Article Text

Statistics from Altmetric.com
Tofacitinib is a novel inhibitor of Janus kinase (JAK) 3 and JAK1 is recently introduced as treatment for rheumatoid arthritis.1 The JAK inhibitors are at the focus of research in a myriad of other inflammatory diseases2 ,3 as the JAK-(signal transducer and activator of transcription) STAT pathway has a central role in cytokine signal transduction. We herein describe a case of refractory polyarteritis nodosa (PAN) successfully treated with tofacitinib.
A 28-year-old man had been diagnosed with PAN at age 14. He presented with livedo reticularis, arthritis and skin nodules with arteritis/fibrinoid necrosis confirmed on biopsy. Immunological panel at the time of diagnosis was negative for antineutrophil cytoplasmic antibodies, anti-nuclear antibodies, anti-Ro/SS-A antibodies, anti-La/SS-B antibodies, rheumatoid factor, with normal complement levels. He was treated with azathioprine and methotrexate for several years with drug-controlled complete remission. At age 24, his disease flared and he began to suffer from necrotic lesions of the scrotum and calves, excruciating abdominal pain and polyarthritis, with high C-reactive protein (CRP) levels (160–300 mg/L) for which he received recurrent intravenous methylprednisolone pulses and oral prednisone 40–60 mg daily between pulses. Numerous treatments, including: infliximab, adalimumab, rituximab, etanercept, tocilizumab, potassium iodide and cyclophosphamide intravenous and oral, failed to obtain remission. He was hospitalised for re-evaluation that included CT angiography of the chest and abdomen, echocardiography, viral serology, blood cultures, toxic screen, anti-infliximab antibodies and genetic mutation of adenosine deaminase 2, all of which were normal or negative.4 Treatment with plasma exchange for 3 weeks achieved partial remission, but had to be discontinued due to central line sepsis. At this point, he was in a severe long-standing inflammatory state for 3 years with high CRP levels, low albumin (3 g/dL) and ongoing leucocytosis treated only by prednisone 60 mg. Preliminary evidence for the role of JAK-STAT pathway in vasculitis has been recently published.5 Considering the use of tofacitinib, JAK1 and 3 activation were evaluated by phosphorylation of downstream STAT 3 following stimulation with interleukin 6 (IL-6) using mass cytometry (CyTOF), a single cell proteomics platform capable of simultaneously measuring the expression of up to 45 proteins at a single cell level in millions of cells. High levels of STAT 3 phosphorylation were detected specifically in CD4+ and CD8+ T cells subsets (figure 1). We initiated treatment with tofacitinib 10 mg twice daily that resulted in prompt normalisation of his CRP, albumin and leucocyte count, resolution of skin ulcers (figure 2) and relief of pain. Prednisone therapy was soon tapered from 60 to 10 mg daily. Re-evaluating the response of the JAK-STAT pathway to IL-6 stimulation after treatment confirmed attenuated response of the CD8+ T and CD4+ T cell resembling the healthy control (separate runs of CyTOF pretreatment and post-treatment were compared with the same healthy control) (figure 1). After 1 year of follow-up, the patient remains in complete remission on tofacitinib 10 mg twice daily and prednisone 10 mg. We have used IL-6 stimulation of STAT3, although the patient was not responsive to tocilizumab, as this is the standard method used to evaluate STAT3. Redundancy in the system and stimulation of the JAK-STAT3 pathway directly by stimulations that bypass the IL-6 pathway, such as toll-like receptor 4, 7 or 9, and IL-23 may explain the response to tofacitinib blocking downstream the pathway and not to tocilizumab.
