Article Text

Statistics from Altmetric.com
- push enteroscopy (PE)
- capsule endoscopy (CE)
- double balloon enteroscopy (DBE)
- gastrointestinal (GI)
- obscure gastrointestinal bleeding (OGB)
CONTENTS
1.0 Introduction
2.0 Formulation of guidelines
2.1 Grading of recommendations
2.2 Scheduled review
3.0 Summary of recommendations
4.0 Types of small bowel enteroscopy
4.1 Enteroscopy using a colonoscope
4.2 Sonde enteroscopy
4.3 Push enteroscopy
4.4 Intraoperative enteroscopy
4.5 Double balloon (push and pull) enteroscopy
5.0 Capsule endoscopy
5.1. Technique
5.2 Indications for capsule endoscopy
5.3 Complications of capsule endoscopy
5.4 Patency capsule
6.0 Service provision and training
References
1.0 INTRODUCTION
The small bowel has historically been a difficult area to examine due to its anatomy, location and relative tortuosity. Examination beyond the duodenojejunal flexure is of importance in a number of small bowel disorders. Before the advent of enteroscopy or capsule endoscopy, radiographic studies had been the main investigative modality of the small bowel. Barium follow-through and enteroclysis permits indirect examination of the small bowel but has a low diagnostic yield particularly in the context of obscure gastrointestinal bleeding.1–3
Capsule endoscopy and enteroscopy are now the preferred methods to examine the small bowel in most situations. These guidelines are intended to provide an evidence based document describing endoscopic investigation of small bowel disorders.
2.0 FORMULATION OF GUIDELINES
These guidelines were commissioned by the Clinical Services and Standards Committee of the British Society of Gastroenterology (BSG) and have been produced by the small bowel and endoscopy sections of the BSG. The guidelines have been produced to conform to the North of England evidence based guidelines development project.4 5 They have been drawn up from a Medline, Embase and Ovid literature search using terms “enteroscopy”, “push enteroscopy”, “intraoperative enteroscopy”, “double balloon enteroscopy” and “capsule endoscopy”. There have been 180 peer review studies, seven review articles, 58 case reports and letters, and one set of American guidelines on enteroscopy.6 The literature search for capsule endoscopy includes 100 peer review studies, 51 review articles, 74 case studies and letters, 21 editorials, four pooled analyses and two sets of guidelines: American and European on capsule endoscopy.7–9
2.1 Grading of recommendations
Grade A—requires at least one randomised controlled trial as part of a body of literature of overall good quality and consistency addressing the specific recommendation (evidence categories Ia and Ib).
Grade B—requires the availability of clinical studies without randomisation on the topic of consideration (evidence categories IIa, IIb and III).
