
In recent decades nutrition has moved from the periphery of medical care to a subspecialty in its own right. Provision of good nutrition is important to all specialties, but nutritional care has evolved from a somewhat eclectic discipline practised by enthusiasts to an independent subspecialty practised by a wide range of physicians and has now been incorporated into gastroenterological training.
Malnutrition is common in hospital inpatients, with about one-in-three considered at risk. An increasing body of evidence demonstrates improved outcomes for better nourished patients, as a result of enhanced muscle strength, immune function and wound healing, leading to reduced length of stay.1–4
Nutritional support encompasses a spectrum from the assurance that patients receive nutritious meals and assistance with eating if required, through oral supplement feeds and enteral tube feeding, to provision of parenteral nutrition (PN) in patients with intestinal failure (Fig 1).
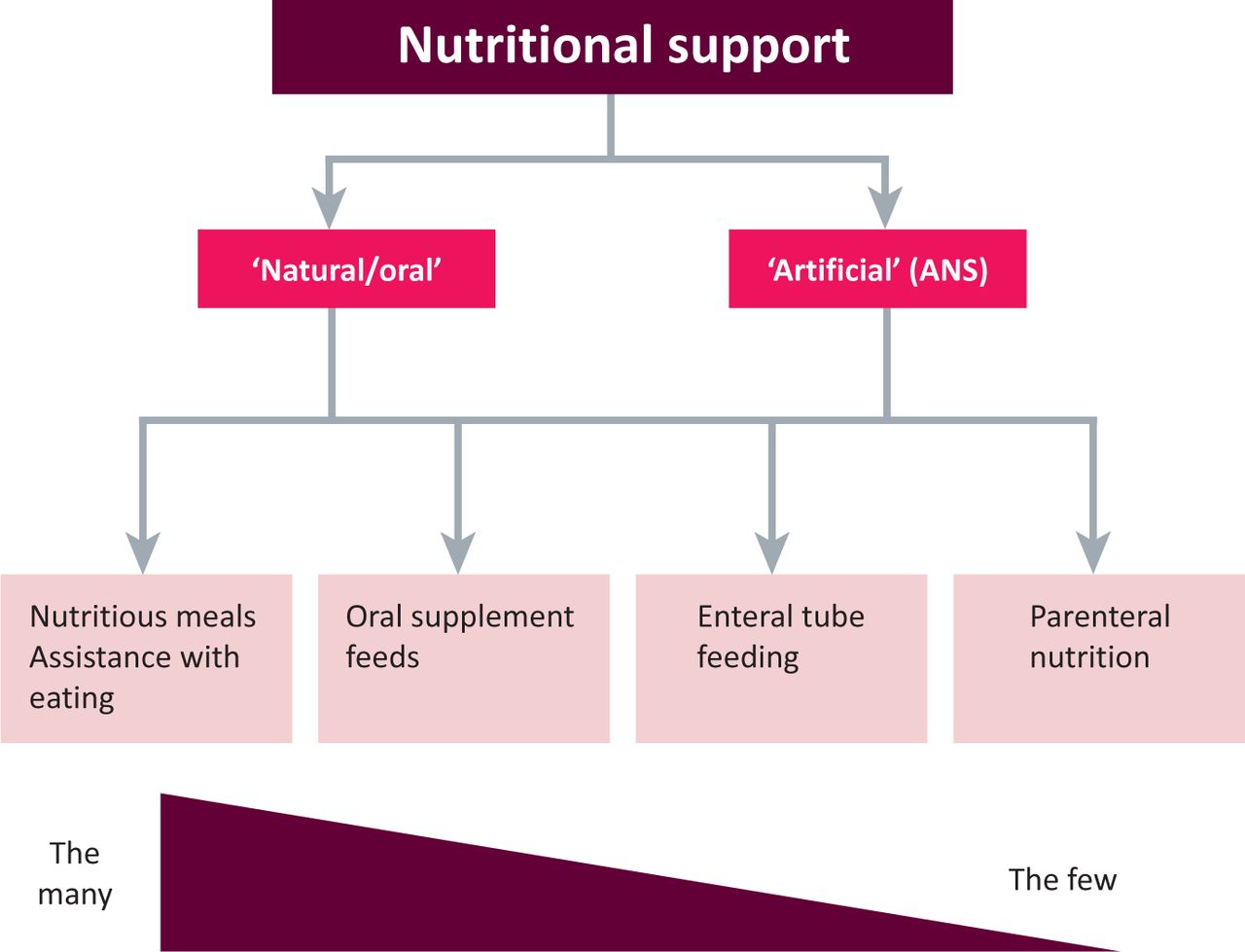
The spectrum of nutritional support, from ensuring that all inpatients receive and are able to eat nutritious meals, to providing parenteral nutrition for those with intestinal failure. ANS 5 artificial nutritional support.
