Article Text

Statistics from Altmetric.com

Although neurophobia is a longstanding problem, it has only recently been given the name. In 1994, Jozefowicz, an American neurologist, described it as “a fear of the neural sciences and clinical neurology” held by medical students and doctors.1 This fear can lead to paralysis of thinking or action. Neurologists on both sides of the Atlantic will be familiar with referrals from medicine or psychiatry of patients with questions like “? organic brain ?”. Other patients, who have not previously been referred, but who clearly have neurological signs, have a clinical record in which the examination reads “CNS NAD”. Neurologists have come to infer that this acronym for “Nothing Abnormal Demonstrated” can equally mean “No Assessment Done”.
Fear of neurology and avoidance of the examination of the nervous system is not only a problem for hospital specialists. It pursues medical graduates when they go out to practice in the community. Epilepsy is one of the commonest neurological conditions managed by general practitioners (GPs).2 And patients generally prefer receiving epilepsy care mainly from their GP.3 Indeed, in the UK, the Department of Health endorsed the importance of monitoring epilepsy in general practice by payments which are linked to standards set by the Quality and Outcomes Framework.4 However, when Thapar et al surveyed GPs, they found that GPs rated as low their confidence and competence to manage this common condition.5 In interviews, GPs also expressed lack of confidence in managing other common neurological conditions, like Parkinson’s disease and headache.6,7 There is simultaneous evidence from patients that lack of confidence in neurology leads GPs to avoid providing advice on the social aspects of the condition—like fitness to work, driving and eligibility for benefits.6,8
It has been an in-joke among neurologists that outsiders feared their subject and so avoided practising it—a kind of inferiority complex. Schon et al suggested that some “neurologists … enjoy their subject’s reputation as one for which only young Einsteins need apply”.9 And a BMJ editorial suggested, tongue in cheek perhaps, that the archetypal neurologist was “a brilliant, forgetful man with a bulging cranium, and a loud bow-tie … who adores diagnosis and rare syndromes, and most importantly—never bothers about treatment”.10
THE BURDEN OF NEUROLOGICAL DISORDERS
Professional rivalry and stereotyping is an entertaining pastime. Some neurologists may cherish their reputation as the metaphorical brains of the profession on whose opinion others depend. However, seen from the outside, an ivory tower approach has disadvantages. Neurology problems are common in the population, with 10% visiting their GP for a neurology problem every year.11 The one year period prevalence of neurology problems has been calculated by sentinel practices for the UK General Practice Morbidity Survey (table 1): new and follow up consultations occur frequently for migraine, cerebrovascular disease, neuropathy, intervertebral disc disorders and epilepsy.2 GPs cannot very well ignore patients with these problems. About 20% of new referrals to UK neurologists are for headache, and about another 20% for loss of consciousness or epilepsy.12 Again in the UK, about 20% of adult medical admissions to a district hospital are for neurological problems, including stroke.13 Twenty eight per cent of all disability is secondary to neurological and psychiatric problems.14 Stroke is the third most frequent cause of death. Analysis of health trends (table 2) shows that other neurological problems, like dementia, head injury, brain tumour and Parkinson’s disease account for a considerable number of deaths in England and Wales.15 And so it goes on—a huge burden of symptoms, disorders and diseases.
The prevalence of consulting by disease group in a general practice population of 10000 per year
Neurological causes of death in England and Wales in 1993
NEUROPHOBIA IN PRACTICE, IN THE UK
If GPs feel they lack confidence and competence in managing common neurological problems, it is difficult to know whether neurologists seeing up to half of their new referrals for headache and loss of consciousness episodes is the right proportion, or case-mix. There is often a poor match between the clinical severity of conditions such as headache and epilepsy, and the likelihood of patients being referred to or staying in specialist care.16,17 Lack of ability to identify appropriate referrals would not be a problem if more patients could be referred to neurologists, that is if the threshold for referral was low. However, there is a lack of capacity with 5–10 times fewer neurologists in the UK, compared with other countries in Western Europe (fig 1).18 A low specialist-to-population ratio has led to bottlenecks in the availability of specialist services and more “neurology” problems have to be managed by other doctors. For example, GPs manage 97% of patients who consult for headache each year without referral.19 Lack of neurologist capacity is also associated with underprovision of teaching for undergraduates and medical postgraduates.

