Article Text

Statistics from Altmetric.com
The human electroencephalogram (EEG) was discovered by the German psychiatrist, Hans Berger, in 1929. Its potential applications in epilepsy rapidly became clear, when Gibbs and colleagues in Boston demonstrated 3 per second spike wave discharge in what was then termed petit mal epilepsy. EEG continues to play a central role in diagnosis and management of patients with seizure disorders—in conjunction with the now remarkable variety of other diagnostic techniques developed over the last 30 or so years—because it is a convenient and relatively inexpensive way to demonstrate the physiological manifestations of abnormal cortical excitability that underlie epilepsy.
However, the EEG has a number of limitations. Electrical activity recorded by electrodes placed on the scalp or surface of the brain mostly reflects summation of excitatory and inhibitory postsynaptic potentials in apical dendrites of pyramidal neurons in the more superficial layers of the cortex. Quite large areas of cortex—in the order of a few square centimetres—have to be activated synchronously to generate enough potential for changes to be registered at electrodes placed on the scalp. Propagation of electrical activity along physiological pathways or through volume conduction in extracellular spaces may give a misleading impression as to location of the source of the electrical activity. Cortical generators of the many normal and abnormal cortical activities recorded in the EEG are still largely unknown. Spatial sampling in routine scalp EEG is incomplete, as significant amounts of cortex, particularly in basal and mesial areas of the hemispheres, are not covered by standard electrode placement. Temporal sampling is also limited, and the relatively short duration of routine interictal EEG recording is one reason why patients with epilepsy may not show interictal epileptiform discharge (IED) in the first EEG study.
If inappropriate questions are asked of the EEG, diagnostic errors will occur, and there will be poor yield of information that could be useful in the management of patients with seizure disorders. It is crucial to recognise that a normal EEG does not exclude epilepsy, as around 10% of patients with epilepsy never show epileptiform discharges. Secondly, an abnormal EEG demonstrating IED does not in itself indicate that an individual has a seizure disorder, as IED are seen in a small percentage of normal subjects who never develop epilepsy, and IED may also be found in patients with neurological disorders which are not complicated by epilepsy. Table 1 lists the areas in epilepsy diagnosis and management for which interictal and ictal EEG are useful, strongly so in some, but in a more limited way in others.
How can EEG help in epilepsy?
SPECIFICITY AND SENSITIVITY OF ROUTINE EEG
Epileptiform activity is specific, but not sensitive, for diagnosis of epilepsy as the cause of a transient loss of consciousness or other paroxysmal event that is clinically likely to be epilepsy. EEG has relatively low sensitivity in epilepsy, ranging between 25–56%. Specificity is better, but again variable at 78–98%. These wide ranges can be explained partly by diverse case selection and differences in clinical requirements for diagnosis of epilepsy in population studies of EEG specificity and sensitivity. Secondly, correlation between different EEG patterns and epilepsy varies, and only IED are associated with seizure disorders at a sufficiently high rate to be of clinical use. Abnormalities of background cerebral rhythms, focal slow activity or regional attenuation are much less specific than epileptiform activity, although they can indicate localised structural pathology underlying the seizure disorder, or diffuse cortical dysfunction as in symptomatic generalised epilepsies. Some types of epileptiform phenomena—3 per second spike wave discharge, hypsarrhythmia, and generalised photoparoxysmal response—are strongly correlated with clinical epilepsy, whereas focal sharp waves in centro-temporal or occipital regions have moderate association with clinically active epilepsy. Of children with centro-temporal or rolandic EEG discharges, only about 40% have clinically expressed seizures. Spikey or rhythmic phenomena such as 14 and 6 Hz spikes, phantom spike and wave, rhythmic mid temporal theta (θ), psychomotor variant and subclinical rhythmic epileptiform discharge in adults (SREDA), have low or zero predictive value for epilepsy. Misinterpretation of such non-epileptogenic phenomena, or overinterpretation of non-specific EEG abnormalities and spiky/paroxysmal variants of normal cerebral rhythms, are a common reason for over-diagnosis of epilepsy.1
How often and in which circumstances do non-epileptic subjects show IED in the EEG? In healthy adults with no declared history of seizures, the incidence of epileptiform discharge in routine EEG was 0.5%.2 A slightly higher incidence of 2–4% is found in healthy children and in non-epileptic patients referred to hospital EEG clinics. The incidence increases substantially to 10–30% in cerebral pathologies such as tumour, prior head injury, cranial surgery, or congenital brain injury3; particular caution is necessary when evaluating the significance of IED in such cases, and especially when the clinical history offers little support for a diagnosis of epilepsy.
