Article Text

Abstract
Experience-based design, co-design, and experience-based co-design can be used within healthcare to design services that improve the patient, carer and staff experience of the services. As palliative and end-of-life care centrally value person-centred care, we believe that service designers, commissioners and those tasked with making quality improvements will be interested in this growing field. This paper outlines these approaches—with a particular emphasis on experience-based co-design—and describes how they are and can be used within palliative and end-of-life care. Based on a rapid review and several case studies, this article highlights the key lessons learnt from previous projects using these approaches and discusses areas for improvement in current reporting of service design projects.
- experience
- co-design
- palliative care
- quality improvement
Statistics from Altmetric.com
Introduction
Experience-based design (EBD) and co-design (CD) methods have relatively recently been adopted within healthcare services from corporate and market research. The Department of Health places patient experience at the core of the National Health Service (NHS)1 and these methods draw on patients', carers' and providers' experiences to make changes in service design and delivery.2 As endorsed by the NHS and other health departments globally, EBD and CD are typically employed as a form of quality improvement.3 In the UK, this has been specifically adapted into experience based co-design (EBCD), which draws on the richness of patients' narratives to focus improvements on key ‘touchpoints’ within the wider experiential journey of using healthcare services.2
Both palliative care and EBCD seek to be patient-centred in their approach, focusing on the patients experience and viewing patients as shared decision-makers. Within palliative and end-of-life care, the experience of the patient and carers is an important quality marker of care.4 Examples of their experience often tell of contact with a complex and bewildering system, which can exacerbate their illness experience and bereavement.5 The experience of professionals is also important, recognising the importance of reflective practice and risk of emotional burnout.6
Owing to their similar starting points—that patients journeys and voices matter—one would expect experience-based methods to be widely used within palliative care service design. Despite the steady growth and evaluation of end-of-life care service provision since the 2008 End of Life Care Strategy,4 our recent rapid review of the academic and grey literature revealed few examples to date.7
Drawing on this review and several case studies, this article describes what EBD and CD approaches, including EBCD, and how they can be used in the development of palliative and end-of-life care services.
Introduction to the methodology
The field of EBD and CD is evolving and interdisciplinary. While the terminology used varies across sources, they share a core methodological approach that is concerned with, and may involve, the experiences of patients (and others) as healthcare service users. Box 1 highlights some of the key potential benefits of using these methods.
Why you might consider using these methods
Engage and empower service users and healthcare professionals;
Create services that seek to improve experiences of care;
Identify issues in systems that may not be readily apparent;
Complimentary with other service improvement methods.
These approaches have been used for around 20 years in industry, being taken up within healthcare in the UK over the past 10–15 years2 ,8 with the development of toolkits to aid service design (see box 2). In particular, EBCD has been designed with healthcare services in mind, and has been used in over 80 healthcare projects worldwide.3
Where you can learn more
King's Fund. Experience-based co-design toolkit. 2012. Available at: http://www.kingsfund.org.uk/projects/point-care/ebcd.
NHS Institute for Innovation and Improvement. The ebd approach: experience-based design. 2009. Available at: http://www.institute.nhs.uk/quality_and_value/experienced_based_design/the_ebd_approach_%28experience_based_design%29.html.
Health Service Co-Design by Waitemata District Health Board, New Zealand. Available at: http://www.healthcodesign.org.nz/about.html.
Experience Led Commissioning: Introduction to ELC in end-of-life care. Available at: http://www.experienceledcare.co.uk/docs/Introduction_to_ELC_in_end_of_life_care_1010.pdf.
Robert et al.18
Healthtalk online national video archive: http://www.healthtalk.org/.
EBD describes a collection of methods that seek to draw on patient/user/customer experiences to inform the design process of services and products. As well as designing for performance and reliability, this approach focuses on the aesthetics of experience—what and how it feels like to use or be part of the service.2 In addition to drawing on people's experiences, CD brings together designers and users (patients and carers in the healthcare context) to collaboratively identify problems and possible solutions. The extent of user participation may vary from public consultation to active co-creation. CD methods can be used alongside other quality improvement methodologies such as Lean and Six Sigma.9 Within healthcare, the use of EBD and CD are examples of drawing on design theory and methods to address the need for service innovation and quality improvement.