Ratio of neurologists to population in European countries. Reproduced with permission from Acute neurological emergencies in adults. London: Association of British Neurologists, 2002.4 Data were derived from Eurostat Annuaire 2000, a publication of the UEMS (Union Européenne des Médecins Spécialistes). Figures have not been given for Belgium and Germany because in those countries services are provided partly by neurologists and partly by neuropsychiatrists, so the numbers are not strictly comparable. There are no data for Finland and Spain.
In the context of the commonness of people presenting with neurological problems, a scarcity of specialists, and lack of neurology education for doctors outside neurology, neurophobia sustains a vicious circle.
WHAT IS THE CAUSE OF NEUROPHOBIA?
An important question becomes why have medical students and doctors become neurophobic in the first place? Is neurology education and training simply too short? Is it too unfocussed? Or is the problem the separation of basic neuroscience and clinical studies at medical schools? Arguments about the length of medical school courses in neurology beg the question “how much is enough undergraduate neurology teaching?” A survey in the US found that respondent medical schools provided 3–4 weeks of clinical neurology teaching.20 It has been difficult to gather similar information in the UK, partially because courses are taught in different parts of the curriculum and often neurologists are not able to accurately identify or lead what is provided.21
It may also be that teaching really has been unfocussed. To a certain extent the BMJ editor10 was probably right. Neurologists have in the past identified and named more disease categories than most other specialities. Patients with rare syndromes are more likely to be admitted to neurology wards simply because they are not easy to diagnose in outpatients. Medical students tend to learn by taking histories and examining these very people because they are available, a captive population—in hospital—on whom they can practice their clinical skills.
Traditionally, basic science, including neuroscience, has been taught prior to clinical teaching. The spatial orientation skills which are required in learning neuroanatomy are not something required for medical school entry. Prior examinations tend to focus on testing left-hemisphere functions. If spatial skills were a priority for medical school, Advanced Level Art might be a prerequisite. Attention to detail demanded by some neuroscience tutors, and lack of link-up with common clinical problems, may discourage future doctors, especially those who believe—wrongly—that neurological problems cannot be managed without a thorough knowledge of neuroanatomy and physiology. But students and teachers are gradually beginning to question this old chestnut. To borrow a metaphor “most people learn how to drive with limited knowledge of how the engine works”.9
Schon et al surveyed 345 students and doctors to explore the attitudes to neurology and neurophobia.9 Students and medical graduates viewed neurology as more difficult than other medical specialties. And the respondents judged themselves as having less knowledge of neurology, and less confidence in managing non-straightforward neurological complaints. Neurology was viewed as no more interesting than other subjects.9
In reviewing the literature, there seems to be a consensus that neurophobia is likely to develop at medical school, and even be caused by it. Medical education is a complex intervention. It is difficult to identify and change individual parts. However, in the context of a new curriculum, we aimed to lengthen the duration, and narrow the focus of neurology teaching in one school. We asked, could this prevent neurophobia?
COMBATING NEUROPHOBIA IN OUR UK MEDICAL SCHOOL
In 1999, the merging of the United Medical Schools of Guy’s and St Thomas’ Hospitals with King’s College, created the largest medical school in the UK (the GKT medical school), with about 400 students in each year group. A college-wide core curriculum was generated under the leadership of the Professor of General Practice. It was agreed that neurology would be taught in tandem with psychiatry over 13 weeks during the first clinical year. Students are divided into about 22 small groups of six learners for clinical teaching. There are between 20 and 30 neurologists, who visit the medical school on at least one or two days a week. Flexibility in scheduling teaching is possible, so that neurologists have first choice of teaching time, which they provide for 1½–2 hours each week for 13 weeks. This is facilitated by sharing teaching time with psychiatrists (there are 10 times as many psychiatrists as neurologists in the UK, and an even higher ratio centred at the Institute of Psychiatry, which is part of King’s College). This flexibility allows neurologists to fit teaching round their service work. Students spend an additional hour with a neurology resident each week. Students are also attached to clinics and have teaching by nurses, therapists, neurophysiologists, neuroradiologists and neurosurgeons. They have scheduled lectures, ward clerking and on-call. The full time equivalent of their neurology teaching is at least four weeks, spread over a 13-week term.
