
Key point
Exacerbations of bronchiectasis requiring antibiotics are characterised by:
increasing sputum volume
increasing sputum purulence
increased cough, wheeze or systemic upset.
Key point
Diagnosis
Always pursue the cause of bronchiectasis as finding the cause may lead to treatment that slows or halts the progression of disease.
Treatment
It is essential that the patient’s sputum is sent for routine bacterial and mycobacterial microscopy and culture prior to starting antibiotics for exacerbations, although treatment should then not be deferred pending results.
Aetiology
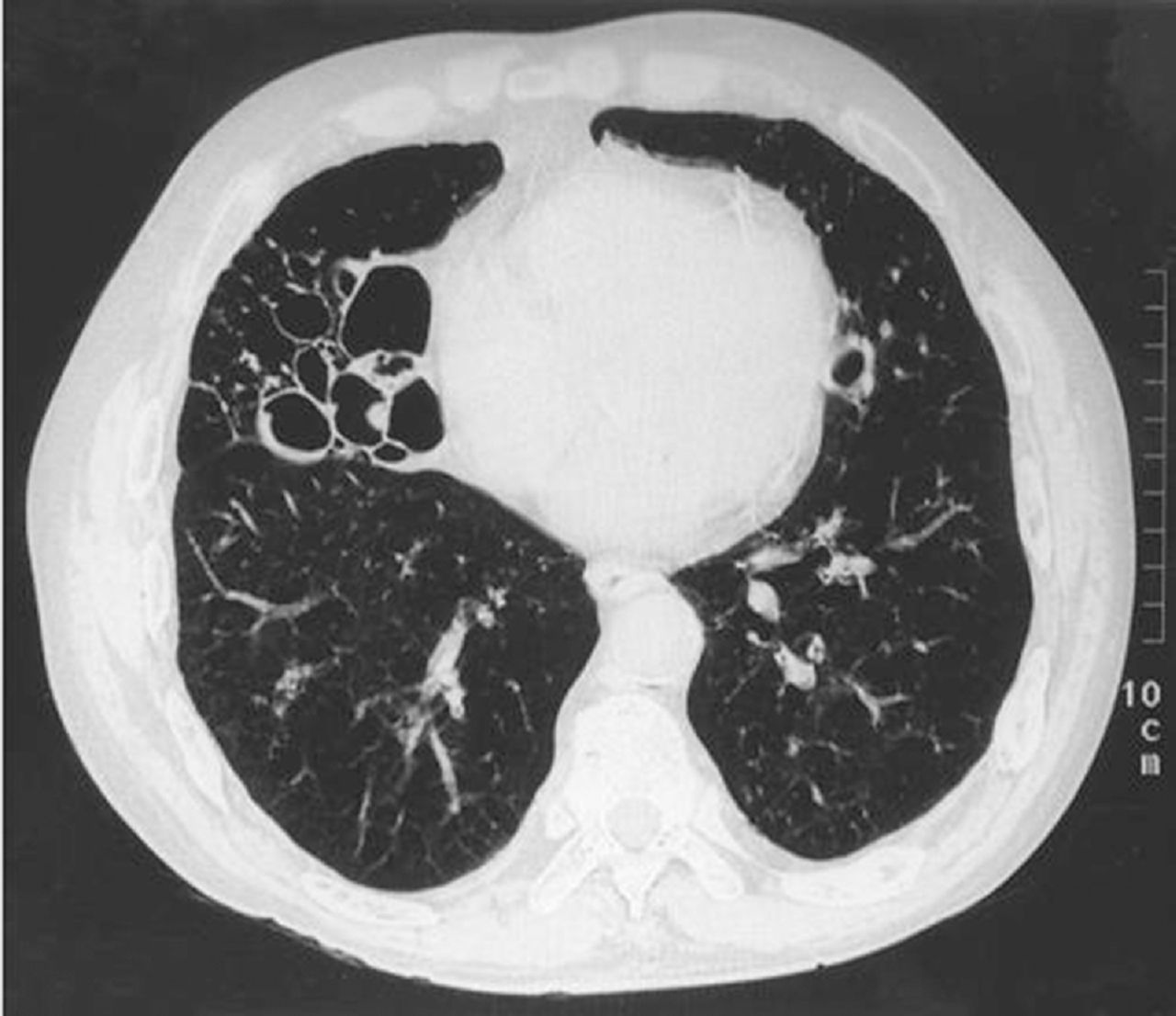
Bronchiectasis is a condition that is characterised by the permanent dilatation of bronchi (Figs 1 and 2) from a variety of reasons (Table 1). No definite cause of bronchiectasis is found in over 50% of patients.