EBCD seeks to combine the focus on experience with the participatory elements of CD to generate service innovation that reflects how people understand and engage with services. Within the NHS, the method was originally called ‘EBD’ but was rebranded to highlight the importance of partnership and collaboration in identifying issues and solutions.3 EBCD draws on four core theoretical positions, embodied in its commitment to change, collaboration, reflection and the use of personal stories. These are (1) participatory action and practice-based research methods, (2) user-centred design, (3) the learning/reflective cycle, and (4) narratives as resources.8 EBCD is similar to other participatory-based approaches in so far that it focuses on engaging a variety of stakeholders to collaborate, but views itself as distinct in its focus on experience as a motivator for change.2 This is done primarily through the use of narratives to provide a way for care providers (eg, nurses, doctors, commissioners) to emotionally connect with patients' experiences and reflect on potential service improvements.10 Designed primarily for the healthcare market, EBCD aims to generate quality improvement and to exceed patients' and carers' current experiences of healthcare services.
Overview of the EBCD method
As a quality improvement exercise, the focus is on capturing, understanding and improving experiences and measuring the improvement in services. Ideally, EBCD uses ethnographic methods such as in-depth interviews, participant observation and patient shadowing to help collect and understand experience. These methods provide useful analytical frameworks for understanding experience.2 Although often described as a cycle, EBCD follows a six-step linear approach (figure 1):2
Setting up the project, including gaining support;
Collecting staff experiences using ethnographic methods;
Collecting patient and carer experiences through ethnographic methods, including filmed narrative-based interviews focusing on the ‘touchpoints’ of engaging with a service. These interviews are spliced together based on common themes to form ‘trigger films’ to use in CD events;
First CD event with staff, patients and carers to view trigger films and identify priorities for change;
CD working parties focus on sets of priorities and implement changes;
Celebration and review event.
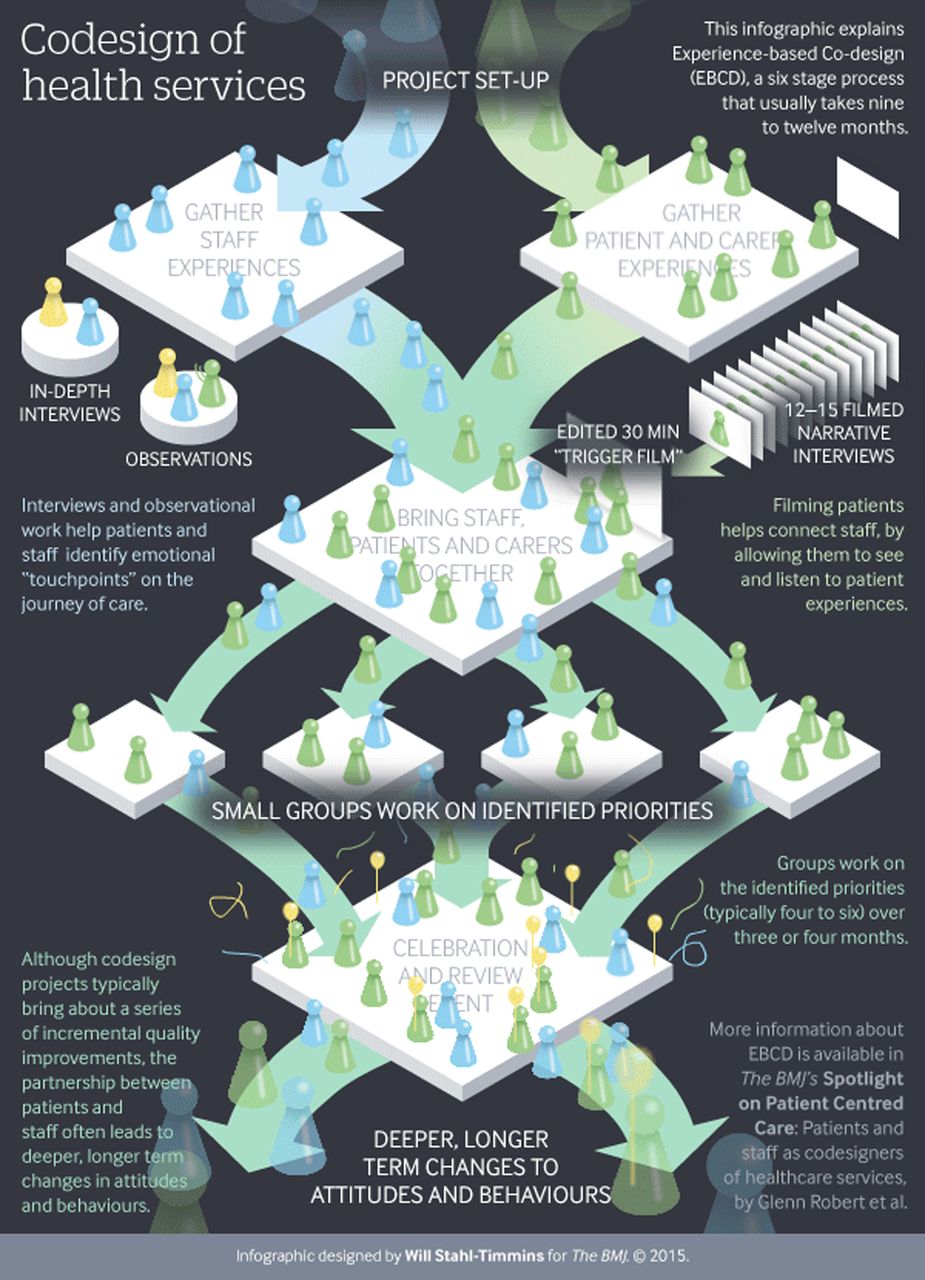
{kind=link}
Experience-based co-design process infographic designed by Will Stahl-Timmins for the BMJ in 2015.