Neurologists agreed to cover core problems as defined in the new curriculum. The topics are similar to those recommended by the Association of British Neurologists (ABN)22 and include headache and migraine; epilepsy and loss of consciousness; movement disorders; transient ischaemic attacks and stroke; head injury; intracranial tumours; infections; inflammations; and peripheral neuropathies. The scientific rationale for teaching these topics was provided by drawing on figures for the frequency with which patients consult family doctors for neurological problems,2 and the frequency with which the population dies from preventable and non-preventable neurological diseases.15
Neurology teachers also agreed to teach and assess students using core neurology examining skills. The process of agreement on core skills was by a series of staff development sessions. Senior neurology staff undertook neurological examinations of each other, with an open forum, so all consultants and residents could contribute to the process. Staff presented their different examining practices, and there was vigorous debate. We were able to develop some consensus, and an improved esprit de corps. Residents found it an entertaining learning process watching the variation in technique displayed by their various mentors, who almost certainly believed their own methods were better than the rest! Core neurology examining skills were listed in the student handbook, and demonstrated on a videotape recording,23 so that all teachers and learners had access to them.
WAS NEUROPHOBIA REDUCED?
We monitored student assessment of teaching routinely in the middle and at the end of each 13-week term. Where assessment was not good, for example on outpatient teaching, we organised more staff development sessions, at which students provided feedback on what makes neurology teaching effective for them. Consultant-led teaching improved so that it was on average rated good to excellent. By 2002–3, the new curriculum had bedded down. So in the context of the debate about neurophobia,9 we contacted all 377 students in the year and asked them to compare their attitudes to neurology in relation to the other specialities taught in the same year, which are cardiology, endocrinology, gastroenterology, respiratory medicine and psychiatry. Students were asked to rate each subject on a scale of 1–5, where 1 was the lowest possible score and 5 the highest. For each question, the neurology mean score was compared to the mean score of all the other five specialist subjects. We used Schon et al’s questionnaire9 but added questions about students’ perceptions of their skills, and asked them to rank their preferences for postgraduate specialisation. We compared neurology mean scores with the mean scores of the other specialities combined using paired t tests. Differences were held as significant when p was less that 0.01.
We found that while medical students and graduates from a variety of schools in Schon’s study showed significantly less confidence in their knowledge of neurology, GKT students were as confident in neurology as they were in other specialities (fig 2). Schon did not ask about skills but our