The advent of nutritional support teams in many hospitals has greatly improved the management of patients with complex nutritional needs. However, these small teams are usually able to provide direct care only to the most complex cases requiring enteral feeding and those requiring PN.5 It is therefore vital that all clinicians develop a basic understanding of good nutritional care. This article presents some tips to help the general physician when considering nutritional aspects of a patient's care.
Who needs nutritional support?
Assessing and monitoring the patient
Weight and body mass index. Body mass index (BMI) provides an imperfect way of assessing nutritional status but is a useful guide. Patients with a BMI below 19 could be at risk of malnutrition. However, patients with a normal or even raised BMI may be nutritionally deplete if they have lost excessive weight or are lacking in vitamins and/or trace elements. Historical weight loss can be a better marker of impaired nutritional status, with unintentional weight loss of as little as 5% associated with worse clinical outcomes.6,7 Weight change during nutritional support in hospitalised patients can be a useful marker of the effectiveness of the intervention, but strict attention to fluid balance is required to militate the confounding effects of fluid gain.
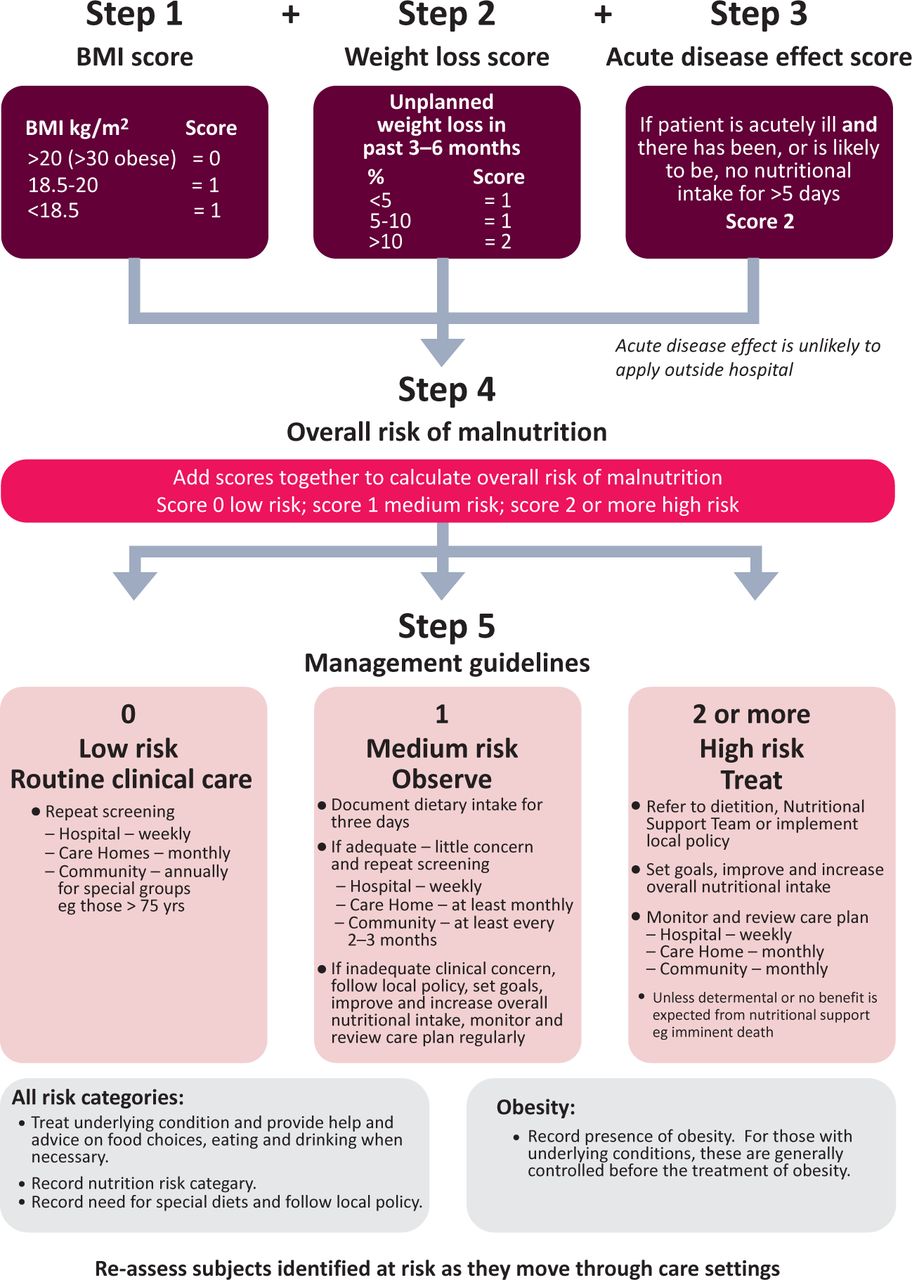