A number of factors influence whether patients with epilepsy will show IED in the EEG. Children are more likely to than older subjects. IED is more likely to be found in some epilepsy syndromes or seizure types. The location of an epileptogenic zone is relevant: a majority of patients with temporal lobe epilepsy show IED, whereas epileptic foci in mesial or basal cortical regions remote from scalp electrodes are less likely to demonstrate spikes, unless additional recording electrodes are used. Patients with frequent (one per month) seizures are more likely to have IED than those with rare (one per year) attacks.4 The timing of EEG recording may be important: investigation within 24 hours of a seizure revealed IED in 51%, compared with 34% who had later EEG.5 Some patients show discharges mainly in sleep, or there may be circadian variation as in idiopathic generalised epilepsies. Co-medication may be relevant, particularly drugs that lower seizure threshold or may themselves induce epileptiform activity.
Improving the yield of interictal EEG
About 50% of patients with epilepsy show IED in the first EEG test. Yield in adults can be increased by repeating the routine EEG (up to four recordings), and in all ages by use of sleep studies. The combination of wake and sleep records gives a yield of 80% in patients with clinically confirmed epilepsy.6 Sleep EEG may be achieved by recording natural or drug induced sleep, using hypnotics which have minimal effect on the EEG, such as chloral or melatonin (the latter is not currently licensed in the UK). Whether sleep deprivation has additional value is difficult to establish from reported studies, although there is some evidence that it activates IED in idiopathic generalised epilepsies,7 and in practice, most patients achieve sleep reduction rather than true sleep deprivation.
Standard activation procedures of hyperventilation (up to three minutes) and photic stimulation (using published protocols) should be included in routine EEG recordings,8 but it is current good practice to warn patients of the small risk of seizure induction and obtain consent to these procedures.
Although potentiation of epileptiform discharge may occur up to 24 hours after partial and generalised seizures, there is insufficient high quality evidence that interictal EEG within this period increases the likelihood of obtaining IED.
Prolonged interictal sampling using EEG monitoring increases yield by about 20%, and is now more widely available through 24 hour ambulatory multichannel digital EEG.
USES OF EEG IN DIAGNOSIS OF EPILEPSY
EEG helps determine seizure type and epilepsy syndrome in patients with epilepsy, and thereby choice of antiepileptic medication and prediction of prognosis. EEG findings contribute to the multi-axial diagnosis of epilepsy, in terms of whether the seizure disorder is focal or generalised, idiopathic or symptomatic, or part of a specific epilepsy syndrome.
Focal and generalised seizure disorders show some overlap of both clinical and electrographic manifestations, and the entity of unihemispheric epilepsies blurs the boundaries further. However, the conceptual division of partial and generalised seizures/epilepsy types is still valid and clinically useful. In practice, the clinician will be reasonably certain about seizure type based on the account provided by the patient and witness. However, when history is unclear (un-witnessed “blackouts” or brief impairment of awareness), EEG can help distinguish between a complex partial seizure with focal IED, and an absence type seizure with generalised IED.
EEG FINDINGS IN EPILEPSY SYNDROMES
Many of the epilepsy syndromes associated with specific EEG features present in early life or childhood (table 2). Some syndromes are well accepted; others are controversial or may not be included in current International League Against Epilepsy (ILAE) classification systems because of insufficient data. These classifications are work in progress, and will increasingly be informed by developments in imaging, genetics, and molecular biology. In some individuals, the epilepsy syndrome may only become apparent over time, necessitating regular electro-clinical appraisal.