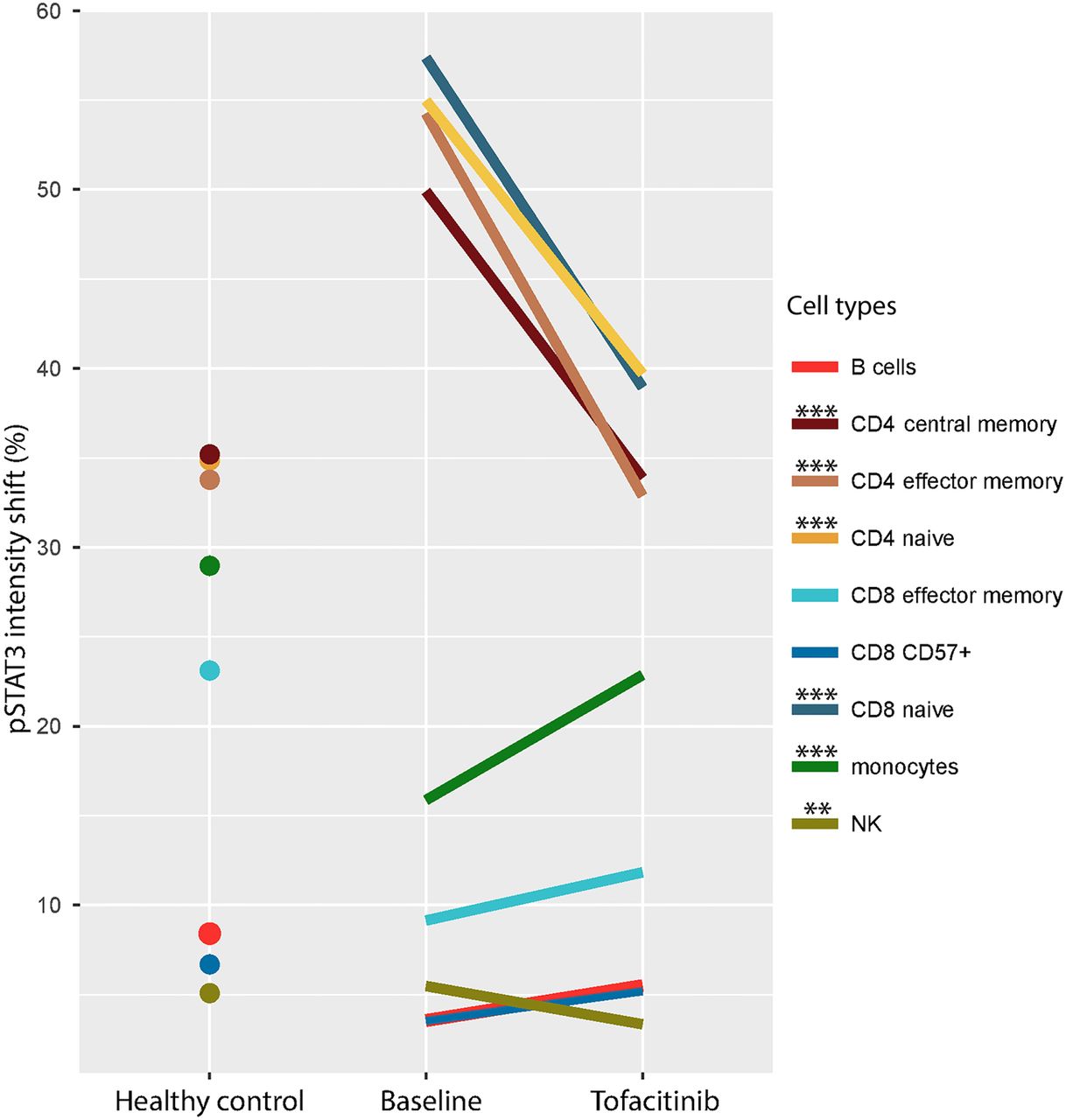
A striking reduction of signal transducer and activator of transcription (STAT)3 phosphorylation level in CD4 and CD8 T cell subsets upon initiation of tofacitinib therapy in peripheral blood of polyarteritis nodosa patient. Phosphorylation level of STAT3 was measured by intracellular staining with phospho-STAT3 metal-tagged antibody (phospho-flow). The response magnitude for each cluster was defined as the deviation of the pSTAT3 single-cell distribution between the two conditions (stimulated and unstimulated). We observed a major drop in the IL-6 induced STAT3 phosphorylation in CD4+ T cell subsets, naïve CD8+ T cells and natural killer (NK) cells under tofacitinib treatment (p< asterisk denotes significance of response magnitude difference between conditions by permutation ***<0.005, **<0.01) which coincided with a striking improvement of clinical signs. Post treatment with tofacitinib, p-STAT3 levels of this patient resembled those of a healthy control. Markers used to define cell populations: B cells: CD19+; naïve CD8+ T cells: CD3+CD8+CCR7+CD45RA+; effector memory CD8+ T cells: CD3+CD8+CCR7−CD45RA−; effector CD8+ T cells: CD3+CD8+CCR7−CD45RA+CD57+; naïve CD4+ T cells: CD3+CD4+CCR7+CD45RA+; effector memory CD4+ T cells: CD3+CD8+CCR7−CD45RA−; central memory CD4+ T cells: CD3+CD8+CCR7+CD45RA−; monocytes: CD33+CD14+; and NK cells: CD45RA+CD7+CD3−.