Grade C—requires evidence from expert committee reports or opinions or clinical experience of respected authorities, in the absence of directly applicable clinical studies of good quality (evidence category IV).
2.2 Scheduled review
The content and evidence base for these guidelines should be reviewed within 5 years of publication. We recommend that these guidelines are audited.
3.0 SUMMARY AND RECOMMENDATIONS
If there is a high suspicion of bleeding from an upper GI source, a second look endoscopy should be undertaken prior to CE to ensure no pathology has been missed. (grade B)
Patients presenting with obscure gastrointestinal bleeding with a negative gastroscopy and colonoscopy should undergo capsule endoscopy if no contraindications exist. (grade B)
All patients undergoing CE for any indication should be appropriately counselled on the risks of capsule retention. (grade C)
Non-passage of a capsule may occur in the presence of a normal radiological contrast study. (grade B)
Those patients with pathology/bleeding sites identified on CE should subsequently undergo either a PE or DBE (oral/anal route) depending on location/site of bleeding. (grade B)
Push enteroscopy should ideally be performed using a dedicated push enteroscope. (grade B)
Endoscopic therapy should be attempted to minimise further bleeding episodes. (grade B)
In patients with a negative CE and persistent OGB, a second look capsule endoscopy may be considered. If this is negative they should be referred for DBE. (grade C)
Intraoperative endoscopy should be reserved for patients with persistent significant GI bleeding in whom the bleeding source remains undiagnosed. (grade B)
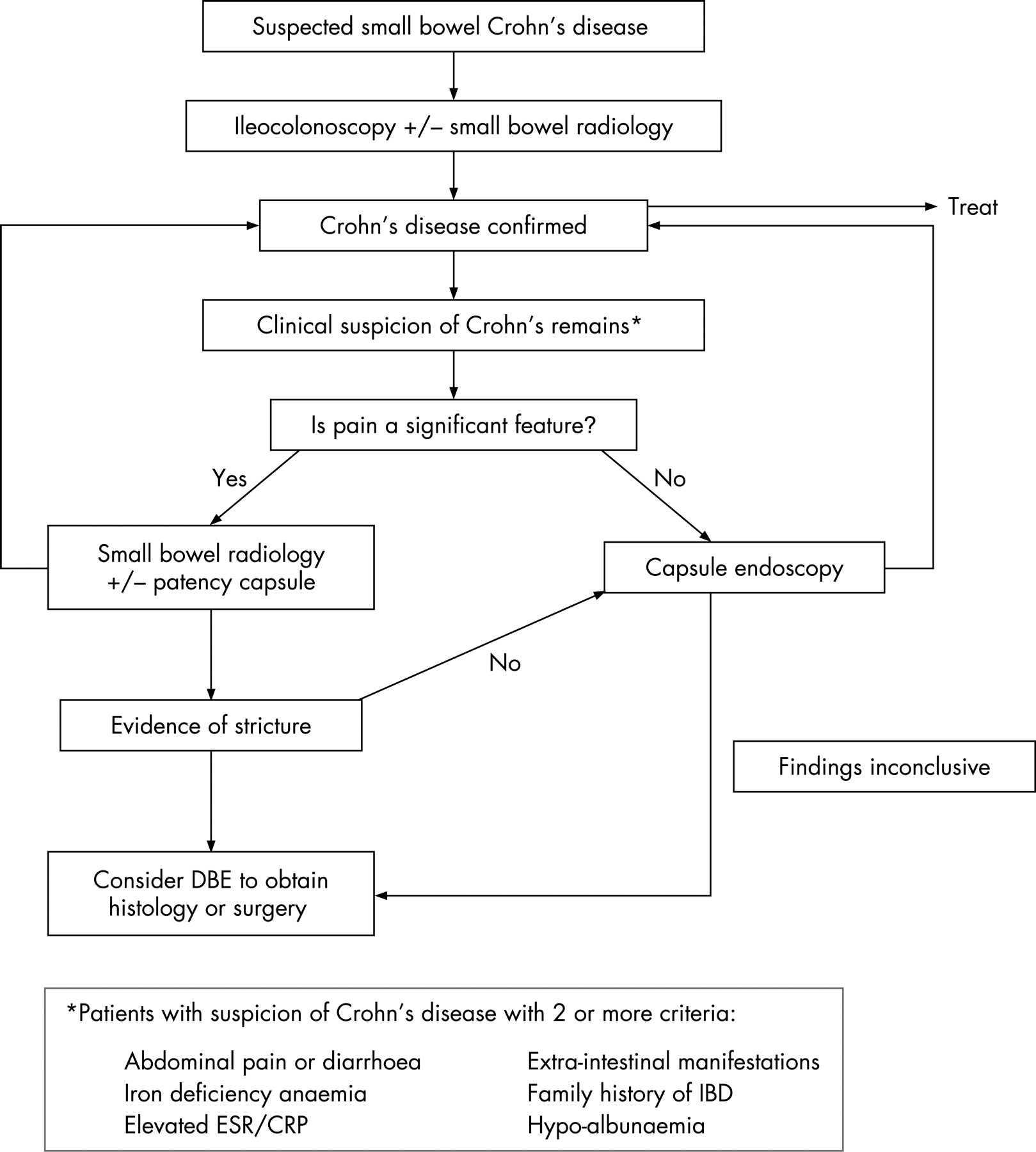
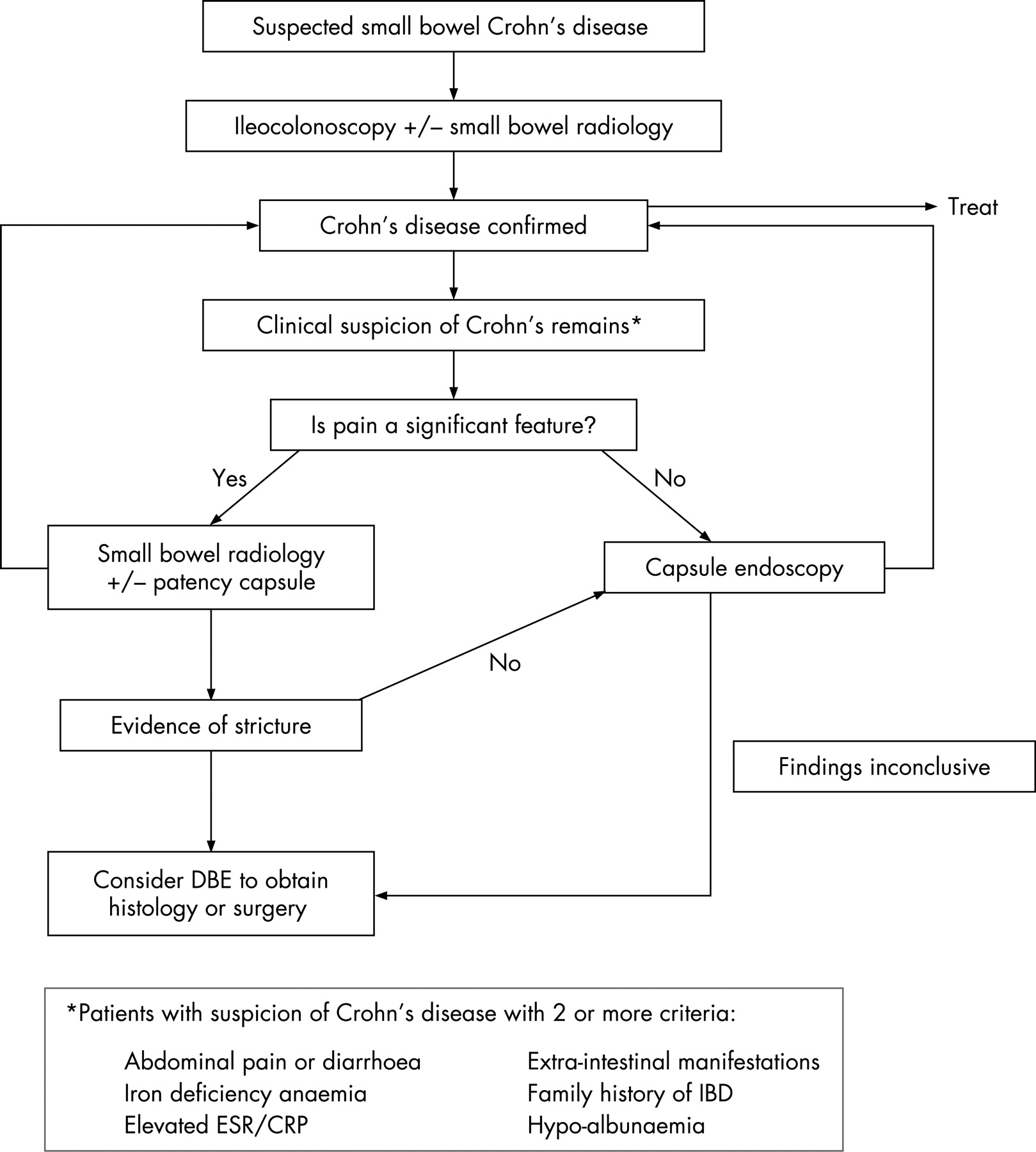
CE should be considered in patients with a high suspicion of small bowel Crohn’s disease based on the clinical history and inflammatory markers undetected by conventional means. Patients with abdominal pain as a significant feature should have radiological imaging to exclude a stricture prior to CE. (grade C)
CE should be considered in patients with refractory coeliac disease to look for coeliac associated complications. (grade C)
4.0 TYPES OF SMALL BOWEL ENTEROSCOPY
4.1 Enteroscopy using a colonoscope
The small bowel may be examined using a standard adult or a paediatric colonoscope without the purchase of a dedicated small bowel endoscope. The colonoscope is advanced as far as possible with the aid of abdominal pressure and change of position of the patient. Using this method, up to 60 cm of small bowel beyond the ligament of Treitz can be examined.6 In practice the stiffness of the adult colonoscope makes advancement difficult and the flexibility of the paediatric colonoscope causes frequent looping therefore this technique is of limited value.