Epilepsy syndromes in early life
Idiopathic generalised epilepsies (IGE)
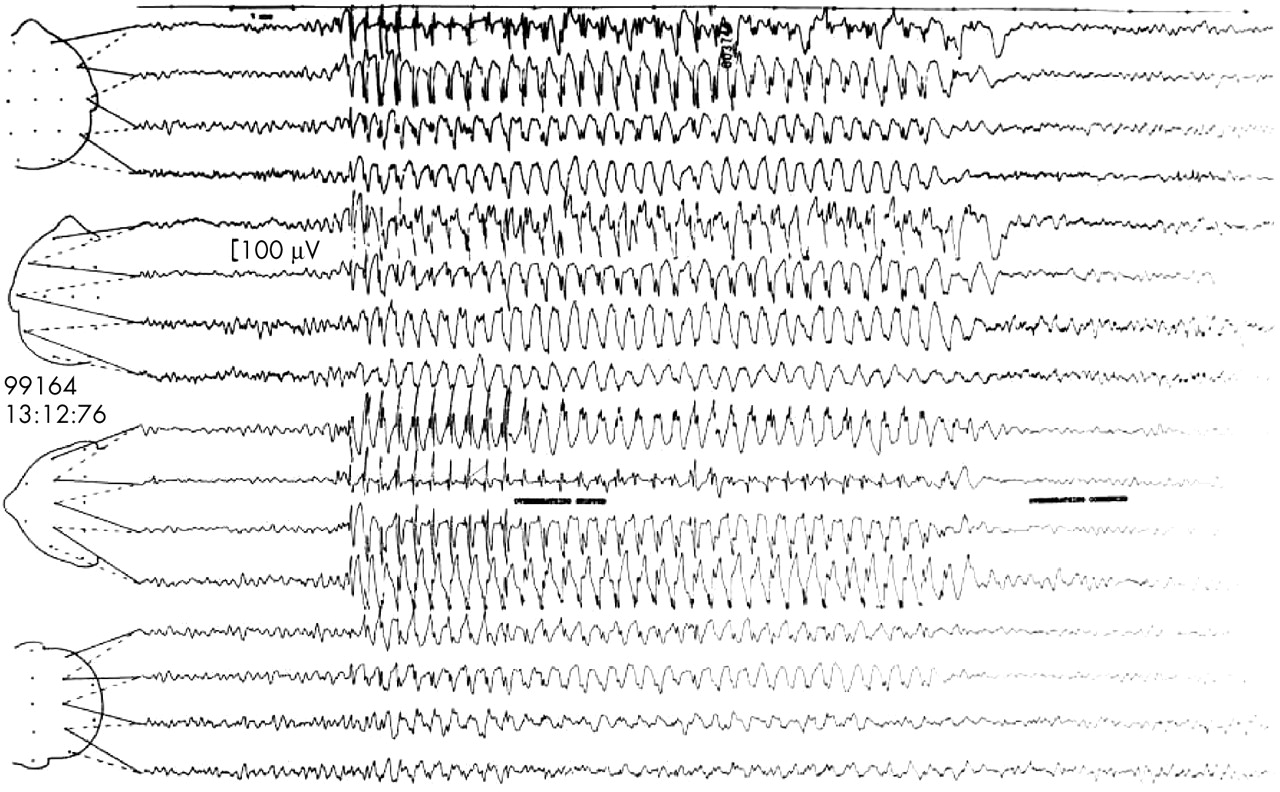
EEG characteristics in IGE include generalised spike or polyspike and slow wave discharge at 3–5 Hz, normal background cerebral activity, and a relatively high incidence of photosensitivity. Polyspike discharge tends to be associated with phenotypes in which myoclonus is prominent. In childhood absence epilepsy, the hallmark is bilateral synchronous 3 Hz spike wave usually lasting between 5–10 seconds, accompanying typical absence seizures (fig 1). The discharge is often slightly faster than 3 Hz at onset, and tends to slow down towards the end. The interictal EEG is normal, or may show runs of occipital rhythmic delta (15–40% of cases), persisting in some children after remission of absences. Photosensitivity is uncommon (< 10%), and may be a marker of poorer prognosis. Patients with juvenile absence epilepsy are more likely to show polyspike discharge or spike wave frequency above 3 Hz; runs of occipital rhythmic delta (δ) are not found. In juvenile myoclonic epilepsy, the interictal and ictal EEG characteristic is brief bursts of polyspike (sometimes single spike) and wave discharge. Variable asymmetry or lateralised emphasis of discharge is common, and interictal focal abnormalities are described in up to 40% of cases. Photosensitivity is also common (40–50%), and seizures may be induced by other reflex mechanisms including reading or praxis induction. Prominent polyspike wave discharge is also seen in eyelid myoclonia with absence epilepsy; absence status epilepticus seems to be relatively common in this syndrome. Generalised tonic-clonic seizures on awakening have no particular distinct EEG features.
