Article Text

Abstract
Background: The aim of this study was to identify key factors on admission predicting the development of complicated parapneumonic effusion or empyema in patients admitted with community-acquired pneumonia.
Methods: A prospective observational study of patients admitted with community-acquired pneumonia in NHS Lothian, UK, was conducted. Multivariate regression analyses were used to evaluate factors that could predict the development of complicated parapneumonic effusion or empyema, including admission demographics, clinical features, laboratory tests and pneumonia-specific (Pneumonia Severity Index (PSI), CURB65 (New onset confusion, urea >7 mmol/l, Respiratory rate ≥30 breaths/min, Systolic blood pressure < 90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years) and CRB65 (New onset confusion, Respiratory rate ≥30 breaths/min, Systolic blood pressure <90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years)) and generic sepsis scoring systems (APACHE II (Acute Physiology and Chronic Health Evaluation II), SEWS (standardised early warning score) and systemic inflammatory response syndrome (SIRS)).
Results: 1269 patients were included in the study and 92 patients (7.2%) developed complicated parapneumonic effusion or empyema. The pneumonia-specific and generic sepsis scoring systems had no value in predicting complicated parapneumonic effusion or empyema.
Multivariate logistic regression identified albumin <30 g/l adjusted odds ratio (AOR) 4.55 (95% CI 2.45 to 8.45, p<0.0001), sodium <130 mmol/l AOR 2.70 (1.55 to 4.70, p = 0.0005), platelet count >400×109/l AOR 4.09 (2.21 to 7.54, p<0.0001), C-reactive protein >100 mg/l AOR 15.7 (3.69 to 66.9, p<0.0001) and a history of alcohol abuse AOR 4.28 (1.87 to 9.82, p = 0.0006) or intravenous drug use AOR 2.82 (1.09 to 7.30, p = 0.03) as independently associated with development of complicated parapneumonic effusion or empyema. A history of chronic obstructive pulmonary disease was associated with decreased risk, AOR 0.18 (0.06 to 0.53, p = 0.002). A 6-point scoring system using these combined variables had good discriminatory value: area under the receiver operator characteristic curve (AUC) 0.84 (95% CI 0.81 to 0.86, p<0.0001).
Conclusion: This study has identified seven clinical factors predicting the development of complicated parapneumonic effusion or empyema. Independent validation is needed.
Statistics from Altmetric.com
Complicated parapneumonic effusions and empyema are key complications of community-acquired pneumonia necessitating prolonged treatment, intercostal drainage and frequently surgical management, leading to prolonged hospital stay.1–3
In 1980, Light and colleagues established the criteria that are now used to define complicated parapneumonic effusions but found no reliable clinical or radiological features to predict which patients with community-acquired pneumonia will develop complicated parapneumonic effusions or empyema.4 Only small studies have been available to date.
Pneumonia severity scores including CURB65 (New onset confusion, urea >7 mmol/l, Respiratory rate ≥30 breaths/min, Systolic blood pressure <90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years), CRB65 (New onset confusion, Respiratory rate ≥30 breaths/min, Systolic blood pressure <90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years) and the Pneumonia Severity Index (PSI)5–9 have been used on admission to predict 30-day mortality, but no-one to date has studied their utility to predict the development of complicated parapneumonic effusion or empyema.
The aim of this study was to identify key factors predicting the development of complicated parapneumonic effusion or empyema in patients admitted with community-acquired pneumonia.
METHODS
We prospectively identified all patients, admitted between January 2005 and January 2008 to NHS Lothian, UK, with a primary diagnosis of community-acquired pneumonia. Ethical approval was obtained from the Lothian research ethics committee.
The inclusion criteria and study protocol have been described previously.9 Exclusion criteria were hospital-acquired pneumonia (development of symptoms >48 h after admission to hospital or discharge from an acute care facility within 14 days of admission); active thoracic or extrathoracic malignancy; metastatic infection from a non-pulmonary source; immunosuppression (including patients prescribed long-term prednisolone, methotrexate, azathioprine or antitumour necrosis α (TNFα) treatment); solid organ transplant; previous empyema or chronic pleural effusion due to a cause other than pneumonia; recent thoracic surgery; and patients for whom active treatment is not considered appropriate (eg, palliative care).