4.2 Sonde enteroscopy
The sonde fibreoptic enteroscope, first described by Tada et al in 1977, has a working length of 250–400 cm, and is passed orally or nasally.10 It is advanced into the duodenum with the aid of another orally passed endoscope.6 It is then propelled through the small bowel by peristalsis. The main disadvantages are the lack of tip deflection, biopsy channel and length of time (from 4–6 h) taken for this examination which makes patient tolerance poor.6 The use of this method of examining the small bowel has largely been superseded by other modalities.
4.3 Push enteroscopy
Push enteroscopy is currently the most frequently used endoscopic method for small bowel examination.11 12 Dedicated push enteroscopes are 2–2.5 m in length with biopsy channels that can accommodate a range of accessories for therapeutic intervention.13 14
4.3.1 Technique
The endoscope is introduced orally and passed into the duodenum beyond the ampulla of Vater. After traversing the curve of the second part of the duodenum, the enteroscope is straightened to reduce any loops formed in the stomach. The enteroscope is then pushed to the maximum length of insertion.15 It is performed as an outpatient procedure, under conscious sedation and takes between 15 and 45 min.13
4.3.2 Use of an overtube
Initial studies using an overtube (first described in 198716) showed an increase in depth of insertion with its use.17–19 A number of reported complications, which include mucosal stripping,20 duodenal perforation,17 pharyngeal tear,14 pancreatitis and Mallory–Weis tear21 have been reported with the use of the overtube and this may limit its application during enteroscopy. Later studies with graded stiffness enteroscopes have questioned the additional value of the overtube, hence many units no longer use it in routine practice.22–24 The depth of insertion during push enteroscopy and the length of small bowel examined (30–160 cm) is variable.13–15 17 21 22 24–31 Two methods can be used to measure the maximum length of small bowel examined: metric measurement from pylorus on withdrawal after straightening, or fluoroscopy which helps to ascertain absence of a gastric loop.18 21 22 27 31
4.3.3 Indications for push enteroscopy
Push enteroscopy is indicated in the following clinical situations:
(a) Diagnostic
Obscure gastrointestinal bleeding
Malabsorption and unexplained diarrhoea
Exploration of radiographic abnormalities of the proximal small bowel
Investigation of small bowel tumours
(b) Therapeutic
Thermocoagulation of bleeding lesions
Placement of jejunostomy tubes
(c) Surveillance
Polyposis syndromes
(a) Diagnostic
Obscure gastrointestinal bleeding
In most patients who present with gastrointestinal haemorrhage, prompt investigation by way of clinical assessment and endoscopy of the upper or lower gastrointestinal tract provides a satisfactory diagnosis. The main indication for push enteroscopy is obscure gastrointestinal bleeding (OGB) when initial gastroscopy and colonoscopy have failed to detect the source of bleeding. This occurs in approximately 5% of patients who present with gastrointestinal haemorrhage.32 33 The investigation and management of OGB provides a resource intensive challenge for clinicians through repeated hospital admissions, investigations, transfusions and medical or surgical therapy.34 OGB is sub-classified as overt with the presence of melaena or haematochezia, or occult with anaemia and/or positive faecal occult blood testing.35 The diagnosis is often delayed due to slow or intermittent haemorrhage that is not detected during endoscopy or angiography. In the elderly, multiple potential bleeding sites may be seen without a clear indication of which lesion is the source of haemorrhage.36 The diagnostic yield of OGB with push enteroscopy is between 12 and 80%.12 13 15 23 26 27 37–49 with the highest yield in patients with overt bleeding.