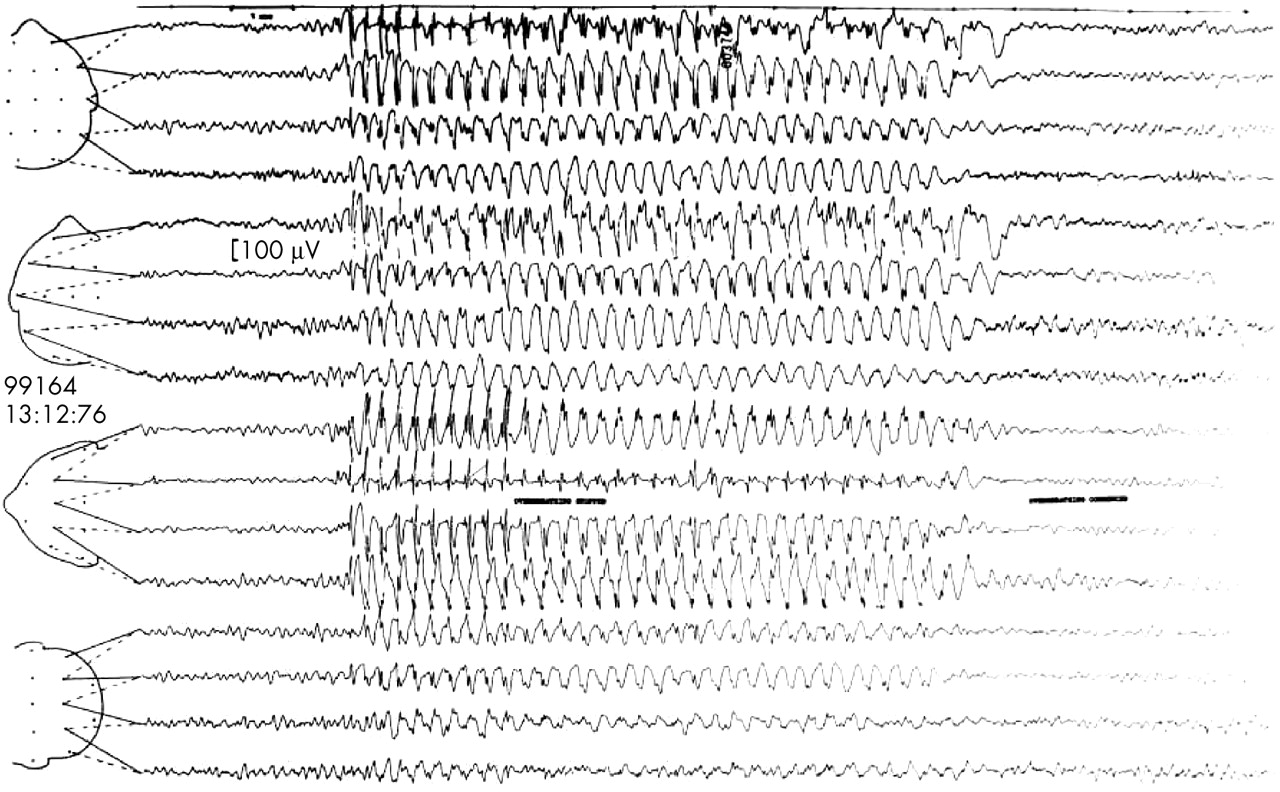
Three per second spike and wave discharge during typical absence seizure.
Differentiation between typical absence seizures and atypical absences
There is a continuum in both clinical and electrographic features of typical and atypical absences (AAS). However, AAS are usually associated with relatively slow (< 2.5 Hz) and less regular spike wave discharge, and background cerebral rhythms are abnormal, often notably so, in keeping with the symptomatic generalised epilepsies, such as Lennox-Gastaut syndrome, in which these absences occur.
