Article Text

Abstract
Objective We evaluated the effect of the systemic inflammatory response (SIR), as provoked by elective orthopaedic surgery, on serum vitamin D [25-(OH)D].
Methods Serum 25-(OH)D, serum vitamin D binding protein (VDBP) and urinary VDBP were measured in 30 patients before and 48-hours after knee or hip arthroplasty. C-reactive protein (CRP) was measured to assess the SIR.
Results The mean (SD) CRP increased following surgery [5.0 (5.5) vs 116.0 (81.2) mg/L; P<0.0001] as did urine VDBP/Creatinine ratio [8 (9) vs 20 (25) pg/mmol; p=0.0004]. Serum 25-(OH)D [56.2 (30.3) vs 46.0 (27.6) nmol/L; p = 0.0006] and serum VDBP [334 (43) vs 298 (37) mg/L]; P<0.0001] decreased.
Conclusions Serum 25-(OH)D is a negative acute phase reactant, which has implications for acute and chronic inflammatory diseases. Serum 25-(OH)D is an unreliable biomarker of vitamin D status after acute inflammatory insult. Hypovitaminosis D may be the consequence rather than cause of chronic inflammatory diseases.
- VITAMIN D
- ACUTE PHASE PROTEINS
- INFLAMMATION
Statistics from Altmetric.com
Introduction
Limited data on the effect of the systemic inflammatory response (SIR) on circulating 25 hydroxy-vitamin D (25-(OH)D) concentrations are conflicting. Serum 25-(OH)D has been reported as either decreased1 ,2 or unchanged3 ,4 during an SIR. Since hypovitaminosis D has been associated with a wide range of, often inflammatory, acute and chronic diseases,5–7 it is essential to ascertain whether serum 25-(OH)D is affected by acute inflammation.
We therefore prospectively evaluated the effect of the SIR on serum 25-(OH)D concentrations by measuring serum 25-(OH)D before and 48 h after elective knee or hip arthroplasty.
Methods
Patients
Patients undergoing elective hip or knee surgery were recruited from those attending orthopaedic outpatient clinics. Exclusion criteria included patients on vitamin D supplements, renal impairment, postoperative infection and postoperative blood transfusion. Patients gave informed written consent to participate in this study, which was approved by the Black Country Research Ethics Committee.
Resting blood and urine samples were collected into gel tubes (Sarstedt Monovet 4.7 ml, Z GEL, Sarstedt, Numbrecht, Germany) and plain universal specimen containers (SSI 30 ml, polypropylene, International Scientific Supplies Ltd, Bradford, UK), respectively, within 4 weeks prior to surgery and then 48 h after surgery. Serum was separated within 60 min. Separated serum and urine were aliquotted and frozen at −80°C until analysed in a single batch to minimise inter-batch analytical variation.
Analytical methods
Serum 25-(OH)D was measured by liquid chromatography-tandem mass spectrometry, following a liquid–liquid extraction procedure.8 Creatinine (kinetic Jaffé method), C reactive protein (CRP) (immunoturbidimetry), serum albumin (Bromocresol green, colorimetric endpoint method), serum calcium (O-Cresolphthalein, colorimetric endpoint method) and urine albumin (immunoturbidimetry) were measured using Roche reagents on the Roche MODULAR P analyser (Roche Diagnostics GmbH, Mannheim, Germany). Free, non-actin bound vitamin D binding protein (VDBP) in serum and urine was determined by an Immunodiagnostik Enzyme Immuno Assay using a microtitre plate coated with polyclonal anti-VDBP antibodies (Biohit HealthCare, Cheshire, UK) on a Grifols Triturus automated ELISA platform (Grifols UK, Cambridge, UK).
Respective intra-assay coefficients of variation are for 25-(OH)D ≤12% over the concentration range 20.7–187.7 nmol/l, serum creatinine 0.7% at 148 µmol/l, urine creatinine 1.1% at 5.39 mmol/l, serum CRP 2.5% at 5.8 mg/l, serum albumin 1.7% at 32 g/l, serum calcium 1.5% at 2.09 mmol/l, serum VDBP 12.8% at 259 mg/l, urine albumin 1.3% at 24.9 mg/l and urine VDBP 3.4% at 29.3 µg/l.
Urine microalbumin was corrected for urine flow rate by expression as the albumin to creatinine ratio (ACR).
Statistical analysis
The Kolmogorov and Smirnov method was used to assess normality of data. Raw urine ACR and VDBP/creatinine data were non-parametric but were normally distributed following logarithmic transformation. All other data were parametric. Paired t test was, therefore, used to assess the significance of differences between raw parametric data or logarithmically transformed urine ACR and VDBP/creatinine data. Pearson's linear correlation was used to assess the significance of association between raw or logarithmically transformed parametric variables. Data processing and statistical analyses were performed using GraphPad Instat V.3.00 for Windows 95 (GraphPad Software, San Diego, California, USA). Data (including pretransformed raw urine ACR and VDBP/creatinine data) are expressed as means with SD in parentheses.
