Article Text

Statistics from Altmetric.com
Shortness of breath is the chief complaint for about 8% of 999 calls to the ambulance service, and is the third most common type of emergency call. It can also be an important symptom in patients with a wide range of conditions. Reference should therefore be made to other relevant articles—particularly that discussing chest pain. The conditions covered in this paper include asthma, chronic obstructive pulmonary disease, acute pulmonary oedema, and chest infections. The objectives for this paper are listed in box 1.
Box 1 Article objectives
-
To consider the causes of breathlessness
-
To describe the recognition of primary survey positive patients and treatment of immediately life threatening problems
-
To describe the recognition and treatment of primary survey negative patients requiring immediate hospital admission
-
To describe the findings and treatment of primary survey negative patients suggesting delayed admission, treatment and referral, or treatment and discharge may be appropriate
-
To consider a list of differential diagnoses.
The common causes of shortness of breath are asthma, chronic obstructive pulmonary disease, and pulmonary oedema but there are many other conditions that can pose diagnostic problems (box 2).
Box 2 Causes of breathlessness
Very common
-
Asthma
-
Chronic obstructive pulmonary disease
-
Pulmonary oedema attributable to left ventricular failure
Common
-
Pneumonia
-
Pneumothorax
-
Pulmonary embolus
-
Pleural effusion
-
Pregnancy
Rare
-
Metabolic acidosis
-
Aspirin poisoning
-
Renal failure
PRIMARY SURVEY POSITIVE PATIENTS
Recognition
Patients with a life threatening respiratory emergency will present in either respiratory failure or respiratory distress. Patients with respiratory distress are still able to compensate for the effects of their illness, and urgent treatment may prevent their further deterioration. They present with signs and symptoms indicating increased work of breathing but findings suggesting systemic effects of hypoxia or hypercapnia will be limited or absent. Conversely, patients with respiratory failure may have limited evidence of increased work of breathing as they become too exhausted to compensate. The systemic effects of hypoxia and hypercapnia will be particularly evident in this group and immediate treatment will be required to prevent cardiac arrest. The key findings of primary survey positive patients with shortness of breath are presented in box 3.
Box 3 Recognition of the primary survey positive patient with shortness of breath
Increased work of breathing
-
Stridor associated with other key findings
-
Use of accessory muscles
-
Need to sit upright
-
Tracheal tug
-
Intercostal recession
-
Expiratory wheeze associated with other key findings
-
Cessation of expiratory wheeze without improvement in condition
-
Inability to speak in whole sentences
Systemic effects of inadequate respiration
-
Respiratory rate<10 or >29
-
Weak respiratory effort
-
Decreased, asymmetrical, or absent breath sounds
-
Oxygen saturation<92% on air or <95% on high concentration oxygen
-
PEFR<33% of normal
-
Hypercapnia (measured with end tidal CO2 monitor)
-
Tachycardia (⩾120) or bradycardia (late and ominous finding)
-
Arrhythmias
-
Pallor and/or cyanosis (particularly central cyanosis)
-
Cool clammy skin
-
Falling blood pressure (late and ominous finding)
-
Changed mental status—confusion, feeling of impending doom, combativeness
-
Falling level of consciousness
-
Exhaustion (+/−muscular chest pain)
Pitfall
Cessation of wheeze in a patient with severe asthma may be misinterpreted as an improvement in the patients condition
Tip
Cyanosis may be detected in patients with increased skin pigmentation by examining the inside of the mouth and eyelids
Treatment
If it is not possible to obtain an airway, if the patient’s condition is deteriorating rapidly, or they show signs of significant respiratory failure (in particular failure to maintain Spo2 of 95% on high concentration oxygen) consider immediate transportation to a hospital with appropriate facilities. Important treatment points for primary survey positive patients are listed in box 4.