In addition to these steps, evaluations of the methods used and/or changes to the services can inform future service development. One review found most projects typically take between 6 and 12 months, with a wide variety of methods used to capture experience and to facilitate CD workshops.3 Accelerated versions of EBCD can use videos from a national archive to cut down the time and cost involved in conducting projects.10 One study found that while in-depth narrative interviews and experiences gathered on surveys raised similar issues, interviews provided more in-depth understanding.11 The EBCD method is still relatively new and underused: as healthcare services become more digitally engaged with patients, variation in how it is employed are likely to continue with greater understanding of the limitations and advantages of different adaptations. More details can be found in the EBCD toolkit hosted by the King's Fund (see box 2).
The review
The rapid literature review, conducted for Marie Curie, identified 12 projects from across the globe that have drawn on EBD and/or CD methods to address palliative and end-of-life care services. Details of all the projects identified may be found in the review report.7 This paper provides an overview of the scope and key messages from the review before outlining several case studies to provide a flavour of this kind of methodological approach to service design.
Only two projects were identified that explicitly drew on the EBCD method12 ,13 with one that adapted the process to create experience-led commissioning (ELC).14 EBD, CD and EBCD have been used to generate a wide variety of outputs from commissioning statements, documents used in advance care planning and technologies. Two projects, neither of them based in the UK, focused more on the personal and interpersonal experience of space, place and communication within palliative and end-of-life care.13 ,15 Across all the projects, there was some variation in terms of who was involved and whose experiences were being sought; not all projects engaged patients, carers and professionals equally. All of the projects demonstrated how engaging with people's experiences of services can reshape how services are designed, but the processes, environments and interactions that are all part of care provision.
Case studies
Case study 1: ELC of end-of-life care services by Healthworks Clinical Commissioning Group, Birmingham in 2011
Drawing on EBCD and other participatory design models, five local events were held to engage stakeholders (users, user representatives, commissioners, service providers and other health professionals) to CD what end-of-life care services could look like using ‘blue skies thinking’. The trigger film used at the events was developed by researchers at Oxford University based on national archive videos (Healthtalkonline); similar videos are available online. Overall, the ELC process involved included: a service needs assessment; service design and specification CD workshop; contracting; monitoring and review; and change champions to facilitate implementation. Reported outcomes included: an end-of-life commissioning strategy document; a health assessment and management action plan for the CCG; a web-based interactive case study and other electronic resources; increased learning and networking for those who attended the events and the CCG.