Push enteroscopy has proven value in the investigation of patients with suspected GI haemorrhage when initial conventional endoscopy is normal. (recommendation grade B)
Twelve to sixty-four per cent of lesions located with push enteroscopy are within the reach of a standard endoscope.12–14 21 23 24 27 37–40 42 43 45 46 48 50 51 Lesions commonly missed are Cameron’s ulcers (linear ulceration in large hiatus hernia), varices, peptic ulcer disease43 and gastric antral vascular ectasia (GAVE) which can be diagnosed as gastritis by the inexperienced endoscopist.52 53
Repeat gastroscopy is recommended if an upper GI source is suspected despite the initial negative gastroscopy.17 39–42 (recommendation grade B)
Malabsorption and unexplained diarrhoea
Duodenal biopsy during upper GI endoscopy is the accepted approach to obtain histology in patients with suspected malabsorption. There is a modest role for push enteroscopy in patients with malabsorption when the duodenal biopsies are abnormal but non-diagnostic or if these individuals are endomysial antibody positive but have had a previously normal duodenal biopsy.29 54 55 In patients with refractory coeliac disease, in one small study, PE identified lymphoma in all four patients that were referred for investigation of refractory disease.48 In a similar cohort of eight patients, PE diagnosed ulcerative jejunitis in 50%.56 Push enteroscopy has also been shown to be useful in smaller studies in detecting rarer causes of diarrhoea such as lymphangiectasia and atypical infections (cyclospora, microsporidia)57 and sprue related strongyloidosis,17 when duodenal biopsies have been normal.
Push enteroscopy to obtain jejunal biopsies should be considered in patients suspected of malabsorption with positive anti-endomysial antibody and non-diagnostic duodenal biopsies. (recommendation grade C)
Radiological abnormalities
The use of push enteroscopy in the evaluation of abnormal radiographic studies has been shown to be helpful in confirming small bowel pathology in 33–83% of cases.13 17 23 25 28 58 However the endoscopist has to be confident that the area in question has been reached, to ensure the validity of a negative endoscopic examination. The enteroscope should be advanced beyond the area as far as possible and fluoroscopic verification can be helpful.28
Push enteroscopy is useful in investigation of proximal small bowel abnormalities detected by radiology. (recommendation grade C)
Small bowel tumours
Small bowel tumours account for 5–7% of patients presenting with OGB.59 60 It is the most common cause in patients under 50 years of age presenting with obscure GI bleeding.12 14 37 40 60 These patients may be asymptomatic at early stages or present with abdominal pain, episodes of obstruction or weight loss. The most common location for both epithelial and non-epithelial small bowel tumours is the jejunum while carcinoids are more common in the ileum.61 Diagnostic methods for small bowel tumours include enteroclysis, computed tomographic scanning, magnetic resonance imaging, arteriography and enteroscopy. In unselected case series the yield of small bowel tumours diagnosed during enteroscopy is between 3.5 and 11%.12 14 47 50 60 However, in some of these cases, there was already a suspicious lesion identified by small bowel imaging. Push enteroscopy offers the important opportunity of taking biopsies when the neoplastic lesion has been identified. (recommendation grade C) However, this approach can only be taken for lesions within the reach of an enteroscope. The adjuvant use of capsule endoscopy may enhance the selection of patients in whom proximal small bowel lesions could be reached and histology obtained.
(b) Therapeutic
Thermocoagulation of bleeding lesions
Angioectasia are the single most common cause of bleeding in patients above the age of 50 years14 21 34 40–43 62 and may account for up to 80% of the diagnoses.63 Angioectasia should be treated with thermocoagulation to reduce the incidences of recurrent haemorrhage.15 42 47 50 64 (recommendation grade B). Follow-up studies of patients with OGB and treatment initiated at enteroscopy, demonstrated a reduction in rebleeding episodes and transfusion requirement.30 38 43 63
Feeding jejunostomy
Percutaneous endoscopic jejunostomy (PEJ) placement is a modification of the PEG method (percutaneous endoscopic gastrostomy) described by Ponsky and Gauderer65 to provide alimentation directly into the small bowel. Indications include prior gastric resection or failure to locate the stomach due to abnormal anatomy and recurrent aspiration.66 It can either be placed directly into the small bowel66 or as a jejunal extension from a PEG.67 68 The endoscopist is responsible for assessing the need for topical anaesthesia and sedation.69 The current BSG guidelines advise prophylactic antibiotics for insertion of PEGs.70 Intravenous antibiotics such as cefotaxime or co-amoxiclav have been shown to be effective in reducing peristomal infection.70–73 Further studies are needed to assess their role in PEJ placements.
With direct PEJ insertion, push enteroscopy is used to get into the jejunum. The tip of the enteroscope is manoeuvred to obtain clear transillumination through the abdominal wall before the stylet is introduced into the jejunal lumen. Small bowel peristalsis may cause loss of the transilluminated site.66 For this reason, care needs to be taken to prevent the jejunum sliding and inadvertent puncture of other abdominal organs occurring. Complications that have been reported with PEJ include bleeding, aspiration and colonic perforation.66 Available data suggests that aspiration still occurs despite more distal placement of feeding tubes. This is thought to be due to aspiration of the patient’s own oropharyngeal secretions due to underlying neurological deficit or reflux of the feed.66 68 74 With jejunal extensions, commonly faced problems include occlusion and kinking of the tube, as well as malposition or migration into the stomach.68 Separation of the inner jejunal tube from the outer PEG tube and aspiration may also occur.67 68 74
Push enteroscopy is the method of choice for endoscopically placed feeding jejunostomy. (recommendation grade C)
(c) Surveillance
Polyposis syndromes
Patients with Peutz–Jeghers syndrome (PJS), a hereditary disorder characterised by mucocutaneous pigmentation and hamartomatous polyposis of the GI tract, are at risk of developing complications as a result of small bowel obstruction, intussusception and bleeding. The aim of management in these patients is to identify and remove the larger polyps endoscopically or surgically before they cause complications.61 Push enteroscopy allows exploration and polypectomy in the jejunum whilst intraoperative enteroscopy provides a supplementary means of removing polyps in the ileum.75 76
Patients with familial adenomatous polyposis (FAP) are at risk of developing extra-colonic polyps, particularly in the duodenum and periampullary region. Surveillance using a side-viewing endoscope is recommended after the age of 20 years by experienced endoscopists, unless the patient has symptoms that warrant investigations earlier.77 The Spigelman classification is used for staging of duodenal polyposis and is based on architectural parameters, grade of dysplasia, number and size of polyps.78 Push enteroscopy is used for endoscopic screening in FAP patients to identify high risk individuals.