Box 4 Treatment for primary survey positive patients
Treatment before transportation
-
Secure the airway (in moribund patients it may be necessary to escalate rapidly through manual methods, simple adjuncts, intubation, and cricothyroidotomy until airway secured)
-
High concentration oxygen via non-rebreathing mask (consider titrating concentration to a COPD patient’s “normal” Spo21)
-
Assist ventilations if respiratory rate<10 or >29, titrated to Spo2
-
Nebulised β2 agonist in the presence of wheeze (for example, salbutamol 5 mg initially)
-
Nebulised anticholinergic in the presence of asthma or COPD (for example, ipratropium bromide 0.5 mg, may be mixed with salbutamol)
-
IM adrenaline in the presence of anaphylaxis (see shock article)
-
Decompress tension pneumothorax
-
Consider MI/acute coronary syndrome: if present consider nitrates, aspirin, morphine and consider thrombolysis and heparinisation (see chest pain article)
Treatment during transportation
In addition to the above, consider:
-
Further nebulised β2 bronchodilators (no maximum dose for salbutamol)
-
IV fluids (asthma and anaphylaxis)
-
Intravenous or oral corticosteroids (asthma and anaphylaxis)
-
Antihistamines (anaphylaxis)
PRIMARY SURVEY NEGATIVE PATIENTS WITH NEED FOR HOSPITAL ATTENDANCE
Primary survey negative patients with the findings listed in box 5 who do not respond to prehospital treatment will require hospital admission.
Box 5 Diagnostic criteria for primary survey negative patients requiring hospital admission
Findings (not reversed by initial treatment) suggesting need for hospital admission
-
Inspiratory or expiratory noises (stridor or wheeze) audible without the aid of a stethoscope
-
Cannot speak in whole sentences
-
Respiration ⩾25 breath/min
-
Pulse ⩾110 beat/min
-
Supplemental oxygen required to maintain Spo2 at 95% or above (or at “usual” level of Spo2 for COPD patients)
-
PEFR<50% of normal
-
Inability to rule out MI or acute coronary syndrome
-
Lack of carer support for those patients unable to look after themselves
SECONDARY SURVEY
The SOAPC system should be used to undertake a secondary survey (see article 2 of this series). In primary survey positive patients, a secondary survey may not be completed in the prehospital phase of treatment as the focus must be on treatment of life threatening problems. For primary survey negative patients requiring hospital care the secondary survey may be undertaken during transportation. For the remaining patient population a secondary survey may be undertaken at the point of contact and will contribute to the decision to admit, treat and refer, or treat and leave.
Tip
If the patient is unable to tolerate a nebuliser, administer 10–25 puffs of β2 agonist (for example, salbutamol 1.0 to 2.5 mg) from the patients’ own inhaler via a large volume spacer, which can be improvised if necessary (fig 1)

Improvised large volume spacer using plastic soft drinks bottle.
Subjective assessment
Confirm that the chief complaint is shortness of breath. Remember that this may be a symptom of conditions affecting systems other than the chest (for example, hypovolaemia attributable to bleeding). Determine if this is a new problem or an exacerbation of a chronic condition. Ask what precipitated the problem and what, if anything, makes the patient feel more or less breathless. Ask about associated symptoms, such as chest pain, cough and sputum production, palpitations, fever and malaise, and leg pain or swelling. Has the patient been using inhalers or nebulisers more than normal? Have they recently sought other medical assistance?
Inquire about previous similar episodes. If this has occurred before, find out what treatment led to its resolution. Has the patient been hospitalised previously for this condition? What is their general previous medical history? What medications are they currently taking, and why? Is there a family history of respiratory illness or heart disease?
Finally, investigate the patient’s social circumstances. Is there evidence of self neglect? If the patient is not capable of caring for themselves, is there adequate carer support from family, friends, or health and social services? Does the patient smoke? Is there evidence of drug or alcohol misuse that may make the patient susceptible to infection?
Objective examination
Vital signs
The vital signs that should be recorded in a patient with shortness of breath are listed in box 6.