Identification of parapneumonic effusions
All patients had a standard chest radiograph within 24 h of admission, and this was repeated if clinically indicated. All patients with pleural effusions underwent clinical assessment and thoracic ultrasound if required. All patients with pleural effusion underwent thoracocentesis, except in small pleural effusions thought unsafe for pleural aspiration from thoracic ultrasound. Fluid was analysed for pH, protein, lactate dehydrogenase (LDH), glucose, Gram stain, culture and cytology. In patients with empyema too viscous to analyse, the sample was sent for Gram stain and microbiological culture only.
Definition of complicated pneumonia and empyema
The primary outcome was development of complicated parapneumonic effusion or empyema. Complicated parapneumonic effusion was defined according to the criteria described by Light and colleagues4 as at least one of pleural fluid pH<7.2, LDH >1000 IU/l or glucose <2.2 mmol/l. Empyema was defined as frank pus aspirated from the pleural space or positive Gram stain/culture for pathogenic organisms.
For the purposes of comparison, early development of complicated parapneumonic effusion/empyema was defined as diagnosis ⩽72 h after admission to hospital. Late development of empyema was defined as diagnosis >72 h after admission. The date of diagnosis of empyema was taken to be the date of the confirmatory thoracocentesis.
Severity scores
We evaluated factors that could predict the development of complicated parapneumonic effusion or empyema, including admission demographics, clinical features, laboratory tests and severity scores. The pneumonia-specific scores included the PSI,7 CURB655 and CRB65.5 The generic sepsis scores included the APACHE II (Acute Physiology and Chronic Health Evaluation II) score,10 SIRS (systemic inflammatory response syndrome) criteria11 and SEWS (standardised early warning score) score.12 For the purposes of calculating the values of predictive tests the following were used to define “severe” for each scoring system, PSI ⩾4; CURB65 ⩾3; CRB65 ⩾3; SIRS severe sepsis or septic shock; SEWS ⩾4. The APACHE score is a progressive scale with increasing estimated death rates for increasing scores. For purposes of comparison in this study “severe” was arbitrarily set at >9 points prior to the study which equates to a >9.9% risk of death.
Statistical analysis
Demographic, clinical, laboratory, radiological and other variables were converted to binary variables based on cut-off points identified in the community-acquired pneumonia literature, primarily studies focusing on mortality. The relative risks were expressed as adjusted odds ratios (AORs) and 95% CI. All variables that were statistically significant in the univariate analysis with a p value <0.05 were entered in a multivariable model with a stepwise approach. Multicollinearity was assessed by using bivariate linear regression between variables and using the variance inflation factor. A variance inflation factor (VIF) of <2.5 was regarded as excluding significant interactions.13
The value of tests for predicting outcomes was compared using the area under the receiver operator characteristic curve (AUC).14 For interpretation of these values the following is widely accepted: AUC 0.50–0.59, no value of test; 0.60–0.69, poor discriminatory value; 0.70–0.79, moderate discriminatory value; 0.80–0.89, good discriminatory value; 0.90–1.00, excellent discriminatory value.
The χ2 test was used to compare categorical variables, and for continuous variables the Mann–Whitney U test was used for two groups. Data are presented as number (percentage) or median (interquartile range (IQR)). A p value of <0.05 was considered statistically significant for each analysis.
RESULTS
A total of 1628 patients were considered for inclusion and 359 patients were excluded (see fig 1); 1269 patients were therefore included in the study. Ninety-two patients (7.2%) met the criteria for complicated parapneumonic effusion (74 patients, 5.8%) or empyema (18 patients, 1.4%).

Method of identification of cases of complicated parapneumonic effusion and empyema. LDH, lactate dehydrogenase.
Baseline characteristics and comorbidities of the study population are shown in table 1. Pleural fluid characteristics were as follows for patients developing complicated parapneumonic effusion or empyema: median pH 7.1 (IQR 7.0–7.2); glucose 1.0 mmol/l (0.6–2.5), protein 40 g/l (35–46); LDH 2900 IU/l (1035–4720).