Plain chest radiograph. The tramlines in the right lower lobe are consistent with bronchiectasis.
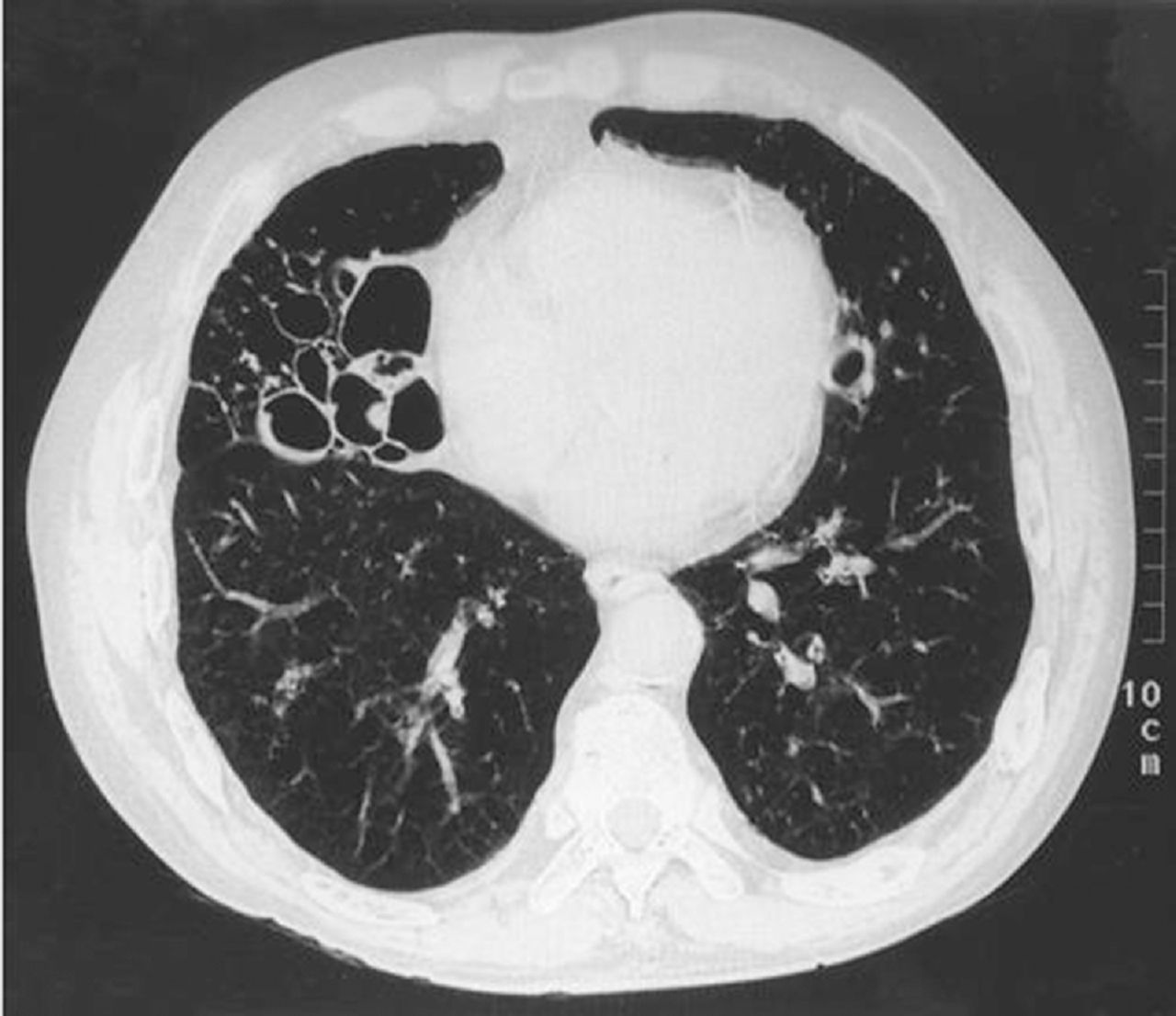
High-resolution CT chest scan. Gross bilateral bronchiectasis, more prominent in the right lung with a classic ‘signet ring’ appearance generated by an enlarged bronchus and a neighbouring vessel.