Box 6 Vital signs for assessing shortness of breath
-
Respiratory rate and effort
-
Spo2
-
Peak expiratory flow rate (PEFR) (fig 2)
-
Pulse rate
-
Blood pressure
-
Orientation and Glasgow coma score
-
Temperature

Peak flow meter in use.
Social context
In addition to the clinical assessment, it is important to consider the patient’s ability to care for themselves or whether suitable support mechanisms are available. If these are absent, can they be arranged? Can the patient perform the normal activities of daily living—feeding and washing themselves and using the toilet—either with or without support? The time of day and day of the week may also influence the decision about whether to admit or refer the patient, as this may dictate how quickly a patient could be seen by their own GP or reviewed by the emergency care practitioner.
Pitfall
Rrepeated “practice” attempts to measure maximum PEFR can worsen bronchospasm. Limit measurement to best of three forced exhalations
General examination
Look for signs of the “unwell” patient (see article two in the series). A detailed examination of the respiratory system is mandatory for patients with shortness of breath. Remember, however, that myocardial infarction, acute coronary syndromes, and congestive cardiac failure can also result in respiratory distress, as may endocrine and neurological problems (for example Kussmaul’s and Cheyne-Stokes respiration in hyperglycaemia and raised intracranial pressure respectively). If a respiratory problem cannot be readily identified as the cause of the patient’s symptoms, undertake an examination of the other systems.
Tip
Elderly patients are likely to have multiple pathologies, so undertake a general systems examination
Tip
Alhough shortness of breath can result from problems in many systems a useful clue is to note if there is any increase in effort of breathing. This invariably means the problem has a respiratory basis.
For details of the respiratory examination, refer to boxes 3, 5, 6, and 7 of this article and article 2 of this series. Note if the patient has excessive production of sputum. What colour is this? Yellow, green, or brown sputum indicates a chest infection. White frothy sputum, which may also be tinged with pink, suggests pulmonary oedema.
Look at the patient to determine their colour, and for signs of raised jugular venous pressure. Is the patient breathing through pursed lips, or using accessory muscles, perhaps suggesting COPD? Are there signs of CO2 retention (tremor of the hands, facial flushing, falling conscious level)? Palpate the trachea to check that it is in the midline. Examine the chest and observe chest expansion. Is this the same on both sides? Is there evidence of hyperinflation? Are scars present from surgery? Is there evidence of chest wall deformity?
Feel the chest to confirm equality of movement, and check for chest wall crepitus and surgical emphysema. Is there evidence of chest wall tenderness or pain? Is any pain positional, or worsened on inspiration (as, for example, in pleurisy)? Feel for tactile vocal fremitus (see the journal web site http://www.emjonline.com/supplemental).
Listen to the chest. Percuss the anterior and posterior chest wall bilaterally at the top, middle, and bottom of the back. Is the percussion note normal, dull, or hyper-resonant? Auscultate the chest at the same locations and in the axillae while the patient breaths in and out of an open mouth. Listen for the sounds of bronchial breathing, wheeze, or crackles. Listen for vocal resonance (see journal web site http://www.emjonline/supplemental) and pleural rubs.
Tip
If it is uncertain if a percussion note is dull or normal, compare with the result of percussing over the liver (lower ribs on the right). The percussion note will sound dull as the liver is a solid organ.
Tip
Tactile vocal fremitus and vocal resonance are increased in consolidation and decreased in pleural effusion and pneumothorax.
If the adult patient complains of symptoms of a respiratory tract infection, undertake an ENT examination. Look in the mouth to examine for tonsullar and pharyngeal inflammation, and feel for enlargement of the lymph nodes in the neck.
Pitfall
Do not attempt to examine the upper airway of a child with respiratory distress associated with stridor or drooling. These findings may be indicative of epiglottitis and attempts to examine the mouth and throat may provoke complete airway obstruction.
In all patients with sudden onset of shortness of breath and in the absence of other findings strongly suggestive of a respiratory problem, undertake an examination of the cardiovascular system (see articles two and three of this series).
The pertinent features of the respiratory examination are summarised in box 7.