Results
We studied 30 patients (17 female subjects) aged 64.9 (8.7) years, of whom 24 had elective knee surgery. A total of 25 patients had osteoarthritis and five patients had rheumatoid arthritis. Other comorbidities included diabetes (two patients), ischaemic heart disease (one patient), hypertension (eight patients), hyperlipidaemia (five patients), hypothyroidism on thyroxine replacement (one patient) and epilepsy (one patient).
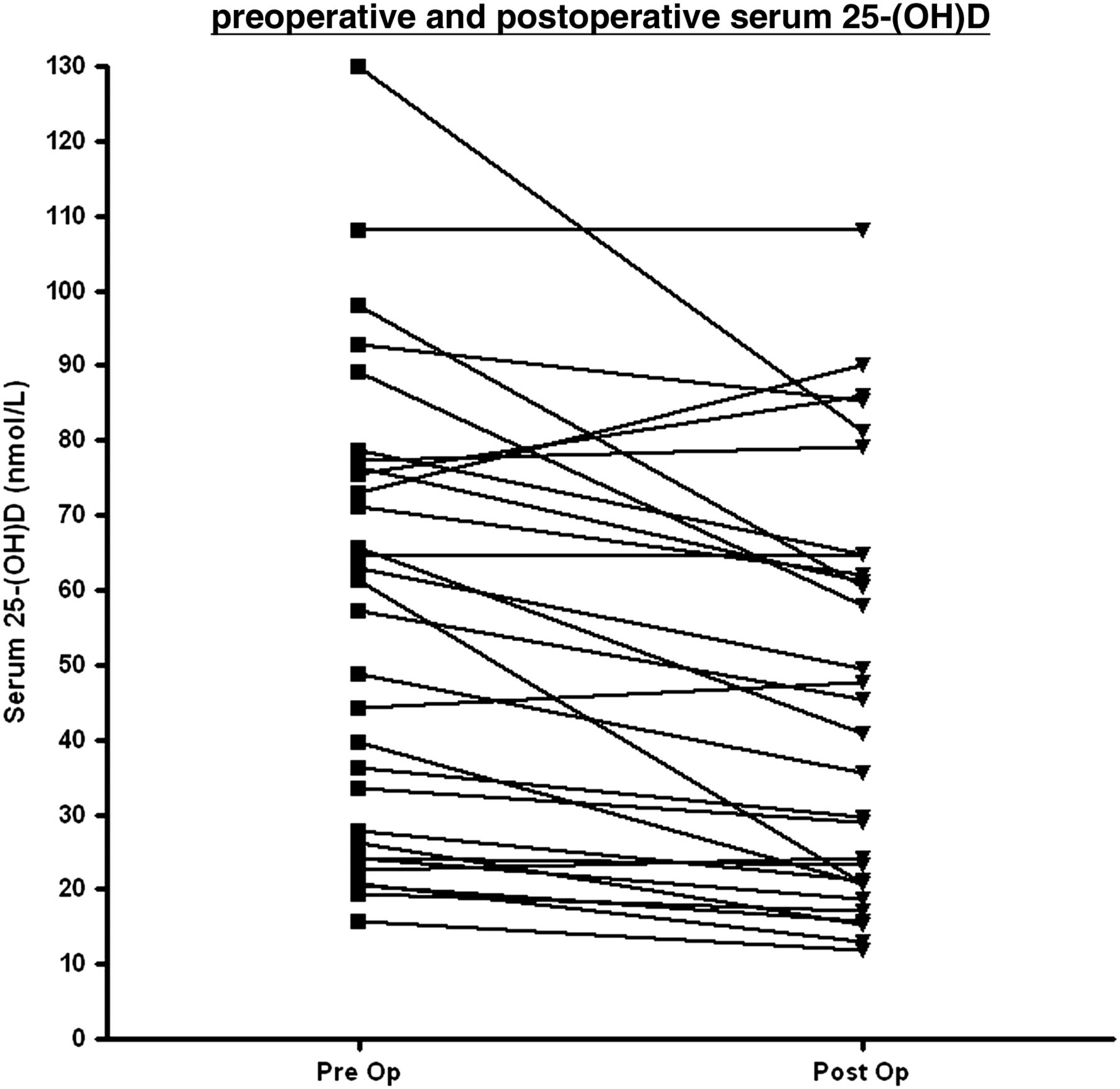
Preoperative serum 25-(OH)D concentrations indicated vitamin D adequacy (>50 nmol/l), insufficiency (30–50 nmol/l) and deficiency (<29 nmol/l) in 53%, 17% and 30% of patients, respectively. The preoperative and postoperative raw biochemical data are shown in the table 1 and figure 1. In summary, following surgery serum CRP and urine ACR concentrations increased (p<0.0001 and p<0.004, respectively), as did urine VDBP/creatinine (p=0.0004), whereas serum 25-(OH)D, albumin and VDBP decreased (p=0.0006, p<0.0001 and p<0.0001, respectively). Serum creatinine and adjusted calcium concentrations were similar before and after surgery. There were no meaningful correlations and, in particular, the absolute change in serum 25-(OH)D did not correlate with the absolute change in CRP (r=0.1273, p=0.5025).