Causes of bronchiectasis
Pathology
Recurrent bacterial colonisation and infection lead to progressive airway injury that is mediated by neutrophils, T-lymphocytes and monocyte-driven cytokines. Released inflammatory mediators, elastase and collagenase lead in turn to the inflammation and then destruction of the elastic and muscular components of the bronchial walls, resulting in permanent bronchial wall dilatation.
Clinical presentation
The classic clinical manifestations of bronchiectasis are a cough and daily production of mucopurulent and tenacious sputum: less than 10 mL/day suggests mild bronchiectasis; more than 150 mL/day indicates severe bronchiectasis. Other symptoms are listed in Table 2.
Symptoms of bronchiectasis (frequency of occurrence)
Signs of bronchiectasis are shown in Table 3.
Signs of bronchiectasis (frequency of occurrence)
Investigations
Investigations are carried out to confirm clinical suspicion of bronchiectasis, identify any potentially treatable underlying causes, and assess any functional impairment and the extent of the bronchiectasis (Table 4).
Investigations in bronchiectasis
Microbiology
Patients with bronchiectasis usually experience recurrent respiratory tract infections. Prevention of infection and prompt treatment of acute infective exacerbations are cornerstones of management to minimise lung damage and maintain lung function.
Sputum culture should be obtained from patients with bronchiectasis in the stable state and at the time of exacerbation, prior to commencing antibiotics. Pathogens that can be cultured are shown in Table 5.
Pathogens cultured from sputum in patients with bronchiectasis
Treatment
Chest physiotherapy
This is the cornerstone of treatment, and it is advised that it should be performed at least twice daily. This includes postural drainage, active cycle of breathing techniques, and oscillating positive expiratory devices.
Adjuncts to sputum clearance
Nebulised saline (normal/hypertonic) assists mucus clearance. Mucolytics (eg carbocisteine) are often used to reduce sputum viscosity, although randomised trial evidence of benefit is limited.
Antibiotics for acute infections
Send sputum for culture. Start empirical antibiotics, treating for 14 days. Adjust antibiotic therapy directed by sputum culture findings if the patient is not responding. Consider intravenous antibiotics if the patient is very unwell, has not responded to oral antibiotics or has resistant organisms (often Pseudomonas).
Long-term prophylactic antibiotics
Consider long-term antibiotics if there are more than three exacerbations per year. Send sputum for microscopy, culture and sensitivity (MC&S) and mycobacterial culture. Select a regimen based on sputum microbiology. Macrolides may have anti-inflammatory, disease-modifying effects. Long-term nebulised antibiotics can be considered for patients chronically colonised with Pseudomonas (Colomycin/gentamicin/tobramycin).
Other medical treatments
Bronchodilators can be given if there is evidence of airflow obstruction. Inhaled corticosteroids are only indicated if there is coexistent asthma.
Interventional techniques
Bronchoscopy can be used for extraction of mucus (bronchial toilet) if physiotherapy has failed. Bronchial artery embolisation may be used to control severe haemoptysis.
Surgery can be used for symptomatic localised disease (but before doing so it is essential to rule out a systemic disease that may result in bronchiectasis affecting the remaining lung, eg immunodeficiency or aspiration), or massive haemoptysis.
Lung transplantation can be considered for end-stage bilateral disease, usually in patients with cystic fibrosis (CF).
Specific treatments
immunoglobulin replacement in common variable immunodeficiency
oral steroids and itraconazole in ABPA (there are no data on the efficacy of voriconazole or other imidazole agents in this condition)
gastric acid suppression and pro-kinetics for recurrent aspiration associated with gastro-oesophageal reflux disease (GORD).
recombinant human DNase (rhDNase) in CF.
Complications
common – recurrent infectious episodes, recurrent pneumonias and cor pulmonale
uncommon – massive haemoptysis, amyloidosis and brain abscess.
Prognosis
Depends on severity, bacterial colonisation (eg Pseudomonas colonisation might be associated with a poorer outcome) and the underlying cause. Deterioration may be due to recurrent and worsening sepsis, or to hypoxia and cor pulmonale.
Prevention
vaccination against measles, pertussis, influenza and TB
prompt treatment of bronchopulmonary infections and ABPA
early removal of foreign body and obstructing lesions.
- © Royal College of Physicians 2019. All rights reserved.








{kind=link}
{kind=link}