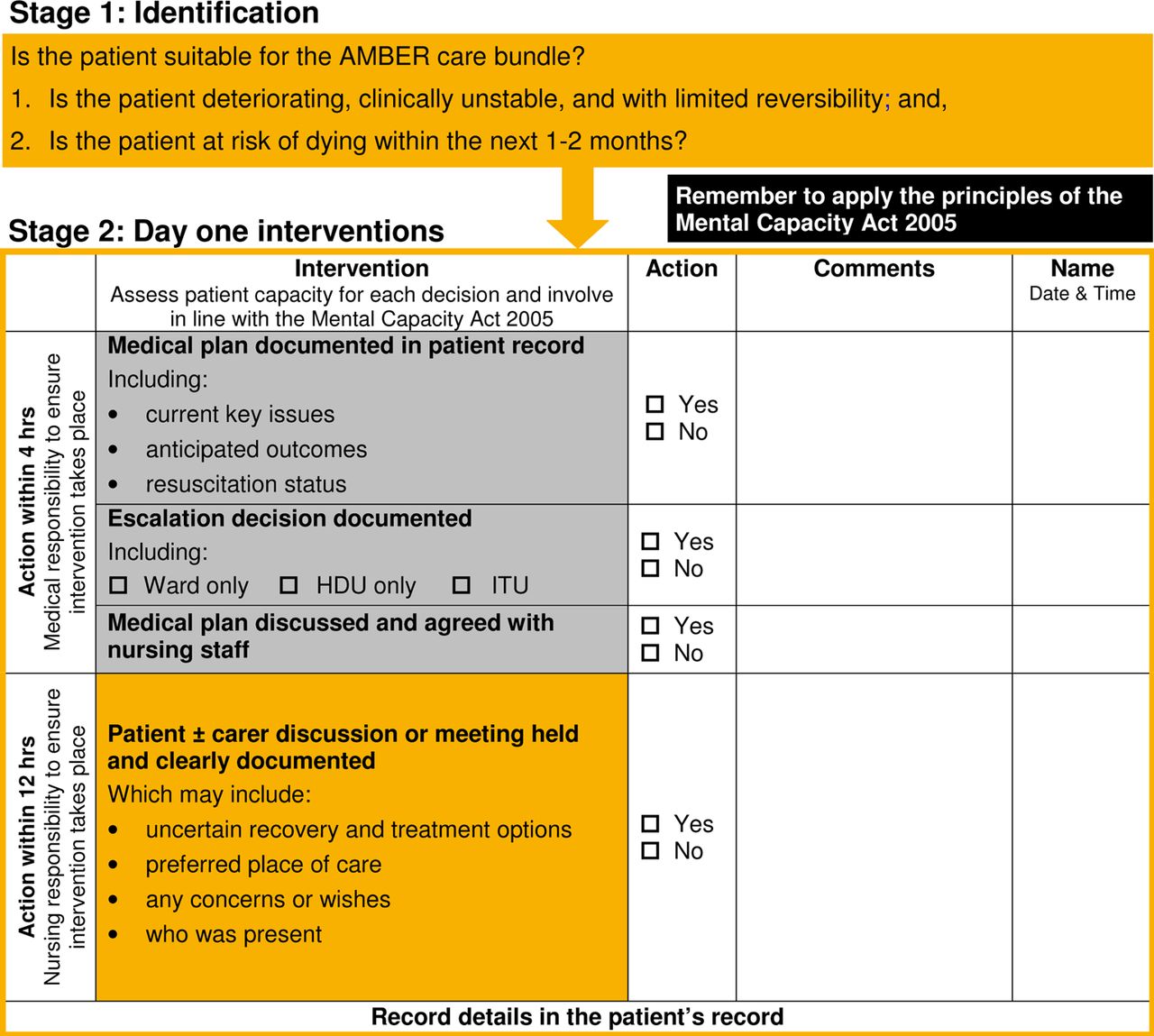
If the answer is ‘yes’ to both questions, the patient is suitable for care supported by the AMBER care bundle (see figure 2). Any member of the multidisciplinary team can raise a concern, but there must be agreement from the medical and nursing teams that care supported by the AMBER care bundle is appropriate that is, the patient's condition and progress are such that the criteria are met.