The best screening method for small bowel polyps in both conditions is yet to be established. (recommendation grade C)
4.4 Intraoperative enteroscopy
Intraoperative enteroscopy (IOE) allows complete examination of the small bowel, and is the current “gold standard” for diagnosing obscure GI bleeding. It is performed when the source of bleeding remains undiagnosed by conventional investigations and the bleeding is massive, continuous or recurrent.79 The reported techniques of IOE vary in several important aspects: approach to intra-abdominal access (laparotomy versus laparoscopy), enteroscope used and technique of insertion (perorally or via multiple enterotomies).79–88 The introductory route is chosen according to the location of the presumed pathology. The procedure is done jointly by the endoscopist and a surgeon. The surgeon telescopes segments of the small bowel over the enteroscope to aid passage. The mucosa is inspected on insertion to avoid mucosal trauma being misdiagnosed as vascular lesions. The surgeon is also able to identify mucosal lesions externally by transillumination from the enteroscope.89 The air-trapping technique, which isolates segments of small bowel by gentle occlusion of the distal aspect, avoids excessive air insufflation and allows meticulous mucosal examination of each segment.83 90 Sequential segmental isolation and inspection is done in an antegrade fashion. Bleeding sites can be oversewn or segmental resections can be performed.87–89 The diagnostic rate of intraoperative enteroscopy for mucosal disease has been reported to range from 70 to 100%.80–82 90–93 Reported complications include prolonged post-operative ileus, mucosal or serosal tears, wound infection and multi-organ failure.81 82 88 89 91 IOE is able to identify treatable lesions with resolution of bleeding.82 83 88 90 It should, however, be reserved for a select group, particularly with the availability of double balloon enteroscopy which may allow complete small bowel visualisation and endoscopic treatment.
Intraoperative endoscopy should be reserved for patients with massive, continuous or recurrent gastrointestinal haemorrhage when other less invasive methods have failed to detect the source of bleeding. (recommendation grade B)
4.5 Double balloon (push and pull) enteroscopy
The DBE system (Fujinon, Inc., Japan) consists of a high resolution video endoscope with an outer diameter of 8.5 mm and a working length of 200 cm, and a flexible overtube with a length of 145 cm and an outer diameter of 12 mm.94 95 Air from a pressure controlled pump system is used to inflate and deflate the latex balloons that are attached to the distal end of the enteroscope.
The inflated balloon on the overtube is used to maintain a stable position while the enteroscope is advanced. The overtube balloon is deflated whilst the enteroscope balloon is inflated, and the overtube is advanced along the distal end of the enteroscope. This is described as the “push procedure”. This is followed by the “pull procedure” where both the enteroscope and the overtube are pulled back under endoscopic guidance, with both balloons inflated. This procedure is repeated multiple times to visualise the entire small bowel.96 97 The double balloon method reduces looping of the endoscope to a minimum. The average time for each approach (per-oral or per-anal) is 75 min.98 DBE can be performed under both conscious sedation and general anaesthetic, the former being the preferred choice in most studies.98–106 Few complications have been reported with DBE: post-procedure abdominal pain which may occur in up to 20% of patients,103 pancreatitis,103 107–109 bleeding and small bowel perforation which is more common after polypectomy of large polyps (>3 cm in size).110 111
4.5.1 Comparison of DBE with other small bowel imaging modalities
Abnormal lesions seen by capsule endoscopy (CE) that are beyond the reach of the push enteroscope have previously been managed either conservatively or by undertaking IOE or surgery.112 DBE allows visualisation of the majority of the small bowel (by combination of the oral and anal approach or oral approach alone).105 DBE also has features of a conventional endoscope such as rinsing, suction, biopsy and, importantly, allows therapeutic intervention.97 113 The insertion route is chosen according to the location of the suspected lesion.106 Total enteroscopy may not be necessary in the majority of patients where the small bowel pathology or bleeding source is found and treated.100–102 A successful endpoint would be resolution of bleeding.102 113 In addition, total enteroscopy may not be achieved in all cases.102 114 However, in cases where total enteroscopy is required, it is recommended that DBE via both anal and oral approach are not performed on the same day.115 This limits the increased risk of patient discomfort due to the longer procedure time and air insufflation. Insufflation of carbon dioxide during colonoscopy, flexible sigmoidoscopy and endoscopic retrograde cholangio-pancreatography has been shown to reduce patient discomfort in a small number of studies.116–119 There are no published studies to date comparing the use of carbon dioxide versus air insufflation for routine DBE. Carbon dioxide insufflation has the potential to be a useful alternative in DBE due to the longer procedure time. For total enteroscopy, the most distal point should be marked or tattooed. Studies comparing DBE and PE have shown that antegrade DBE is superior to PE in length of insertion.104 120 A higher success rate for deep intubation of the small bowel and improved diagnostic yield has been described.96 105 106 120 The diagnostic yield from DBE is between 43 and 83%95 98 101 103 105 106 110 112 114 121–125 with a subsequent change in management for 57–84% of patients.101 102 105 114 125 Whilst DBE may be more labour intensive, another advantage is that it allows “to and fro” observation and controlled movement.126 127 CE allows localisation of lesions prior to DBE.127 128 CE not only allows an initial imaging study for small bowel pathology but findings on CE may affect the endoscopist’s choice of route of insertion for DBE.99 128 The ability to confirm pathology and allow therapeutic application, makes DBE complementary to CE.100 129–131 DBE may be preferable to IOE in angioectasia, as repeat procedures may be needed to ablate new lesions that develop over time.121 In cases where surgery may still be required, biopsy sampling and India ink marking with DBE provides useful information to the surgeons.95 There have also been other therapeutic applications of DBE in the reported literature: the insertion of stents132 and the removal of them in patients with previous Roux-en-Y surgery,133 DBE assisted chromoendoscopy in patients with FAP134 and endoscopic ultrasound (EUS) of the small bowel.135 The use of EUS with DBE may be helpful to evaluate the depth of small bowel lesions and assessing the suitability of lesions for endoscopic mucosal resection. DBE has also been used to remove retained capsules, preventing the need for surgery.136–138