BMI and reported weight loss are integral to nutritional screening and both are utilised in the current favoured method of nutritional screening, the Malnutrition Universal Screening Tool (MUST), endorsed by many government agencies and professional bodies, including the British Association of Parenteral and Enteral Nutrition (Fig 2). The National Institute for Health and Clinical Excellence recommends that all patients admitted to acute hospitals should be screened at admission using this or a similar tool.8
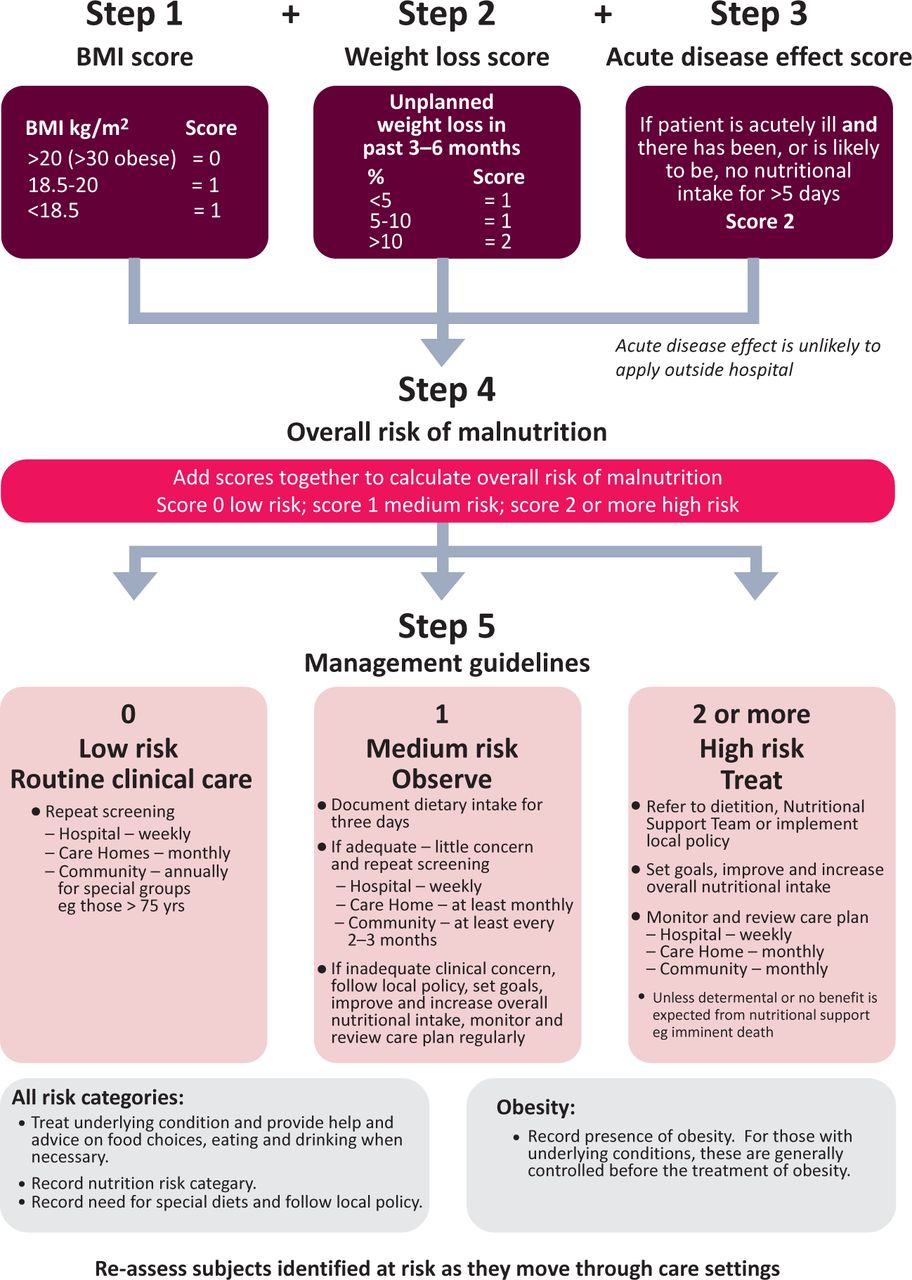
The Malnutrition Universal Screening Tool (MUST) (BMI 5 body mass index).
Biochemistry. To date, no reliable biochemical markers of malnutrition have been identified. Serum albumin is often erroneously referred to as a proxy for nutritional status, but changes in serum albumin usually relate to extravascular shifts in inflammatory states or altered synthetic function of the liver rather than being a true reflection of malnutrition – indeed, normal plasma albumin levels are seen in patients with profound anorexia nervosa.9
Key points
Good nutritional status improves clinical outcomes
All clinicians should be vigilant for, and able to recognise, patients who require nutritional support
All patients should have their nutritional status assessed on admission to hospital using a nutritional screening tool
When deciding on the mode of nutritional support the principle of ‘if the gut works, use it’ can usually be applied
Feed should be introduced cautiously in a nutritionally deplete patient, with careful monitoring and replacement of plasma phosphate, potassium and magnesium levels, and administration of supplemental thiamine
Measurement of water and fat-soluble vitamins can demonstrate deficiency, particularly in malabsorptive states, for example after bariatric surgery, but are often normal in individuals with poor nutritional status.10 Patients with severe malnutrition can have low levels of intracellular ions (including phosphate, magnesium and potassium) often becoming manifest only when nutritional support is commenced (see ‘Refeeding syndrome’).11
In practice, assessment should be based on a pragmatic approach using a combination of history, BMI and biochemistry to identify specific nutrient deficiencies.
Which patients require enteral tube feeding?
Oral supplements can provide adequate additional protein and energy to replenish body stores for most patients in hospital requiring nutritional support beyond normal dietary intake. Enteral tube feeding is reserved for patients unable to swallow food safely or if their energy intake remains inadequate.12 On occasion, tube feeding can be used to supplement oral intake in patients with high metabolic demands, for instance in patients with cystic fibrosis who are often unable to meet these demands with oral intake.