{kind=link}
{kind=link}
The AMBER care bundle (V.3, 2012)—stages 1 and 2.
Interventions supported by the AMBER care bundle
An initial long list of interventions was refined to four questions that could be easily answered in ‘yes’ or ‘no’ in an acute care setting. These comprised:
-
1. Is the medical plan documented in the patient records (including current key issues, anticipated outcomes, resuscitation status)?
-
2. Is an escalation decision documented (ward only, high dependency, intensive care)?
-
3. Has the medical plan been discussed and agreed with nursing staff?
-
4. Has a patient±carer discussion or meeting been held and clearly documented?
The apparent simplicity of this list of interventions reflects the importance of the early testing work, distilling out the core tasks felt to impact on patient experience and improve consistency and patient-centred teamwork.
In order to ensure a prompt initial response, a timeline in which to complete these actions was added of 4 h for questions 1, 2 and 3 and 12 h for question 4. An AMBER care bundle proforma was developed to be completed and inserted into the patient's notes (see figure 2).
Ongoing daily monitoring—stage 3
The need for daily review of the patients’ status and appropriateness for the AMBER care bundle was identified as a result of feedback from patients and families. The proforma therefore reminds the multidisciplinary team to ACT daily:
-
A: Is the patient still ‘AMBER’?
-
C: Has the medical plan Changed?
-
T: Touch base with the patient and relatives—is everything ok?
The AMBER care bundle ACT stickers were developed and are inserted into patients’ casenotes daily when the review takes place. These stickers allow for quick and easy recognition of consistent and complete implementation of the care bundle for each patient.
A prompt to review the patient’s preferred place of care—a dynamic variable15—is built into this daily ACT review.
Stopping the AMBER care bundle—stage 4
Importantly, four possible reasons to stop the AMBER care bundle were identified, including:
-
1. Patient recovers.
-
2. Patient is discharged from hospital or transferred to a clinical area unfamiliar with its use. In either case, handover of key clinical information and plans is expected.
-
3. End-of-life care plan for the last hours or days of life is developed.
-
4. Patient dies.
Implementation
‘Implementing a bundle with high reliability requires redesign of work processes, communication and infrastructure, along with sustained measurement and vigilance’.10 The AMBER care bundle was developed in 2010 on one geriatric medicine and two oncology wards, and, once finalised, extended to two further wards (Head and Neck Surgery, and Acute Medical Admissions). Implementation was facilitated by ward based and formal teaching, using supportive guidelines and documentation, on each of the wards to teach the foundations and rationale behind the care bundle. A ‘see one, do one’ approach was also facilitated by senior nurses in order to embed a common understanding and practice into the daily routine of the ward for all staff. This was backed up by ward-based support with difficult conversations and communication skills. The care bundle returns were assessed during the development phase and administrative and management practices adapted using the PDSA approach in order to maximise fidelity and ensure consistent implementation. By July 2012, the AMBER care bundle was in use in 17 wards across the hospital.
Impact on clinical service
Between 1 August 2011 and 31 July 2012, 638 patients (mean (SD) age of 73 (16) years) were supported by the AMBER care bundle for a median of 7 days during their inpatient stay. Table 1 describes the proportions discharged from hospital, dying in hospital while still receiving active medical care and dying in hospital having been recognised to be irreversibly dying.
Outcomes for patients whose care was supported by the AMBER care bundle—discharged or died between 1 August 2011 and 31 July 2012
Of the 638 patients supported by the AMBER care bundle, 365 (57.2%) were discharged from hospital and 53 of these (14.5%) had an unplanned readmission within 30 days of discharge. Two hundred and seventy-five of these discharged patients (75.3%) died within 100 days of discharge. As patients supported by the AMBER care bundle are only tracked for 100 days post discharge, the ultimate outcome for those 90 patients (24.7%) who survived longer than 100 days is not recorded (see table 2).
Readmission and 100-day survival for patients discharged from hospital whose care was supported by the AMBER care bundle—discharged between 1 August 2011 and 31 July 2012
Of the 275 patients who died within 100 days of discharge, the place of death was identified for 196 (71.3%) patients as outlined in table 3.