A formal evaluation of the process was conducted, which provides more details of how ELC was managed.14 A key finding is that the ELC was considered by participants to be more ‘human’ and ‘real’ than the normal way of commissioning, by generating ‘meaningful’ user engagement and contribution from a wide range of stakeholders.14 The participatory methods therefore enabled the commissioning process to generate what was viewed as meaningful public consultations and CD in strategy and documents.
Case study 2: EBCD within research on the delivery of palliative care within an emergency department.
This PhD study based in the UK had two main phases of data collection.12 The first focused on gathering staff experiences through 17 semistructured interviews with nurses, doctors and coders as well as observations in the emergency department, post-take ward rounds and staff meetings. Based on this data collection, the researcher confirmed and validated her understanding of the process with nurses and doctors from the emergency department in a series of five feedback sessions staff. The second phase focused on patient and carer experiences, recruiting people with any life-limiting condition presumed to be in the last year to 6 months of life. Ten filmed interviews were conducted: six with patients (majority oncology) and four carers (two bereaved). During the recruitment process in the emergency department, the researcher made observations about patient and carer experiences, communication and interactions. All data were thematically analysed and cross-referenced for validation. The data were used to identify redesign priorities and the filmed interviews were used in the CD workshops.
CD workshops were held with older patients with palliative care needs, emergency department staff, the hospital's palliative care team and other stakeholders. The CD events identified four sets of challenges faced by staff, patients and carers in the emergency department and planned initial responses.
The first set of challenges is presented on a systems and process level, primarily concerned with helping patients and carers find their way through the emergency department and process. The group suggested a review of the IT systems, emergency preservation and resuscitation for cardiac arrest procedure, and the palliative care pathway through the emergency department.
The second theme highlighted communication and information issues, particularly around being informed and informing patients and carers. Potential solutions suggested included a palliative care passport to enable staff to identify patients with palliative care needs on arrival and an emergency department walk through to identify gaps in communication.
The third theme empathised seeing the person in the patient, suggesting that staff need more training (potentially linked to palliative care) and that cubicles could be redesigned. The last set of challenges focused specifically on training and education for staff, suggesting bespoke training and routine palliative care updates.
At the time of writing this research was being written up for the PhD: it is likely to be used in future service development projects.
Discussion
As we have already noted in the introduction, EBD and CD methods can have a particular synergy with palliative and end-of-life care. Both seek to foreground the patient (or user) experience and to enable shared decision-making. The review highlighted that there were few reported cases of using these methods within palliative and end-of-life care settings, although we would like to stress that the methods are relatively new and are gaining momentum. Moreover, such projects may not regularly be reported in the research or grey literature, although there is much benefit from sharing insights across projects. Here, we consider the appropriateness of these methods in palliative and end-of-life care settings, examples of potential uses beyond the case studies outlined above, and practical tips in addition to a general overview of the advantages and disadvantages of using the methods in practice.
Use within palliative and end-of-life care
A key focus within palliative and end-of-life care is on the quality of care provided to a patient. The methods described here are well situated to explore and respond to different experiences and perspectives as part of service design by giving voice to a variety of stakeholders and time to reflect and respond to this. It could be that involving patients and carers on projects like this may be ‘too sensitive’ and ‘distressing’. However, the case studies discussed here provide testimony that it can be done in a manner that enacts good ethical practice and does not overly emotionally burden those involved. Timeliness and when to involve patients who may be receiving end-of-life care is a particular issue within this field. Determining who to involve and when depends on the specific nature of the project and services involved. As with many research projects in palliative and end-of-life care it is likely that people will want to be involved. Since these methods are flexible, considerations can be made about the intensity and longevity across the life course of the project of a person's involvement (perhaps they provide an example of their experience but are not part of a working party). Although there may be particular concerns about the burdens collaborative projects place on stakeholders, it could be argued that such methods that focus on experience and valuing a wide range of voices are particularly needed in a field and at a time where the quality of care is regularly questioned and highly valuable to those involved.