Microbiology of empyema
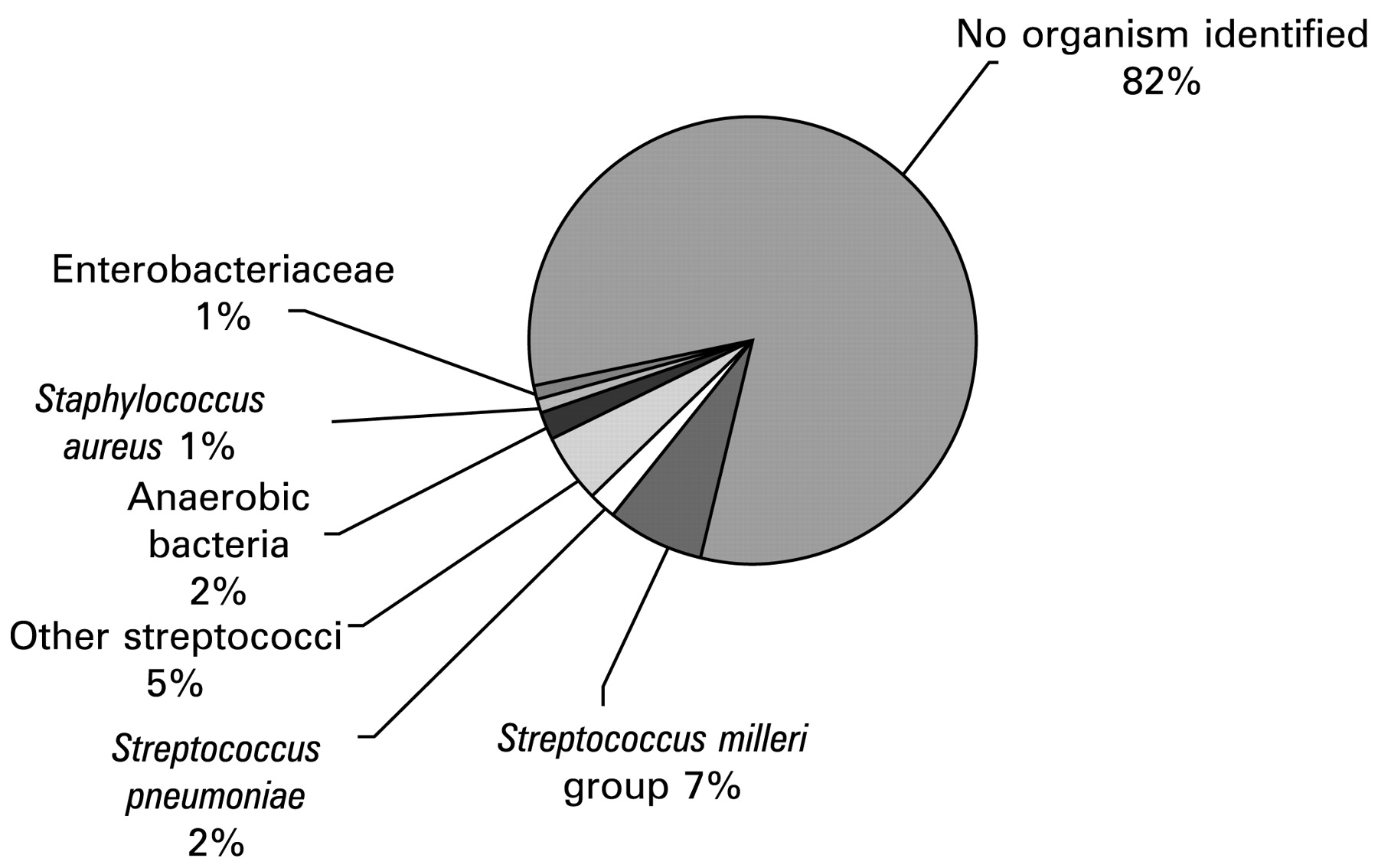
A positive pleural fluid culture was found in 16/92 patients. The Streptococcus milleri group (S intermedius, S constellatus and S mitis) were the most frequent organisms isolated in six cases. S pneumoniae was isolated in two cases and other streptococci were isolated in four cases. Two samples grew anaerobic organisms. Staphylococcus aureus and Enterobacteriaceae were isolated in a single case. Ninety-two patients (100%) had received antibiotic treatment prior to pleural aspiration. The organisms isolated are shown in fig 2.

Microbiology of empyema.
Outcomes in patients with and without complicated parapneumonic effusion or empyema
Patients with complicated parapneumonic effusion or empyema had longer length of stay and higher rates of intensive care unit admission compared with patients without these complications. The 30-day mortality rate was not significantly different between groups (table 2).
Ninety-two patients (100%) meeting the criteria for complicated parapneumonic effusion or empyema had an intercostal drain inserted for drainage of their effusion. Intrapleural fibrinolytics were not used. Eighteen patients failed to improve with chest tube drainage and subsequently required surgical thoracotomy. Two of these patients died within 30 days of admission. A further six patients died within 30 days and had not received thoracotomy. Twenty-four patients (22%) were therefore categorised as failure of medical treatment.