Biochemical data in 30 patients before and 48 h after elective knee or hip surgery

{kind=link}
Plot of individual change within patients for serum 25-(OH)D. The square and triangle points indicate preoperative and postoperative values for serum 25-(OH)D, respectively.
Discussion
Serum 25-(OH)D concentrations decreased following elective knee and hip surgery. The postoperative increase in serum CRP and urine ACR confirms that an SIR was provoked solely by surgery, since none of the patients developed postoperative infection or other acute inflammatory disease. The decrease in serum 25-(OH)D concentrations was, therefore, associated with the SIR.
Our results are consistent with those of two other studies reporting a rapid and significant fall in serum 25(OH)D concentration during an SIR.1 ,2 They appear, however, to contradict the results of two other studies reporting no change in serum 25(OH)D concentration after an inflammatory insult.3 ,4
Reid et al reported that following elective knee arthroplasty, serum 25-(OH)D decreased by 40% to a nadir at 2 days at a time when the SIR as assessed by serum CRP was at its peak. Serum 25-(OH)D concentrations were still significantly 20% lower after 3 months by which time the SIR had resolved as assessed by a normal CRP.2 Louw et al similarly reported a significant but transient decline in serum 25(OH)D of 15%–20% within 48 h following uncomplicated orthopaedic surgery. This corresponded with the SIR as monitored by a reciprocal increase in CRP concentration, with a peak value at 48 h postsurgery.1
Two other recent studies, however, have reported no change in serum 25-(OH)D concentrations for up to 42 and 90 days during malarial infection and following myocardial infarction, respectively.3 ,4 The initial serum samples in these two studies were, however, all collected after the inflammatory insult at a time when we and others1 ,2 have shown serum 25-(OH)D is already likely to be at a nadir. A unifying explanation for the apparently conflicting results of these studies is that serum 25-(OH)D concentrations decrease rapidly and dramatically after an inflammatory insult and persist for at least 3 months.
Our study confirms that serum VDBP falls during an SIR2 ,9 ,10 and this may explain, at least in part, the fall in the serum 25-(OH)D. The postoperative decrease in serum 25-(OH)D concentrations may, therefore, just reflect a loss of VDBP and thus 25-(OH)D from the circulation due to the redistribution that occurs during the SIR.11 ,12 In addition, we have shown for the first time that the decrease in serum VDBP during an SIR is associated with increased urinary loss of VDBP. Although significant, the urine loss of VDBP is relatively small and therefore unlikely to significantly contribute to the decrease in serum 25-(OH)D.
We conclude that serum 25-(OH)D is a negative acute phase reactant, which has implications for acute and chronic diseases. First, serum 25-(OH)D is an unreliable biomarker of vitamin D status after an acute inflammatory insult. Second, it supports the notion that hypovitaminosis D may be the consequence rather than the widely purported cause of a myriad of chronic diseases.13
Key messages
-
25(OH)D3 decreases during the systemic inflammatory response (SIR).
-
25(OH)D3 is an unreliable marker of vitamin D status following a SIR.
-
Hypovitaminosis D may be the consequence rather than cause of chronic inflammatory disease.
Acknowledgments
The authors would like to thank the orthopaedic preoperative clinic nursing team for their help with patient recruitment and Ross Wheatcroft (Grifols UK) for his technical support with the VDBP assay.
References
Footnotes
-
Contributors JLW researched the literature, recruited patients, took consent, collected samples, helped supervise the study, analysed samples, analysed the data and wrote the first draft. HLA researched the literature, designed and supervised the study, recruited patients, took consent and collected samples. JB researched the literature and helped design the study. CR recruited patients, took consent and collected samples. OLT, SD, SC, CF and RG contributed to the data. RMG and MPC conceived the study. All authors reviewed and edited the manuscript and approved the final version of the manuscript. Guarantor: RG.
-
Funding No funding support has been received for this study.
-
Competing interests None.
-
Ethics approval Granted by the Black Country Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.