Place of death for patients who died within 100 days of discharge
Table 4 (below) shows the 30-day emergency readmission rates for patients who died within 100 days of discharge, comparing those whose care was supported by the AMBER care bundle to those receiving standard care from the same wards. This comparison includes only the 17 wards on which the AMBER care bundle was implemented and excludes seven patients who were transferred to a clinical area where it was not in use.
Readmission rates for those who died within 100 days of discharge from inpatient spells between 1 August 2011 and 31 July 2012
The 95% CI for the difference between these percentages is −29.1% to −18.8% indicating significantly fewer readmissions.
Discussion
Improving care for people facing clinical uncertainty in the acute hospital setting has specific challenges.2 The recent report ‘More Care, Less Pathway: a review of the Liverpool Care Pathway’ has highlighted many of these and emphasised the need for an individualised approach to patient care.16 The public inquiry into the Mid-Staffordshire NHS Trust17 also highlights the need for effective teamwork and regular interaction between staff and patients and those close to them.
The AMBER care bundle was developed to address the needs of those whose potential for recovery is uncertain in the acute hospital setting. It is not designed to replace the LCP or any form of individualised end-of-life care planning for the last hours or days of life. The care bundle is rather designed for use alongside acute medical care across a range of specialties. Dealing with uncertainty and enabling a palliative care approach to work in parallel with active medical treatment represents a significant cultural challenge in this setting.
The focus for improvement was to ensure the recognition and timely response to a cohort of patients in the acute hospital setting who may be approaching the last 1–2 months of life. The care bundle prompts the team to ‘stop’ and review, driving better teamwork between healthcare professionals and involvement of patients and those close to them in shared decision-making and individualised care-planning. This should include preferences regarding place of care but be driven by holistic attention to what is important to the patient including attention to symptom control and emotional and family support.
The components of a care bundle should be broadly applicable to the full population for which it is developed. The use of overarching clinical prompts (medical plan, escalation and de-escalation plans, multidisciplinary team agreement, patient and carer discussion and systematic daily follow-up of preferences and clinical status) supports reliable completion of these key steps. Each of these is important within this patient cohort and, together, they underpin an individualised approach to shared decision-making and care planning.
Although simple in concept and design, continued efforts must be made to ensure the AMBER care bundle is, and remains, embedded in ward practice. Staff support with communication skills (of varying levels) as well as with reliable implementation of the processes is crucial. A programme of education and training will continue to address staff turnover, and to maintain confidence, maximise fidelity and ensure consistent implementation of the care bundle.
Next steps
The AMBER care bundle has been adopted as a key enabler in the Transform Programme to improve end-of-life care in acute hospitals18 in England and is being implemented in a cohort of hospitals nationally. While encouraging, our findings are uncontrolled and from a single teaching hospital site in which the care bundle was developed.
There is a need for robust prospective evaluation of the impact of the care bundle as recently emphasised by Currow and Higginson.19 To this end, a feasibility study examining the methodology to evaluate the AMBER care bundle has been conducted, using an embedded mixed methods design with a case–control approach. This study will complement the clinical descriptors by comparing the experience of patients receiving care supported by the AMBER care bundle and those receiving standard care. The study utilised a postbereavement retrospective follow back survey in conjunction with interviews with staff, patients and family. It will be reported in 2014 and its results will be used to inform the design of a larger evaluation.
Acknowledgments
The authors thank and acknowledge the following for their guidance in the development of the AMBER care bundle: Jayne Chidgey-Clark, previous Director of the Modernisation Initiative in End of Life Care; Roger Resar, Institute for Healthcare Improvement; Anita Hayes and Claire Henry, the former National End of Life Care Programme.
Footnotes
-
Contributors IC, AH, SS, MM and LB were involved in original development of the AMBER care bundle. MM, CR, LB, MG, KC, SS, IC and AH were involved in testing, data collection and analysis. IC, KB, SS, JK, RC, KC and AH were involved in original article design and content. IC, SS, KB, JK, MM, LB, CR, RC, MG, KC and AH took part in revising the article.
-
Funding This work was funded through a programme grant from the Guy's & St Thomas’ Charity.
-
Competing interests None.
-
Ethics approval Development and testing of the AMBER care bundle formed part of a service improvement work stream and did not require submission to a research ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Additional unpublished data are available from Dr Irene Carey: irene.carey@gstt.nhs.uk.