DBE should be used complementary to CE particularly in the context of therapeutic intervention beyond the reach of PE. (recommendation grade B)
5.0 CAPSULE ENDOSCOPY
The capsule endoscope (CE) is a 26 by 11 mm capsule containing a battery-powered complementary metal oxide silicon imager (CMOS), a transmitter, antenna and four light emitting diodes.139 The imager is activated by removal of the capsule from its magnetic holder and takes two images per second through the transparent plastic dome of the capsule. The capsule is swallowed and is propelled through the intestine by peristalsis. Currently, CE is manufactured by three companies: Pillcam SB, Given Imaging Ltd, Yoqneam, Israel; Olympus Endocapsule from Olympus, Japan; and OMOM capsule endoscope from Jinshan Science and Technlogy Group, Chongqing, China (not currently available in the UK). Whilst the Pillcam uses CMOS imaging, the other two prototypes of CE use charge-coupled device (CCD) technology.9
5.1 Technique
Patients are fasted for between 8 and 12 h prior to the procedure. As the capsule usually leaves the stomach within 30 min, the patient is allowed to drink after 2 h and eat after 4 h. Images taken by the capsule are transmitted via eight sensors, which are secured to the abdominal wall, to a battery-powered data recorder worn on a belt. The equipment is removed after 8 h (the approximate battery life) by which time the capsule has reached the caecum in 85% of cases.140 On completion of the procedure, the data from the recorder is downloaded onto a computer workstation which allows approximately 50 000 images to be viewed as a video. The average reading time of the video images takes between 40 and 60 min depending on the experience of the endoscopist.
The yield of CE can be affected by two problems: firstly, the presence of dark intestinal contents in the distal small bowel which may impair visualisation of the mucosa, and secondly the rate of gastric emptying and small bowel transit which could lead to the exhaustion of the capsule batteries before the capsule reaches the ileo-caecal valve. Incomplete examination occurs in 10–25% of cases.141–143 There have been a small number of studies and numerous abstracts addressing the use of bowel preparation (polyethylene glycol solution/oral sodium phosphate) to improve small bowel visualisation and the use of prokinetics (metoclopramide/domperidone/tegaserod/erythromycin) to accelerate transit times thereby improving the proportion of cases where the colon is reached.144–150 The current literature broadly suggests that by taking this approach, better quality of small bowel cleanliness is achieved; however, the optimal type of preparation, dosage and time of administration remains to be determined. In one prospective randomised study, the diagnostic yield was also found to be higher after bowel preparation.146 It has been also reported that caecal visualisation rates are lower in patients having capsule endoscopy during hospitalisation.143 Two small studies also suggested reduced intra-luminal bubbles and improved mucosal visibility after the administration of simethicone prior to CE.151 152 The available data at present are insufficient to make a firm recommendation for preparation of the patient for CE. (recommendation grade C)
5.2 Indications for capsule endoscopy
Obscure gastrointestinal bleeding
Small bowel Crohn’s disease
Assessment of coeliac disease
Screening and surveillance for polyps in familial polyposis syndromes
5.2.1 Obscure overt and occult gastrointestinal bleeding
Capsule endoscopy (CE) now has an established role in patients with persistent obscure gastrointestinal bleeding (OGB) who have had a negative gastroscopy and colonoscopy. Most studies using CE in patients with OGB have been in comparison to other modalities of investigation of the small bowel. Prospective studies have consistently revealed a superior diagnostic yield for capsule endoscopy compared to push enteroscopy in patients with OGB.1 153–166 A recent meta-analysis (of 14 studies on patients with OGB) reported yields of 63% for CE and 28% for PE.167 The yield of CE has also been shown to be superior to barium follow through and CT enteroclysis in the context of OGB.99 165 167 168 The second meta-analysis of 17 studies (526 patients) supports these findings: the rate difference (ie, the absolute pooled difference in the rate of positive findings) between capsule endoscopy and other investigative modalities for OGB was 37% (95% CI, 29.6 to 44.1).165
The rate of rebleeding in patients with OGB and negative CE is significantly lower compared to those with a positive CE (48% versus 4.6% respectively).169 In patients with a negative CE and cessation of bleeding, a conservative approach may be adopted.169 In the subgroup of patients with negative results on initial capsule endoscopy and persistent bleeding, a second look capsule endoscopy may be considered, as small studies have shown an additional yield of 35–75%.170 171 (recommendation grade C)
When comparing more invasive forms of endoscopy (DBE) with capsule endoscopy, diagnostic rates are similar. Studies comparing DBE and capsule endoscopy have shown diagnostic yields of between 42.9–60% (for DBE) and 59.4–80% (for CE).99 100 Complete small bowel examination was achieved more frequently by capsule endoscopy99 (90.6% compared to 62.5%, respectively; p<0.05).