The review found that these methods were being used in practice or theoretically to address issues, such as: advance care planning; delivery of care in emergency department; commissioning of services and pain management. We would suggest that the potential for these methods extends beyond these examples, and could include but is not limited to: other departments where palliative or end-of-life care are provided across health and social care settings, including home visits; communication of different kinds; peer support groups; symptom management; spiritual care provision; carer and family support; and bereavement. The first stage of the project should set out ideas for the scope while allowing for the CD workshops to set the priorities within that scope.
Practical tips
It was noted in several of the projects and in discussions with project leaders that people—staff, patients and carers—often want to take part, as they would like to see change. However, it can be difficult to know from the outset who to all involve, at what stage in the process to involve them and with what time commitment. It is therefore recommended that project teams map out potential stakeholders early on and engage with as many of them as early as possible. The toolkit provided by the King's Fund is useful for identifying and anticipating these issues, and provides a good starting base for those wishing to learn more about how to conduct these types of projects.
Several projects found staff engagement difficult to sustain and that managerial buy-in was necessary. When developing service innovation projects it is important therefore to realise the impact this may have on staff workload (and even the impact it can have for patients' and carers' activities) and to provide recognition of their contribution. Some sites have found it useful to have ‘hubs’ that highlight progress and provide a physical space to share ideas and ‘champions’ who actively promote the work of the projects and regularly engage stakeholders. Securing project or researching funding could help buy-out staff time and/or provide the finances to employ a project administrator or manager, which may be crucial for the success of larger projects or those with many working parties. The celebration event at the end of the project is another useful method for recognising and rewarding the work that is involved.
A key feature of these methods is the ability to bring together different groups to CD outcomes. When run well, these workshops set the tone and pace for the project and good facilitation was repeatedly mentioned as an important aspect.14 Personal communication with an experienced leader of several CD workshops stressed the importance of creating a level playing field and getting to know participants as people. This includes not making assumptions about cultural background or the taboo nature of certain topics—such as end-of-life care—but also respect if people do not wish to divulge certain aspects of their experiences. Good facilitators are able to enable equity in engagement, including listening to all stakeholders, and manage expectations created by the workshops.14 However, many facilitators are not trained or feel that CD and EBCD are a new area; courses and multiple tool kits are now available to support those who are interested in using these methods (see box 2).
Irrespective of the technique used, it is important to consider the emotional impact for those involved (both in generating content and listening to experiences) and to provide support and space to hear responses to the exercises. We would add that it is also useful to consider the impact on the project team and facilitators and to provide them with emotional support in their roles.
Although projects in the UK using this method may not require formal approval by a healthcare research ethics committee if conducted as a service improvement, it is still essential to apply ethical principles and good research practice.16
Benefits of these methods
Table 1 outlines the advantages and disadvantages of the method, discussed here in more detail. All publications about the projects identified in the review suggested that the methods used helped to understand the issues of service provision better, and where CD was involved, generated engagement between the stakeholders involved. The participatory methods built closer working relationships between professional groups, bringing communities together. Participant feedback, where provided, tended to be positive, patients and carers valuing the opportunity to be involved. Drawing on personal and professional experience generated empathy and trust in participants, challenging the assumptions and expectations of the project team or researchers, such as different cultural interpretations of care planning. It has been suggested that co-designed services might be more readily accepted by the wider patient population because services are tailored to focus on patient experience and are informed by user involvement.14
Advantages and disadvantages
There is considerable flexibility within the methodology.3 In the literature, mapping the ‘touchpoints’ or patient journey was noted as particularly helpful,17 connecting people with the activity in workshops and presenting a useful way to understand what it is like to experience a service. While supporters of the EBCD method stress the importance of video,3 not all projects reviewed used this method and some found they were able to have meaningful CD sessions without it.