Recognised severity scores
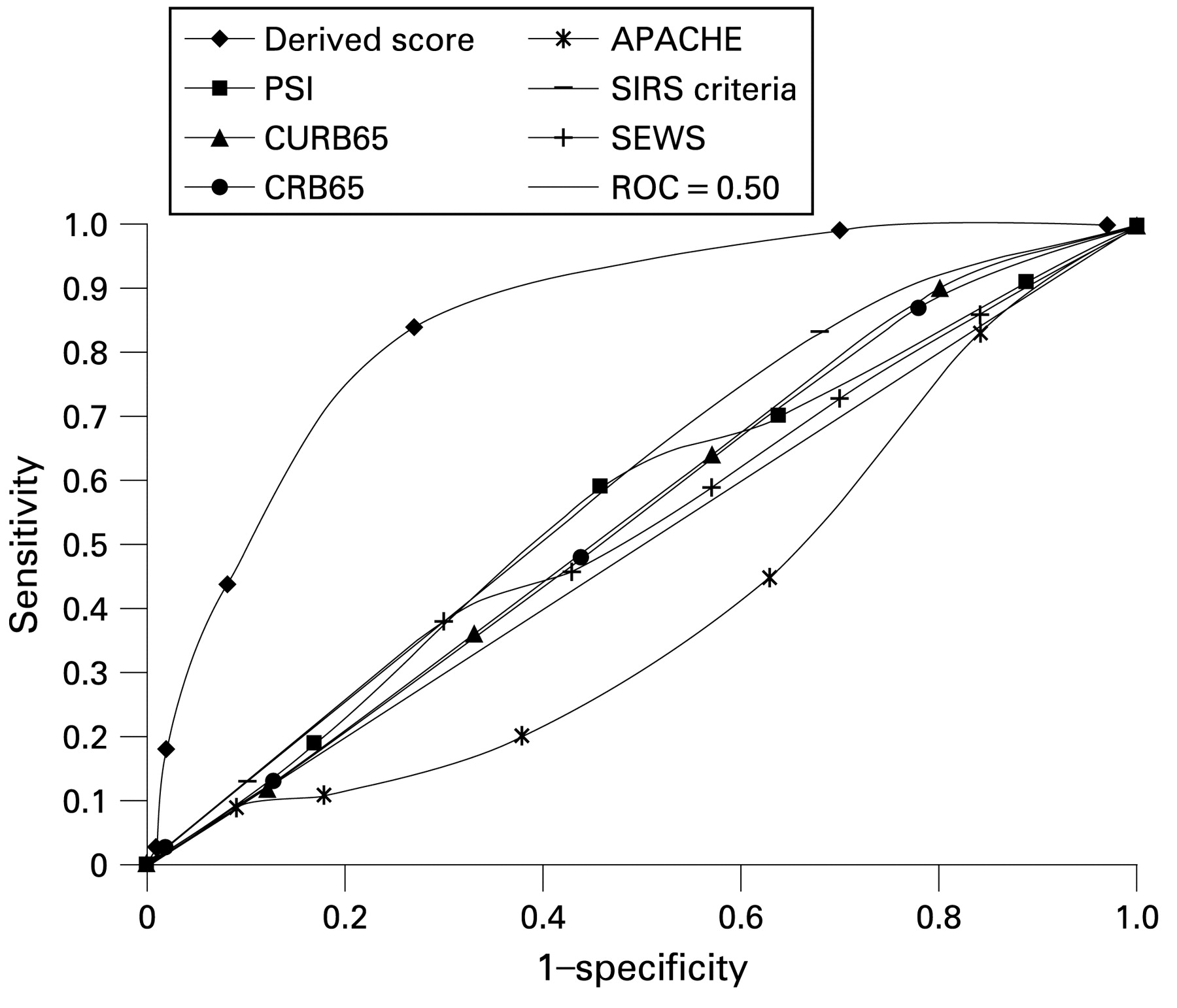
Recognised severity scores were compared for their ability to predict the development of complicated parapneumonic effusion or empyema. All had low AUCs for the prediction of complicated parapneumonic effusion and empyema (see fig 3 and table 3.