Photosensitive epilepsy
Photosensitivity is found in about 5% of all epilepsies, usually IGE, but occurring also in progressive myoclonic epilepsies and rare cases of partial epilepsy. There is age related expression of photosensitivity: 75% of patients will have the first photic induced fit between the ages of 8–20 years.9 Photosensitivity is twice as common in females. Follow up studies have revealed that photosensitivity (and therefore risk of seizures) persists in the majority of cases, without age limit. Different types of photoparoxysmal response (PPR) have been described according to EEG distribution of discharge, and only generalised photoparoxysmal (spike wave) discharge is strongly correlated with clinical epilepsy. Acute symptomatic PPR can occur with abrupt withdrawal of alcohol or certain drugs, but is not associated with long term risk of epilepsy. Identification of photosensitivity in patients with epilepsy is important, to enable specific advice on avoidance of seizure triggers.
Benign childhood epilepsy syndromes
In benign childhood epilepsy with centro-temporal spikes (benign rolandic epilepsy), the EEG hallmark is high amplitude focal sharp wave discharges in the central and temporal regions, either bilateral or unilateral. A small percentage shows focal discharges in other regions or generalised spike wave. The discharges are potentiated by sleep. Background cerebral rhythms are normal. Interictal EEGs often show striking amounts of discharge, even though frequent seizures occur in only 20–25% of cases, and the EEG trait can be present without clinical expression. Benign childhood occipital epilepsy has more variable EEG findings; occipital spike wave paroxysms on eye closure (fixation off sensitivity) are characteristic of the early onset form, and multifocal discharges, rolandic spikes, and generalised spike wave are common.
Landau-Klefner syndrome (acquired aphasia and epilepsy) and electrical status epilepticus in sleep (ESES)
The hallmark of these disorders, which are probably related, is continuous spike wave discharge occupying 85% or more of the sleep record.
Progressive myoclonic epilepsies (PME)
Specific disorders manifesting as PME share common neurophysiological features—generalised spike wave discharge, photosensitivity, “giant” SEPs, facilitated MEPs with afferent stimulation, and abnormalities of background cerebral activity (excess slow activity). The latter are usually progressive, with most pronounced changes occurring in syndromes with significant dementia or cognitive decline, such as Lafora body disease. More specific findings are vertex sharp waves in sialidosis, occipital spikes in Lafora body, and giant VEPs in Batten’s disease (late infantile neurolipofuscinosis).
Partial epilepsy syndromes
Mesial temporal lobe epilepsy associated with unilateral hippocampal sclerosis shows anterior/mid temporal interictal spikes, which are ipsilateral or predominant over the pathological temporal lobe, and a characteristic rhythmic 5–7 Hz ictal discharge accompanying seizures (fig 2). In familial temporal lobe epilepsy, a relatively benign partial seizure disorder, focal IED is uncommon (20% of cases only). EEG findings are a defining feature of familial partial epilepsy with variable foci, which manifests as temporal and extratemporal seizures; the EEG focus is usually congruent with seizure type in individual cases. In autosomal dominant frontal lobe epilepsy, interictal EEG is often normal, and ictal EEG unhelpful or non-localising.

{kind=link}
{kind=link}
(A) Interictal focal temporal discharges in left mesial temporal epilepsy. (B) Ictal rhythmic θ discharge in left mesial temporal epilepsy caused by hippocampal sclerosis.
Does abnormal EEG predict seizure recurrence?
Subjects presenting with their first unprovoked seizure have a higher risk of seizure recurrence when the initial EEG shows unequivocal IED; if so, treatment should be offered after the first tonic-clonic seizure. In a systematic review,10 the pooled risk of recurrence at two years was 27% if the EEG was normal, 37% if there were non-specific abnormalities, and 58% if epileptiform activity was present.
Strategy for EEG investigation in a newly presenting case of epilepsy
The recently published National Institute for Clinical Excellence (NICE) guidelines for diagnosis and management of the epilepsies in adults and children11 recommend that an EEG should be performed to support a diagnosis of epilepsy in adults in whom the clinical history suggests the seizure is likely to be epileptic in origin. In children, EEG is recommended after the second or subsequent seizure (studies having shown that yield of information gained from EEG after a first seizure was too low to affect treatment decision). Individuals requiring an EEG should have the test performed within four weeks of request. This latter good practice guideline will seem unachievable by many UK neurophysiology departments. However, EEG referrals can be stratified at the time of receipt, and a reduction in requests for unnecessary routine EEG tests in patients with established epilepsy (see below) would help ease service pressures.