Historically, intra-operative endoscopy has been considered the gold standard in patients with OGB and negative standard endoscopic evaluation. When compared to intraoperative endoscopy, capsule endoscopy had sensitivity, specificity, positive and negative predictive values of 95%, 75%, 95% and 86%, respectively.172 An algorithm for investigation of patients with OGB is suggested in fig. 1.173 (recommendation grade B)

5.2.2 Crohn’s disease
The small bowel is commonly affected by Crohn’s disease. Endoscopically, however, the small bowel is relatively inaccessible. In addition, ileal intubation is not always achieved at colonoscopy. Small bowel contrast studies have variable success rates in diagnosing active Crohn’s disease.1 174–176 Whilst CT may be effective in diagnosing small bowel thickening and complications of Crohn’s disease, its accuracy in determining the presence of mucosal disease is unknown. This difficulty partly explains a mean delay of between 1 and 7 years from onset of symptoms to diagnosis.177 178
A number of studies have now addressed the question of how best to investigate patients in whom conventional tests have failed to confirm a diagnosis of active Crohn’s disease. These include patients with symptoms of pain, diarrhoea, weight loss, or investigational findings including iron deficient anaemia and an acute phase response.179 Which combination of these features accurately predicts a diagnosis of Crohn’s disease is not known, but a consensus group has suggested that further investigation using CE might be considered in patients with two or more of these criteria.179 (recommendation grade C)
A number of studies performed have compared capsule endoscopy with colonoscopy and ileoscopy, small bowel follow through, CT enteroclysis and MRI.180–184 In addition to confirming suspected Crohn’s disease and assessing disease extent, CE has also been used in the context of recurrence of disease post-operatively.185
Capsule endoscopy versus endoscopy
Evidence of Crohn’s disease was found by capsule endoscopy in 43–71% of patients typically suspected of having Crohn’s disease in which colonoscopy (and small bowel radiography) had previously been normal.181 182 186 An analysis of four prospective comparative studies (total of 115 patients) showed a diagnostic yield of 61% for CE compared to 46% for ileo-colonoscopy in the detection of small bowel Crohn’s (p = 0.02; 95% CI, 2 to 27).179 CE was also able to identify the extent of disease proximal to the terminal ileum. CE has been found to have a greater diagnostic yield when compared to PE in patients known to have established Crohn’s disease perhaps reflecting the greater extent of small bowel mucosa visualised during CE.184 187
The use of CE for recognition of disease recurrence within 6 months of ileo-colonic resection, had a reported sensitivity of between 62 and 76% compared to 90% for ileo-colonoscopy.185 However, CE did identify lesions outside the reach of a ileo-colonoscope. This data does not necessarily represent that of routine clinical practice: capsules entered the colon in all cases (compared to a reported incomplete examination in 10–25% of other series) and all patients had successful ileo-colonoscopy (compared to an average UK rate of 57% for caecal intubation).188 Ileo-colonoscopy has a higher yield in the detection of recurrent disease compared to CE in patients post ileo-colonic resection. (recommendation grade C)
Capsule endoscopy versus small bowel radiology
In patients with suspected new or recurrent Crohn’s disease, CE was more likely to identify active disease than small bowel barium imaging.180 184 189 190 Studies comparing CT enteroclysis with CE also showed a higher yield of small bowel ulceration for CE.3 174 184 191 The two studies comparing CE and MR enteroclysis showed either comparable or better yield for CE.192 193 An important observation from most radiological versus CE studies is that radiological examination was able to delineate the presence of strictures which precluded the use of CE in a significant number of patients.184 191 192 194
A recent meta-analysis made a comparison of CE versus other modalities in established and suspected Crohn’s disease.190 In the evaluation of recurrence, CE is superior to both barium studies and ileo-colonoscopy in established non-stricturing Crohn’s disease. (recommendation grade B) However, despite a higher yield of CE in comparison to other modalities in the suspected Crohn’s group, the sub-analysis did not show a statistically significant difference in favour of CE in this group.190 Larger studies are needed to better establish the role of CE in the diagnosis of suspected Crohn’s disease. (recommendation grade C)
Capsule retention remains a risk in patients with Crohn’s disease even in the presence of radiological investigations that do not show significant strictures. This is discussed in more detail in section 5.3. In the studies referred to, with predominantly Crohn’s patients, retention occurred in 0–6.7% of cases174 175 182–184 186 191 192 194 and capsules passed either after medical treatment of Crohn’s disease,191 192 endoscopic removal191 or surgery.183 194 The risk is greater in patients with established Crohn’s disease compared to patients suspected to have Crohn’s disease.195
CE should be considered in patients with a high suspicion of small bowel Crohn’s disease undetected by conventional means. These patients should have radiological imaging to exclude strictures prior to CE. (recommendation grade C)
An algorithm for the investigation of patients suspected of having Crohn’s disease using CE is suggested in fig. 2. (recommendation grade C)
{kind=link}
{kind=link}
5.2.3 Coeliac disease
There have been two reported roles for the use of CE in coeliac disease. Firstly, typical mucosal changes of coeliac disease has been recognised at CE including a mosaic pattern, scalloping, “octopus leg” appearance, loss of mucosal folds and atrophy.196 197 As a result there have been small studies using CE as virtual histology in conjunction with positive coeliac serology, as the mucosal changes seen on CE is comparable to the macroscopic appearance at endoscopy. The sensitivity, specificity, positive and negative predictive values of CE for coeliac disease has been reported as 70%, 100%, 100% and 77%, respectively.196 At present, duodenal biopsy remains the gold standard and there is insufficient evidence for CE for the routine diagnosis of coeliac disease. (recommendation grade C)