{kind=link}
{kind=link}
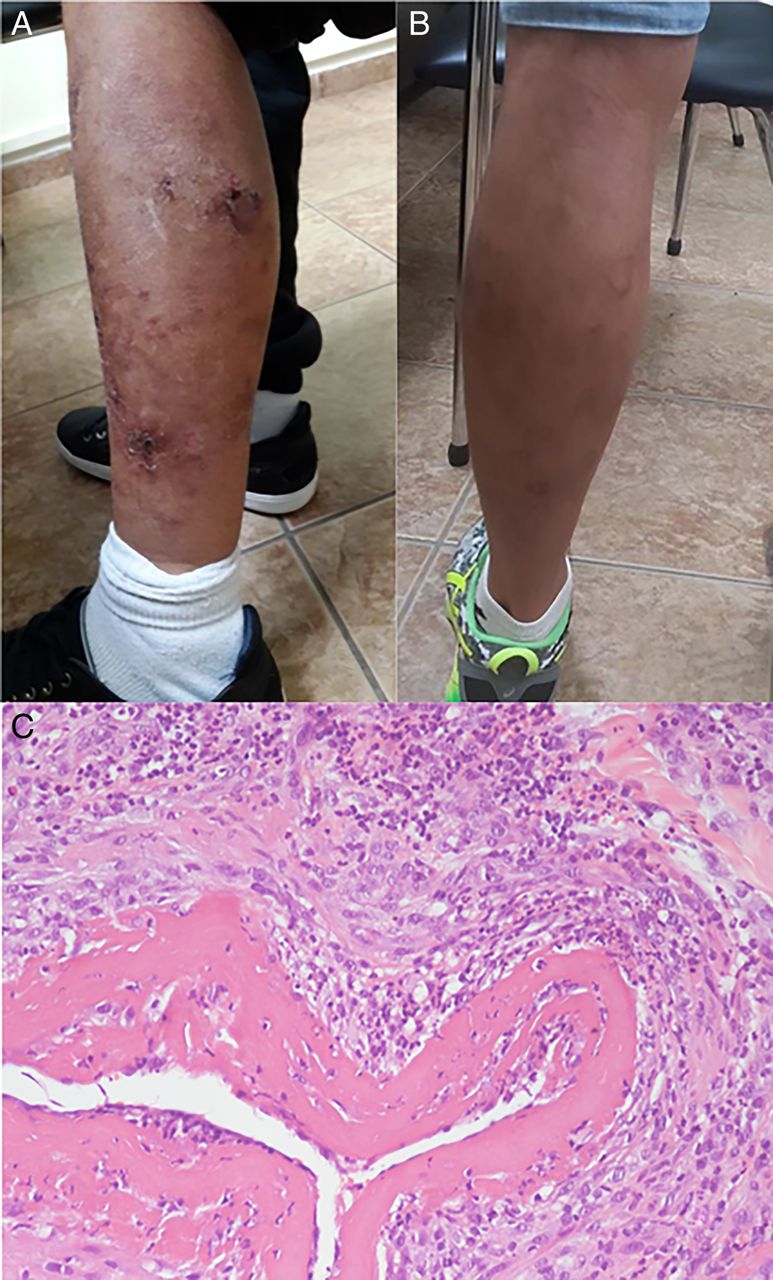
(A) Vasculitic skin ulcers on the calf of a patient with polyarteritis nodosa. (B) Resolution of skin ulcers after initiation of treatment with tofacitinib. (C) A skin biopsy (H&E, ×200) showing fibrinoid necrosis of arterial wall with residual nuclear dust and periarterial neutrophilic infiltration consistent with polyarteritis nodosa.
In conclusion, this is the first report in the literature of treatment of refractory PAN vasculitis with tofacitinib. Using high-resolution mass cytometry technology, we were able to tailor and monitor therapy.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.