students’ self-rating of their skills was not significantly different from other specialities (fig 3). GKT students were similar to other students and graduates in perceiving neurology as more difficult than other subjects (fig 4), and stating they had less confidence in managing non-straightforward problems (fig 5). Gratifyingly, our students found neurology significantly more interesting compared to students and doctors surveyed by Schon (fig 6), and together with cardiology, it was rated highly as a preference for specialisation (fig 7).
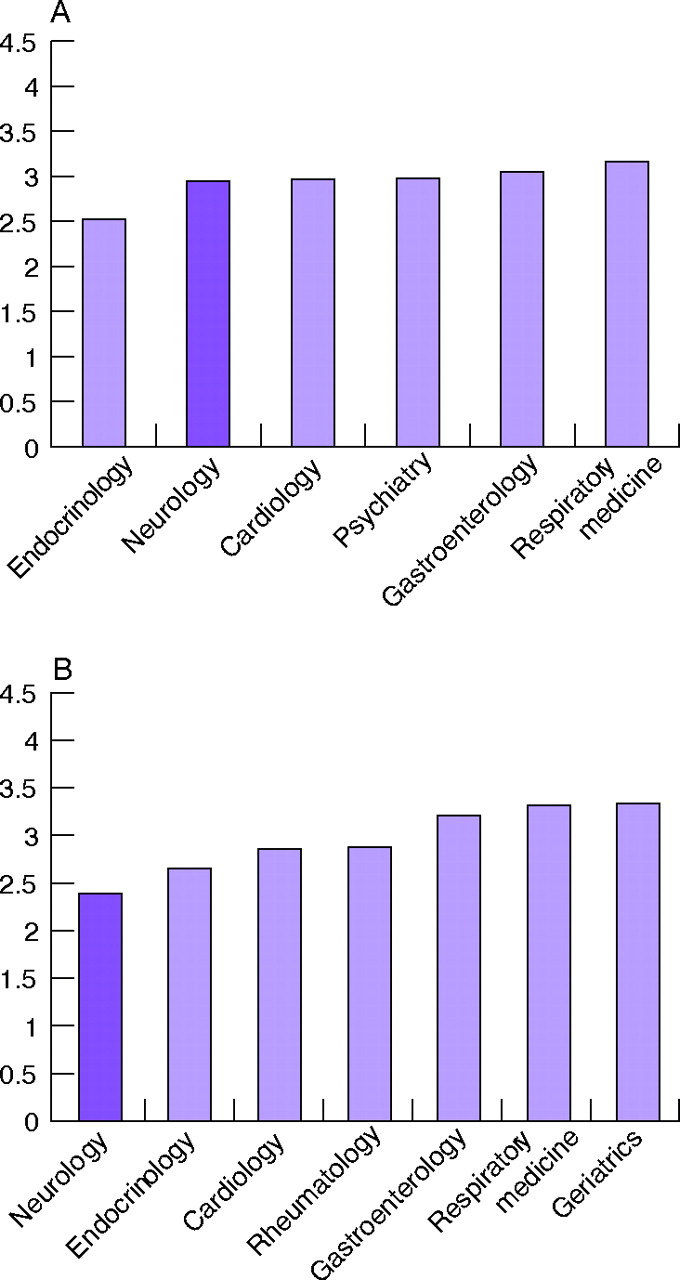
“What is your current level of knowledge?” Students’ mean response to question for each speciality. Comparison between present study (A) and findings of Schon et al9 (B).
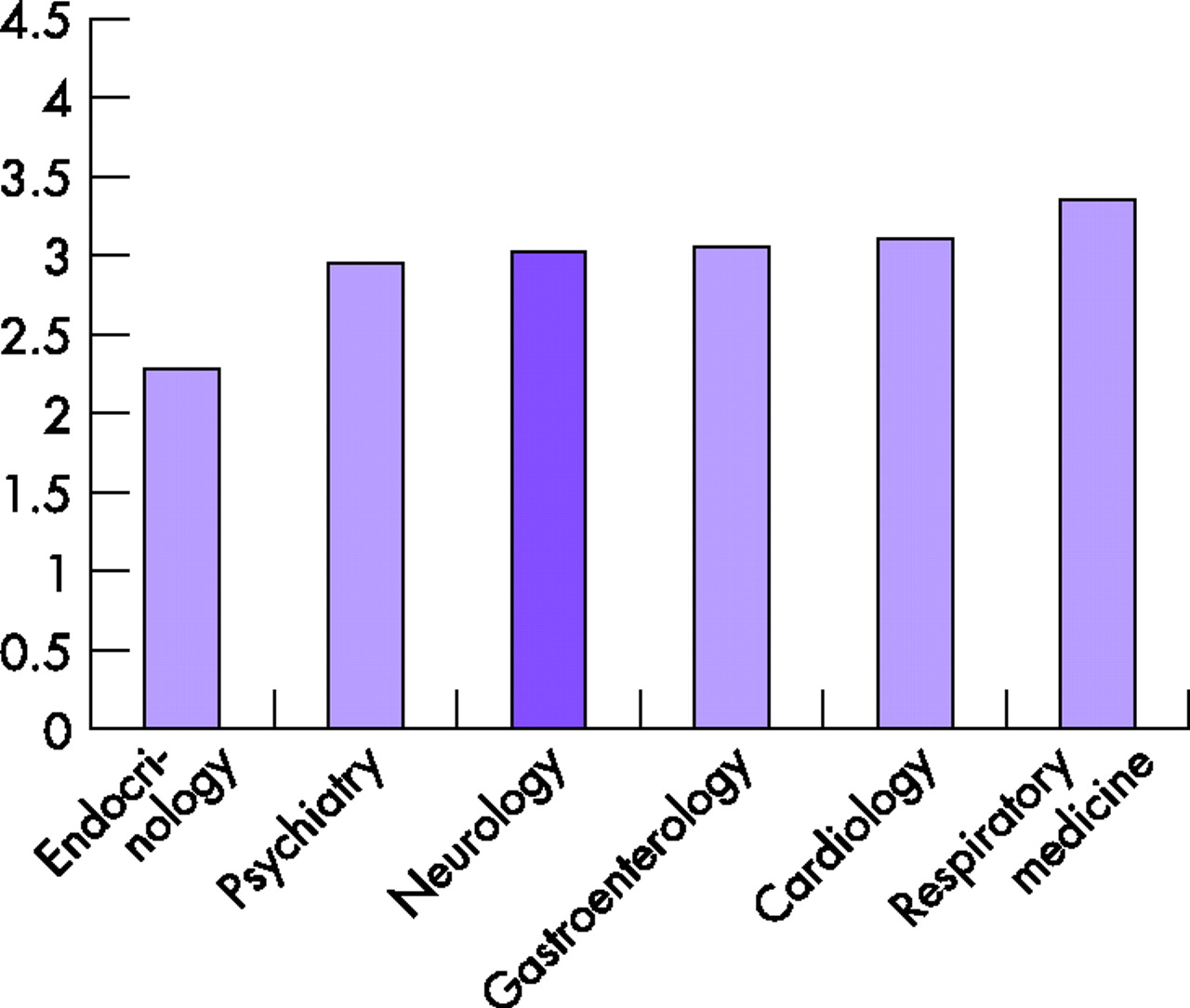
“What is your current level of skill?” GKT students mean response to question for each speciality.

“How difficult do you think the subject is?” Students’ mean response to question for each speciality, GKT (A) versus Schon et al (B).

“How confident do you feel when you see a patient with a not-straightforward complaint?” Students’ mean response to question for each speciality, GKT, (A) versus Schon et al (B).
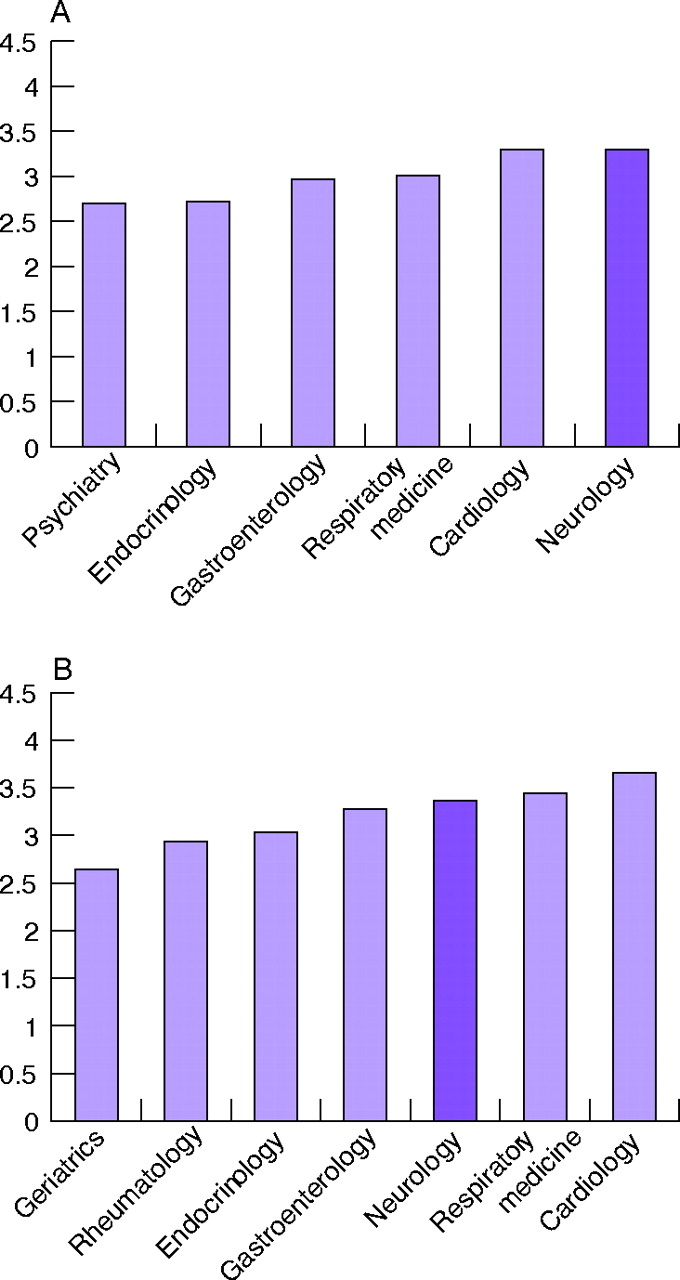
“What is your current level of interest in the specialty?” Students’ mean response for each speciality, GKT (A) versus Schon et al (B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
“Imagine you have to choose to specialise in one of these areas. Please rank tham in order of preference.” GKT students’ response to question for each specialty.