The Scottish Intercollegiate Guidelines Network (SIGN)12 recommend EEG for young people with generalised seizures to aid classification and to detect a photoparoxysmal response. Some caution is required when setting age limits to EEG investigation in adults, as idiopathic generalised epilepsies can present beyond adolescence.13 Late onset IGE has the same electroclinical features as younger onset cases,14 and the diagnosis will be missed if EEG is not requested, in the assumption that all new onset generalised seizures in adults are secondary to partial epilepsy.
EEG AND MANAGEMENT OF EPILEPSY
Interictal EEG has limited use in chronic epilepsy, particularly if well controlled or in remission. There is only a weak association between the amount of IED and seizure frequency, and antiepileptic medication has variable effect on the amount of epileptiform discharge. There is no value in repeating the routine EEG if seizures become more frequent, or to assess treatment effect, with the exception of idiopathic generalised epilepsies in which persistent IED or PPR would suggest suboptimal treatment in patients taking sodium valproate or lamotrigine. In general, “treating the EEG” is unnecessary, although there is emerging evidence that suppression of interictal discharges which cause transient cognitive impairment may improve school performance in some children.
Prediction of seizure relapse after withdrawal of antiepileptic drug treatment
The role of EEG is controversial, and it is uncertain which aspect(s) of EEG may be important (non-specific abnormality versus IED, prior or persisting abnormality, de novo appearance of IED during the course of or following drug withdrawal). The relative risk of relapse if the EEG is abnormal ranges from 0.8–6.47 in published studies,15 some of which cover children and adults, or a range of seizure types and epilepsy syndromes. EEG is probably more useful for prediction of seizure relapse in children than adults, and otherwise for identification of epilepsy or seizure types that carry a high risk of relapse, such as photosensitivity, juvenile myoclonic epilepsy, or symptomatic seizure disorders.
Cognitive change
Acute and subacute cognitive decline or confusional states in epilepsy may be due to frequent subtle/clinically unrecognised seizures; perhaps a pronounced increase in IED; a metabolic or toxic encephalopathy; or non-convulsive status, and EEG will help in the differential diagnosis. However, recognition of acute encephalopathies or non-convulsive status can be difficult in severe symptomatic epilepsies because of similarity in interictal and ictal EEG patterns. Chronic cognitive decline may be due to a progressive disorder underlying the epilepsy, or an unassociated neurodegenerative process. EEG can confirm an organic brain syndrome by demonstrating a deterioration of background EEG activity, but will not discriminate as to cause. Epileptic encephalopathy—a condition in which epileptiform abnormalities are believed to contribute to progressive disturbance in cerebral function—is an emerging concept, particularly in childhood epileptic syndromes. As yet, there are no widely agreed or clear definitions as to the essential EEG features.
Long term EEG monitoring
Long term video or ambulatory EEG has an important role in the assessment of patients who present diagnostic or management difficulties following clinical evaluation and routine EEG. The clinical applications of EEG monitoring are:
-
diagnosis of paroxysmal neurological attacks
-
differentiation between nocturnal epilepsy and parasomnias
-
diagnosis of psychogenic non-epileptic seizures
-
characterisation of seizure type
-
quantification of IED or seizure frequency
-
evaluation of candidates for epilepsy surgery.
Ambulatory EEG is most suitable when concurrent synchronised video to document clinical features is not essential, or for monitoring in an outpatient setting or specific environment. Inpatient video EEG telemetry is expensive and labour intensive, and a limited resource. Specialised telemetry units have the advantage of dedicated ward based staff, experienced in the identification of subtle clinical events, and close management of patients during seizures. Duration of study depends on frequency of attacks; in practice, long term EEG monitoring is unlikely to be productive if the patient’s events occur less than once per week. Methods to increase likelihood of seizures include antiepileptic drug reduction (utilising specific protocols, and best reserved for pre-surgical evaluation) and provocation techniques. There is a risk that provocation by suggestion may lead to false positive results particularly in psychogenic non-epileptic seizures, and use of other techniques such as saline injection or alcohol swabs carries ethical difficulties.