Receiver operator characteristic (ROC) curves for widely used severity scores and development of complicated parapneumonic effusion or empyema. APACHE II, Acute Physiology and Chronic Health Evaluation II; CRB65, New onset confusion, Respiratory rate ≥30 breaths/min, Systolic blood pressure <90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years; CURB65, New onset confusion, urea >7 mmol/l, Respiratory rate ≥30 breaths/min, Systolic blood pressure <90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years; SEWS, standardised early warning score; SIRS, systemic inflammatory response syndrome.
The positive predictive value, negative predictive value, sensitivity, specificity and AUC for each rule are shown in table 3.
Prediction of development of complicated parapneumonic effusion or empyema
Complete clinical data were available for all patients, with the exception of arterial blood gas measurements which were not performed in all patients and so were not included in the multivariate analysis.
On multivariate logistic regression, low serum albumin <30 g/l, elevated C-reactive protein (CRP) >100 mg/l and platelet count >400×109/l, low serum sodium <130 mmol/l, intravenous drug use or chronic alcohol abuse were all were identified as independent predictors of the subsequent development of complicated parapneumonic effusion or empyema. A history of chronic obstructive pulmonary disease (COPD) was associated with decreased risk (table 4). No strong correlations were identified between predictors. No VIF was >2.5 and the average VIF was 1.03.
Clinical application of the data
A scoring system was developed to assess if the identified “risk factors” for development of complicated parapneumonic effusion or empyema could be applied clinically. Each risk factor identified in the multivariate analysis that predicts complicated parapneumonic effusion or empyema (table 5) was given a numerical value (+1 point); 1 point was subtracted for the presence of COPD. The incidence of complicated parapneumonic effusion or empyema according the number of risk factors is shown in table 5.
Although in theory this was a 6-point score, in practice no patients had the maximum of 6 points. The resultant scoring system was analysed using the AUC. There appeared to be a clear separation between patients with 1 point (2.4%) and patients with higher scores (⩾11.8%), and so performance characteristics were calculated with these values representing high and low risk of developing complicated parapneumonic effusion and empyema.
For predicting complicated parapneumonic effusion or empyema, using ⩾2 point as the cut-off, the sensitivity is 87.0%, specificity is 68.3%, positive predictive value is 17.7%, negative predictive value is 98.5% and AUC is 0.84 (0.81 to 0.86), p<0.0001 (fig 4). This score was superior to all of the severity scores in table 3 for prediction of complicated parapneumonic effusion or empyema (p<0.0001 for all analyses).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operator characteristic (ROC) curve for the derived risk score and prediction of complicated parapneumonic effusion or empyema. APACHE II, Acute Physiology and Chronic Health Evaluation II; CRB65, New onset confusion, Respiratory rate ≥30 breaths/min, Systolic blood pressure <90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years; CURB65, New onset confusion, urea >7 mmol/l, Respiratory rate ≥30 breaths/min, Systolic blood pressure <90 mm Hg and/or diastolic blood pressure ≤60 mm Hg and age ≥65 years; SEWS, standardised early warning score; SIRS, systemic inflammatory response syndrome.
Early versus late complicated parapneumonic effusion/empyema
Twenty-two patients (24%) had the diagnosis of complicated parapneumonic effusion or empyema made within 72 h of admission. The AUC for the derived score was 0.86 (0.81 to 0.91) for prediction of early complicated parapneumonic effusion/empyema and the AUC was 0.83 (0.80 to 0.86) for prediction of late complicated parapneumonic effusion/empyema.
DISCUSSION
This study has identified seven key features that can determine patients at risk of development of complicated parapneumonic effusion or empyema. Low serum albumin <30 g/l, CRP >100 mg/l, platelet count >400×109/l, serum sodium <130 mmol/l, intravenous drug use and chronic alcohol abuse were all were identified as independent predictors of the subsequent development of complicated parapneumonic effusion or empyema. A history of COPD was found to be associated with decreased risk.
Using this information, this study has provided proof of the concept that complicated parapneumonic effusion and empyema can be predicted by deriving a scoring system with good predictive value. The presence of ⩾2 of the above risk factors has a 87% sensitivity for detection of complicated parapneumonic effusion or empyema, and a score of <2 gives a negative predictive value of 98.5%. The scoring system had “good” performance characteristics for predicting both early and late parapneumonic effusion and empyema. This scoring system now requires independent validation.
Although in univariate analysis, patients with complicated parapneumonic effusion and empyema were younger, more likely to be male and more likely to be current smokers, these differences were not significant in the multivariate analysis.