For short-term feeding (less than six weeks), nasogastric or nasojejunal feeding tubes usually suffice. Although nasal tubes can be tolerated for a longer time, it is usually preferable to place a direct gastrostomy or jejunostomy tube in suitable patients who do not tolerate nasal tubes, or require a longer period of enteral feeding. Postpyloric feeding, either via an endoscopically or surgically placed tube, may help for patients intolerant of intragastric feed (eg diabetic gastroparesis) or at high risk of aspirating stomach contents (eg post-stroke), although its benefit in improving outcomes remains contentious.13
Gastrostomy tubes are usually placed endoscopically using a ‘pull through’ technique (PEG) but can be placed under fluoroscopic guidance (RIG) using agastropexy technique. PEG placement is generally considered a quicker and easier technique, although RIG placement has the advantage of not requiring sedation or gastroscopy. There are often complex ethical issues around the merits of PEG feeding, particularly in patients in the later stages of dementia. Although not explicitly contraindicated, consensus opinion appears to be that enteral feeding is not beneficial in this group of patients for improving either their quality or duration of life.14
Which patients require parenteral nutrition?
The rule of thumb when deciding on the mode of nutrition is: ‘if the gut works, use it’. PN is therefore largely reserved for individuals with intestinal failure. PN is expensive and not without risk; it should be instituted only under the supervision of a nutrition support team. A recent enquiry by the National Confidential Enquiry into Patient Outcome and Death into the provision of PN in UK hospitals highlighted widespread inadequacies, particularly inappropriate use of PN and excessive complication rates.15
PN can be given via central or peripheral venous access. Peripherally delivered PN can cause thrombophlebitis and requires the use of PN of low osmolality, so larger volumes can be needed to meet energy requirements. This is not an optimum route of administration but means that PN can be started without the need to secure central access. The preferred central route for those requiring PN for weeks is via peripherally inserted central catheter lines, while tunnelled lines (eg Broviac or Hickman) are the optimum lines for long-term (more than three months) use.16
What are the risks of nutritional support?
Risk is inherent to any medical treatment and nutritional support is no exception. Risks can be divided into those related to biochemical excursions or fluid balance problems and those related to the methods of delivering the artificial nutrition.
Feed-related complications
Refeeding syndrome. Refeeding syndrome is characterised by precipitous drops in plasma levels of phosphate, potassium and magnesium, and can occur in individuals who have had inadequate oral intake for more than five days. Cautious gradual increases in calorific intake should be employed after appropriate restitution of electrolyte deficiencies. Overenthusiastic feeding of the malnourished patient orally, enterally or parenterally can lead to an insulin surge with large intracellular shifts of potassium, phosphate and magnesium, leading to low plasma levels of these ions. Daily measurement of these levels is therefore mandatory. Furthermore, increased thiamine use by cells during refeeding can provoke Wernicke's encephalopathy, so thiamine replacement should always be administered before feeding is started in patients at risk.8
Fluid and electrolytes
PN use can lead to derangements in fluid and electrolyte balance. Blood and strict fluid balance monitoring is required until the patient is stabilised on PN.8
Line- and tube-related complications
Tube feeding places patients at risk of aspiration, particularly in those with decreased conscious levels. Postpyloric feeding may help in high-risk individuals. Nasal tube complications usually relate to incorrect placement. All individuals placing and assessing tube position should be aware of current guidelines regarding checking tube position using pH testing, with chest X-ray where uncertainty remains.17 Gastrostomy tubes have many more complications, including bleeding or perforation at the time of placement, and infection after placement. These can often be averted by good aftercare.18
Central feeding catheters
Catheter-related sepsis (CRS) can cause morbidity or even mortality. There is good evidence that careful technique when handling these lines can obviate these complications.5 If CRS is suspected (eg fever or rigors on feeding), PN should be discontinued and simultaneous line and peripheral cultures taken. If line sepsis is confirmed, short-term temporary feeding lines should be removed while longer-term tunnelled lines may be salvaged with antibiotic therapy.16 Long-term feeding catheters can also provoke venous thrombosis necessitating long-term anticoagulation.
Conclusions
Nutritional care is an important part of good clinical care. All physicians should be mindful of, and be able to recognise, poor nutritional status in their patients. It is particularly important that nutritional care is not overlooked when managing patients with complex medical conditions, as these patients benefit most from good nutritional support. Although nutritional support is generally an intervention of high benefit and low risk, clinicians should be aware of, and be vigilant for, risks associated with feeding sick patients.
- © 2012 Royal College of Physicians








{kind=link}
{kind=link}