Limitations of these methods
The main limitations to these methods discussed in the literature were the resources required and the barriers to change. Some of the projects had dedicated funding as part of a research or service design initiative:12 others were part of ongoing service provision and had to create time in staff schedules to conduct the project, which created difficulties in securing sustained staff engagement. As found in other reviews of EBCD, projects could be seen as costly and time-intensive, although accelerated versions of EBCD can be quicker and cheaper: overall these methods can be less resource-intense compared with other research methods.3 It should also be considered that conducting these projects enhances skills of staff, encourages team work and can improve the patient–professional relationship. This is in addition to the anticipated improvements in how the service is delivered and experienced.
As with other change development projects, EBD, CD and EBCD projects faced the difficulty of creating sustainable change within a complex and ever-shifting healthcare system. The evaluators of the ELC project noted that it is unclear if such work can lead to sustainable changes.14 Others have noted that while EBD and CD only usually provide incremental quality improvement in the healthcare setting, they also set the scene for longer term change by shifting behaviours and attitudes towards a focus on experience, collaboration and continuous development.3 Building projects into a larger commitment to continuously improve services can help foster this shift. The small numbers and types of people likely to participate in CD also create difficultly in achieving representativeness for wider patient populations. It was not always clear that projects appreciated these caveats in understanding how and what was being co-designed, and how this may affect the long-term viability of service developments.
Limitation in current reporting and knowledge transfer
Sources varied in the level of detail about the methods used, the form and content of CD workshops, or how working parties developed services. This probably reflects the sources of publication and the conventions that accompany different styles, such as journal article word limits; grey literature and conversations with project leaders provided more detailed information. While projects reported outcomes of workshops, there was little analysis of the themes derived from earlier data collection (ie, the videos) or information concerning the interactions between people, including the role of designers, in the workshops. This makes it difficult to compare projects, and for others to learn directly from projects to inform their own service developments. More consistent reporting would enable knowledge sharing between sites and enable the translation of learning from one context to another.
For most projects, we were unable to identify formal or informal evaluations: the main exception was the evaluation of the ELC project, although this did not include information on cost of different elements of the project.14 Some projects suggested that they did not perform overall evaluations as there was local and political support for participatory methods, and any feedback they conducted focused on running the CD workshops to improve facilitation in the future. Others suggested that design projects more generally often do not undergo the same kind of review or evaluation that healthcare research and implementation typically employs. This is not to say that future projects could not, or should not, involve some element of evaluation, especially as an evidence base is built for these methods within research and service innovation.
Conclusion
EBD, CD and EBCD all offer a variety of techniques to generate service development that is focused on the experiences of service delivery through engagement with a wide range of stakeholders. Within palliative and end-of-life care, there have been to date few projects published that have used these methods and the quality of reporting varies. Consequently, while we are able to identify the potential to use these methods within the field of palliative and end-of-life care, more could be done to document what is being done, how collaboration is being achieved, and evaluation of the changes implemented. Sharing experiences of using these methods helps in knowledge transfer.
From a research perspective, there is scope for more theorising about how EBD, CD and EBCD function within the palliative and end-of-life care setting and the experiential and emotional aspects of this method. This could be part of evaluations that should cover a wide spectrum of implications, including cost, and reflect the implementation of solutions devised in CD workshops. Based on the review, it is evident that the development of these methods within research and service improvement can improve the ways in which patients, carers and professionals experience receiving and delivering care, but more can be done in documenting and sharing these projects.
Acknowledgments
The authors would like to thank Marie Curie for funding the review that this article is based on. The authors also would like to thank Glenn Robert, Rebecca Black, Leigh Manson and Alastair Macdonald for their insights into the methods discussed. The authors would also like to thank their colleagues and the reviewers who offered constructive feedback on earlier drafts.
Footnotes
Twitter Follow Erica Borgstrom @ericaborgstrom
Contributors EB and SB conducted the review and wrote the subsequent report and this paper.
Funding The authors received funding from Marie Curie to complete the research related to this article.
Disclaimer The views are the authors' own, not those of the funders.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement More details of the methods employed in the review and the sources can be found in the report written by EB and SB (2015) for Marie Curie, cited in this article.