The second group of patients who would benefit from CE are those with known coeliac disease established on a gluten free diet but with ongoing symptoms or those who develop alarm symptoms. These patients often undergo extensive radiological and sometimes surgical evaluation to look for possible complications of ulcerative jejunitis and small bowel lymphoma.198–200 A reported study showed a yield of 60% in detection of coeliac related complications including ulcerated mucosa, stricture and malignancy.198
CE may be indicated in the diagnosis of complications of coeliac disease. (recommendation grade C)
5.2.4 Familial polyposis syndromes
There is a small number of studies looking at the use of CE in surveillance of polyposis syndromes (familial adenomatous polyposis and Peutz–Jegher’s syndrome).201–207 CE is more accurate in detection of polyps than small bowel follow through and it can also detect smaller polyps in comparison to MRI.205 Given the limited number of studies, the routine use of CE in patients with polyposis syndromes is currently not advocated. The effect of CE on the change of management in this group of patients also needs further clarification. (recommendation grade C)
5.3 Complications of capsule endoscopy
The main risk of CE is capsule retention. CE is contraindicated in patients with known strictures or swallowing disorders. Patients with extensive small bowel Crohn’s (discussed in section 5.2.2) chronic usage of non-steroidal anti-inflammatory drugs and abdominal radiation injury are at higher risk. Patients should be fully informed about the risk of retention before consent for CE is undertaken. It should be highlighted that further intervention including surgery may be required if passage of the capsule is impeded by a stricture. Capsule retention has been defined by the International Conference on Capsule Endoscopy (ICCE) working group, as the capsule remaining in the digestive tract for 2 weeks or more requiring directed medical, endoscopic or surgical intervention.195 A large study (937 patients) reported an incidence of 0.75% of patients worldwide who required surgical intervention to remove a retained capsule.208 An alternative imaging modality should be considered prior to CE in patients with obstructive symptoms. (recommendation grade B) The absence of strictures on a barium study however does not entirely preclude the capsule being safely passed, as retention is known to occur despite a normal barium or enteroclysis study.141 183 194 In certain situations, however, CE may be used to diagnose an obstructing lesion not identified by other techniques and the capsule removed at surgery. (recommendation grade C)
A plain abdominal radiograph should be obtained to confirm excretion of capsule if the video fails to show that it enters the colon. Patients should not undergo magnetic resonance imaging after CE until they have safely passed the capsule. Occasionally the capsule may be retained in the stomach due to gastroparesis. In these cases, specifically designed “capsule delivery systems” are recommended for delivery of the capsule directly into the small bowel.209–212 (recommendation grade C)
There is theoretical potential for interference between the radiofrequency of the capsule, data recorder and permanent pacemakers (PPM) and implantable cardiac defibrillators (ICD). The manufacturers of CE have listed them as a relative contraindication for use of CE. Small studies have tested the use of CE in patients with these devices and have shown it to be safe without adverse events or interference of capsule images.8 213–215 Larger studies are required to verify its safe use. Advice should also be obtained either from the manufacturers of the cardiac device or the cardiologists to ensure that the capsule does not affect function of the cardiac device.215 216 (recommendation grade C)
5.4 Patency capsule
The M2A patency capsule was designed to overcome the potential hazard of capsule retention in high risk patients. This capsule is identical to the video capsule in size and shape. It is filled with lactose and protected by a plug with a specifically sized hole that allows the influx of intestinal fluid if impacted in stenosed bowel, which in turn dissolves the lactose in a predetermined time of approximately 40 h.217 The patency capsule also has a transmitter which allows it to be detected by a hand-held scanner placed close to the anterior abdominal wall. Small studies have recommended its safe use in patients with known small bowel strictures217 218 whilst one study showed that it can precipitate symptomatic intestinal occlusion.219 The occlusion may have occurred because the lactose plug requires fluid to dissolve and the distal side of an obstructed stricture may be relatively dry. More recently, the Agile patency capsule (Given Imaging, Yoqneam, Israel) which has dissolvable plugs at both ends has been devised to improve its use as a non-invasive tool in the assessment of functional patency of intestinal strictures.220 221 Larger studies are needed before the patency capsule can be recommended for routine use in the high risk group. (recommendation grade C)
6.0 SERVICE PROVISION AND TRAINING
The demand for CE has risen since its introduction in the United Kingdom. This is reflected by the increase in the number of centres which offer this service. In addition to developing a role in the investigation pathway of OGB and IBD, the use of CE is cost effective by preventing unnecessary cycles of investigations in patients.166 222 223
The reading of capsule endoscopy videos remains a time consuming exercise for gastroenterologists. Few studies have compared the inter-observer variability between an experienced gastroenterology or endoscopy nurse against a physician.224–227 Other investigators have also made comparisons between physicians of different levels of experience (endoscopy fellows or juniors endoscopists versus experienced physicians).228 These studies have shown that trainees were able to interpret CE images and reach the correct diagnosis in all clinically relevant cases. Specialist registrars and nurse specialists who have an interest in the small bowel may wish to take up this role. Incorporation of a section on capsule endoscopy into the generic curriculum would help to formalise the training in this field.
Despite the expansion of the service of capsule endoscopy, double balloon enteroscopy is likely to remain as a regional service. A DBE users group has recently been established to help promote standards, uniformity of practice and training across the UK. Like capsule endoscopy, formal training and perhaps, in addition, a basic skills course should be mandatory for all wishing to practise DBE. Regular audit of the service should be carried out at appropriate intervals. (recommendation grade C)
REFERENCES
Footnotes
Competing interests: Declared (the declaration can be viewed on the Gut website at http://www.gutjnl.com/content/vol57/issue1).