The risk factors identified in this study are supported by the existing literature. Alcohol abuse is the most common disorder reported in patients with empyema.15 16 Aspiration of gastric contents and the failure to seek prompt medical attention are two mechanisms that have been proposed to explain this. This may also in part explain the increased incidence of patients with a history of intravenous drug use. There is strong evidence that inflammatory markers are elevated in patients with parapneumonic effusions and empyema, as pleural inflammation is the characteristic feature of these diseases.17 In the present study CRP >100 mg/l was strongly associated with the development of empyema or complicated parapneumonic effusion. It is well recognised that patients with an elevated CRP on admission that fails to fall with treatment are at increased risk of complicated parapneumonic effusion or empyema.18–20 Elevated platelet count is also well recognised in acute and chronic infections.21 Empyema is a recognised cause of the syndrome of inappropriate antidiuretic hormone secretion (SIADH),22 but hyponatraemia is also recognised in severe community-acquired pneumonia without SIADH.23 Hypoalbuminaemia is well recognised in severe community-acquired pneumonia as well as being associated with the development of empyema.7 23 24
The finding that COPD was associated with a decreased risk of complicated parapneumonic effusion and empyema is intriguing. There are compelling reasons to believe that patients with COPD should have increased mortality from pneumonia, but prognostic studies to date have found that this is not the case.7 23 Authors have speculated that the local pulmonary inflammation present in patients with COPD may produce a dampened response when exposed to an acute bacterial challenge.25 The acute administration of steroids is another important potential confounding factor. Steroids have potent effects on attenuating pulmonary and systemic inflammation26 and may also attenuate pleural inflammation.
The widely used pneumonia severity and sepsis severity scores considered in this study were not found to be useful for predicting the development of complicated parapneumonic effusion or empyema. The clinical features that predispose to 30-day mortality from pneumonia are clearly different from those identified in this study to predispose to the development of complicated parapneumonic effusion or empyema. Of the risk factors identified in this study, only hypoalbuminaemia, hyponatraemia and an elevated CRP have been identified as independent risk factors for mortality, and none of these is among the “core” high risk features carrying the greatest risk of death.
This study found that the S milleri group was the most frequently isolated organism in patients with empyema, followed by other streptococci. This is consistent with the findings of the UK trial of intrapleural streptokinase and a recent study of patients with community-acquired pleural infection from Canada.27 28
However, 82% of patients had no organisms cultured. The frequency of positive microbiological diagnosis in this study is lower than in many other published studies of empyema, which have reported a microbiological diagnosis in between 40% and 60% of cases.29–32 Several factors may account for this; first, many of these studies have reported positive blood cultures in addition to positive fluid microbiology29 rather than simply positive pleural fluid cultures, which is the case in this study. Many studies have focused exclusively on empyema and consequently reported a much higher incidence of patients with frankly purulent effusions,27–30 which may be more likely to give a positive result. In addition, prior antibiotic treatment is likely to play a role, as empirical treatment in community-acquired pneumonia covers the majority of potential organisms, whereas in other studies the aetiology of empyema is variable and it cannot be said with certainty whether empirical treatment was effective against the organisms isolated.
Limitations
Although the clinical assessment of patients in this study was comprehensive, 27 patients had pleural effusions that were not sampled, because thoracic ultrasound indicated insufficient pleural fluid to tap safely. As all patients were followed up, we feel that it is unlikely that clinically important cases of pleural infection were missed.
This study represents a large cohort of patients with community-acquired pneumonia; the numbers developing the outcome of interest (92 patients in total) were relatively small, and this is reflected in the wide confidence intervals for some of the individual predictors. Multicentre studies would be required to define the relative risks more accurately.
Athough the performance of the derived predictive score is defined as “good” (AUC 0.84) in our study population, prospective validation is required before any recommendations can be made about its use in clinical practice.
Conclusion
There are important differences in the presentation of patients with complicated parapneumonic effusion and empyema compared with patients with uncomplicated community-acquired pneumonia. Pneumonia and generic sepsis scores do not predict the development of these complications, but a simple 6-point scoring system can allow identification of high risk patients. Independent validation studies are needed.
REFERENCES
Footnotes
See Editorial, p 556
Funding: JDC is supported by a Clinical Research Training Fellowship from the Medical Research Council.
Competing interests: None.
Ethics approval: Ethics approval was obtained from the Lothian Research Ethics Committee.