Long term monitoring generates very large amounts of data for analysis, which can be reduced by use of commercially available spike and seizure detection algorithms (accepting these may underestimate or overestimate relevant events). There is current research interest in methods that anticipate or predict seizures, by detection of non-linear changes in EEG data at least several minutes before an epileptic seizure. Specificity and sensitivity of these methods has not been fully evaluated, and their clinical role is as yet uncertain.16
In partial epilepsies, the most important ictal EEG changes for seizure localisation are those that occur within the first 30 seconds after the seizure onset. Broadly speaking, localised changes are more common in temporal lobe epilepsy than in extratemporal seizures, and epileptiform or high frequency discharge is more likely to occur in neocortical epilepsy, particularly if the focus is relatively superficial. In mesial temporal epilepsy, the typical ictal onset pattern is a rhythmic θ (5–7 Hz) discharge localised to the anterior mid temporal lobe, with up to 80–90% of patients showing such change. In lateral temporal seizures, ictal onset EEG changes are usually lateralised, and more likely to have a repetitive epileptiform appearance than mesial temporal seizures. Frontal lobe epilepsy ictal EEG onset patterns are most often generalised or widespread, comprising high frequency activity or slow rhythms or attenuation. Localised changes are rare, for a number of reasons—inaccessibility of much of the frontal lobes to scalp electrodes, widespread anatomical connections, likelihood of bifrontal damage in post-traumatic frontal epilepsy, and variability in size and distribution of epileptogenic regions. Interictal discharges in frontal lobe epilepsies are often generalised or non-localised for similar reasons. Ictal EEG changes may also be obscured by the hypermotor clinical manifestations of FLE. Ictal onset EEG patterns in parietal and occipital seizures vary, in part dependent on pathways of seizure propagation. Localised and lateralised ictal onset may occur, particularly in non-mesially sited epileptogenic foci. However, the rate of false localisation and lateralisation is highest in these two seizure types, thus limiting the role of ictal recording in parietal and occipital lobe epilepsy.
Scalp EEG commonly shows no change in simple partial seizures, because the focal ictal discharge is distant or deep, or involves too small a neuronal aggregate for synchronised activity to register on the scalp. This is unfortunate given how difficult diagnosis of simple partial seizures can be on clinical grounds.
Role of neurophysiology in evaluation of patients for epilepsy surgery
Interictal and ictal EEG remain pivotal in pre-surgical assessment, although their role has evolved with the advent of high resolution volumetric magnetic resonance imaging (MRI) and other imaging techniques. The importance of neurophysiological investigation also depends on the surgical procedure. It is high in resective surgery (lesionectomy, lobectomy) and multiple sub-pial transection, moderate in hemispherectomy, and low in callosotomy or vagal nerve stimulation, except to exclude the possibility of a resective procedure.
Most candidates for epilepsy surgery can be adequately investigated by scalp interictal and ictal EEG. The purposes of neurophysiological assessment are:
-
to confirm that the individual has epileptic seizures (4–10% of patients in surgical programmes have co-morbid psychogenic non-epileptic seizures; if untreated before surgery, non-epileptic attacks often become more florid and present a major management problem)
-
to characterise electroclinical features and establish whether these are concordant with other data (MRI, functional imaging, psychometry)
-
to demonstrate epileptogenicity of the presumed pathological substrate of refractory epilepsy
-
to identify possible other epileptogenic foci
-
to assess cortical function when pathology is in or close to eloquent cortex.