There were some gender differences; male students were more likely to report confidence seeing patients with a non-straightforward complaint, whatever the speciality. Male students had a significantly higher preference for specialising in cardiology, while female students had a higher preference for specialising in psychiatry. Despite being provided with the equivalent of four weeks’ teaching, when asked to suggest how clinical neurology learning might be improved, students suggested they wanted more bedside teaching, more outpatient clinics and more patient contact.
SO IS NEUROPHOBIA PREVENTABLE?
Reflecting back on the question of whether neurophobia is preventable, it is possible to revisit the putative causes in the light of some evidence. If neurophobia were due to education and training being too short or unfocussed, GKT has gone some way to providing a longer course, (4 weeks full time, spread over 13 weeks) which is focussed on core knowledge and skills. On the basis of our survey of student perspectives, it seems that the course has redressed some of the problem, with students perceiving their knowledge and skills in neurology as comparable to other subjects. However, students still rate neurology as being more difficult and lack confidence in managing non-straightforward problems. Despite a new curriculum, neuroscience at GKT is still taught quite extensively in the pre-clinical phase. Since 2004, this has been “topped and tailed” by clinical scenarios presented by neurologists. The effect of this has not yet been evaluated.
It is difficult to judge whether students’ lack of confidence in non-straightforward neurological problems compared to respiratory and gastroenterological problems is appropriate. Non-straightforward problems in neurology are challenging to everyone, and deserve respect. In the past, both teachers and students may have assumed that a focus on unusual problems would be more interesting than the workaday and mundane. And so it may seem a paradox that a course which aimed to teach common and core neurology knowledge and skills elicited more student interest in the subject. But then methods of teaching which focus on unusual problems may increase anxiety, and dampen the curiosity which fosters continuing learning.
Moving between theory and evidence is difficult. Students enter medical school with attitudes they have acquired in their family and society about, for example, the difficulty of neurology, the cachet of saving lives in cardiology, as well as any gender specific attitudes. Medical schools have only a part to play in fostering or challenging attitudes and behaviour.
Compared with other medical specialities, taking a skillful history and doing an examination takes longer and is more complex in neurology. Students who enter medical school and complete pre-clinical programmes have clearly demonstrated their ability in acquiring knowledge. However, they sometimes seem unprepared to spend time learning and practising skills. Time and feedback are important for this, as in learning to play tennis or football. It may be that students spending more time practising and staff developing a coaching relationship over a longish period for time is important to teach these core skills and prevent neurophobia. Rogers has emphasised the importance of personal relationships in learning.24 When student numbers rise and the curriculum is overcrowded, this can so easily result in relationships with teachers becoming more tenuous and limited. It suited GKT and the neurologists to offer a longer programme, shared mostly with psychiatrists. The process of learning with one neurologist over 13 weeks may have helped students to feel “good enough”.24
We feel cautious optimism that increasing the length and focus of neurology courses may prevent neurophobia in medical students, and so doctors. The ABN has produced new guidelines on neurology teaching at undergraduate level.26 Extending neurology postgraduate training for hospital trainees in their early years may help too. General practitioners have recently created specific training templates for neurology for future GPs.27
The BMJ editorial caricatured the neurologist as a “brilliant, forgetful man with a bulging cranium and a loud bow-tie” who “adores diagnosis and rare syndromes” in the same year that GKT launched its new curriculum (1999). Since then both the editor and the NHS have moved on. Neurology and neurology teaching need to change too, and influence for the better the attitudes of medical students and future doctors. Neurology may not be for the masses, but the perception of students that they have good enough knowledge and skills is a start.
REFERENCES
Linked Articles
- From the editor's desk