Some patients require invasive neurophysiological studies. The proportion who do in a given epilepsy surgery centre depends on complexity of case mix, availability of non-invasive localising investigations such as SPECT, PET, MEG, and fMRI-EEG, and to some extent the traditional practice of the centre. Invasive EEG utilises depth electrodes (inserted surgically under stereotactic MRI guidance) and subdural electrodes (strips or grids, the latter requiring craniotomy for placement). Cortical stimulation can be performed with either type of electrode. Electrode selection and placement is determined by the location of the epileptogenic zone. In general, wider areas of cortex are covered by subdural electrodes; depth electrodes are more suitable for deep lying foci, but have the disadvantage of sampling only small areas of brain. The risks of invasive EEG—infection, haemorrhage, cortical damage—depend on electrode type and number. The main indications for invasive EEG are dual or possibly multiple potential epileptogenic pathologies, bilateral hippocampal sclerosis, and focal lesions in eloquent cortex. Invasive EEG might also be offered to a patient with no underlying structural pathology identified on neuroimaging, but in whom other investigations have generated a plausible hypothesis as to location of the epileptogenic region.
The number of seizures that need to be recorded, and thus length of study, in either scalp or invasive EEG video telemetry depends on type of epilepsy and findings in other investigations, particularly MRI. Video EEG telemetry may be unnecessary if there is strong concordance of interictal scalp EEG with other investigative modalities. Some centres have reported good outcome after temporal lobectomy in small series of unilateral hippocampal sclerosis evaluated by interictal EEG without seizure recording.
EEG AND STATUS EPILEPTICUS
EEG is essential for correct diagnosis and management of status epilepticus, and ideally there should be 24 hour availability of reported EEG with monitoring facilities. However, under-provision of neurophysiology services in the UK means that many district general hospitals have no on-site EEG machine or appropriately trained staff. The minimum standards should be EEG within 12–24 hours for admissions with uncontrolled seizures or confusion, EEG before or during transfer to ICU, and trained staff able to report data.
In convulsive status epilepticus, EEG is used diagnostically to confirm that the patient has status and not pseudostatus, in which ictal EEG is normal,17 and to differentiate causes of obtundation—continuing seizures, drug induced coma, or encephalopathy. Electrographic monitoring to control and guide treatment is essential once general anaesthesia has been induced, as clinical manifestations of ongoing seizure activity may be subtle or absent, regardless of whether paralysing agents or sedating drugs are administered. What constitutes a satisfactory electrographic end point of treatment is uncertain. Burst suppression is commonly used, but levels of anaesthesia to achieve this may not be tolerated by the patient. Seizure suppression might be sufficient, although this is less easy to define, and distinction between seizure activity per se and merging of frequent epileptiform discharge can be difficult. When evaluating the clinical use of EEG monitoring in status, it has to be accepted that there are no studies that demonstrate that EEG monitoring independently improves outcome in convulsive status epilepticus. EEG can contribute prognostic information: continuing electrographic status is associated with worse outcome in convulsive status,18 and some studies have shown that periodic epileptiform discharges are associated with poorer outcome independent of aetiology of status.19
The term non-convulsive status epilepticus (NCSE) covers a range of conditions, with variable clinical features, and pathophysiological, anatomical, and aetiological bases: generalised absence status, de novo absence status, simple partial status epilepticus, complex partial status, electrographic status with subtle clinical manifestations, and electrical status epilepticus in sleep. EEG manifestations reported in NCSE include continuous or virtually continuous spike wave discharge, discrete focal electrographic seizures, diffuse slow activity with or without spikes, and periodic or repetitive epileptiform discharges. Complex partial status in patients with existing epilepsy is relatively benign, probably under-recognised, and readily diagnosed on clinical grounds. Most other clinical situations in which NCSE occurs require EEG for diagnosis, which can be confirmed if the EEG shows continuous or virtually continuous paroxysmal activity, and preferably improvement simultaneous with clinical response to anticonvulsant medication such as intravenous/oral benzodiazepines. Electrographic diagnosis is relatively easy in generalised absence status (de novo absence status of late onset, or in patients with existing/previous IGE), in which there is a prolonged state of altered consciousness associated with generalised 3 Hz spike wave EEG activity. EEG confirmation is also usually straightforward in persistent electrographic status after control of convulsive status, and in children with ESES. More problematic are cases of simple partial status, in which the EEG is unchanged or non-specific; or the patient with acute cerebral damage (caused by anoxia, infection, or trauma) whose EEG shows frequent or continuous abnormalities which may be due to the primary pathology per se; or those with epileptic encephalopathy who have clinical symptoms suggestive of NCSE, but show similar ictal and interictal EEG patterns. For these situations, internationally agreed criteria for EEG diagnosis of NCSE are needed urgently.