Box 7 Pertinent features of the respiratory examination
General
-
Discoloured sputum
-
Consider examination of cardiovascular, ENT, and other systems
Feel (palpate)
-
Chest wall tenderness
-
Tactile vocal fremitus
-
Percussion note
-
Crepitus
-
Surgical emphysema
Look (inspect)
-
Skin colour
-
Jugular venous pressure
-
Tracheal deviation
-
Breathing through pursed lips
-
Use of accessory muscles
-
Hand tremor
-
Symmetry of chest wall movement
-
Hyperinflation or fixed expansion
-
Scars from previous surgery
-
Chest wall deformity
Listen (auscultate)
-
Bronchial breathing, wheeze, or crackles
-
Vocal resonance
-
Pleural rub
ANALYSIS (DIFFERENTIAL DIAGNOSIS)
Diagnosis is often straightforward with a typical history and findings. For example, the patient presenting with wheeze and tachypnoea may state that they have asthma. The skill is in determining the severity of the condition. Few patients die as a result of the misdiagnosis of asthma but significant numbers die because professionals or patients under-estimate the severity of an episode. Differential diagnosis can also be very difficult, the classic situation being in distinguishing between an exacerbation of COPD and cardiogenic pulmonary oedema. This may be made simpler by the use of b-naturetic peptide (BNP) estimations. This has recently been made available as a near-patient test and may become increasingly common in the out of hospital setting.
Asthma
Table 1 summarises the pointers in history and examination in patients with asthma that help to gauge the severity of an episode. Patients with severe or life threatening asthma need calm reassurance (even if the healthcare provider is panicking internally), early treatment with β2 agonists, oxygen, and immediate transfer to hospital. Patients with mild or moderate episodes who respond well to treatment may be suitable for home management with further inhaled β2 agonists, oral corticosteroids, and early review (tables 1 and 2).2
Differential diagnosis of asthma
“Personal best” PEFR values with ranges for estimating severity of acute asthma episode
COPD
Exacerbations of COPD are common. These can be triggered by a number of factors but a viral infection is the most frequent. Diagnosis is often simple but it is the assessment of the severity of the condition that needs skill. The main differential diagnosis is of cardiogenic pulmonary oedema (LVF). A pneumothorax is an uncommon reason for a severe sudden exacerbation of COPD. Knowledge of the patient’s normal pulmonary function is important. Some patients with COPD have a “normal” Po2 that would indicate severe respiratory failure in a normal person. Signs of exhaustion, inability to expectorate, or CO2 retention are the main worrying features indicating a severe episode.
Oxygen treatment in these patients should be titrated against the SPo2 (controlled oxygen therapy—see the North-West Oxygen Group guidelines).1 If the episode is not severe and the patient has adequate home support, then hospital admission may be avoided (table 3).3
Differential diagnosis of chronic obstructive pulmonary disease (COPD)
Acute cardiogenic pulmonary oedema
The onset is often sudden and severe. The patient is older and usually has a history of ischaemic heart disease although this may be the first indication of heart problems. Acute MI is often a precipitating factor. Severe shortness of breath, white frothy sputum, tachypnoea, and tachycardia are common. Such patients need to be transported to hospital, sitting upright if possible. Immediate treatment consists of buccal nitrates (providing the blood pressure is not low), oxygen, and intravenous opioids (table 4).
Differential diagnosis of acute pulmonary oedema (left ventricular failure/LVF)
Pneumonia
Fever, malaise, and purulent sputum suggest a diagnosis of pneumonia. The criteria for home treatment varies from country to country (table 5).4
Differential diagnosis of shortness of breath with fever and malaise (pneumonia)
CONDITIONS FOR EXCLUSION IF HOSPITAL ATTENDANCE IS NOT CONSIDERED APPROPRIATE
Box 5 lists the key findings that indicate the need for immediate hospital admission in primary survey negative patients. Table 6 describes additional findings determined from the secondary survey that will suggest the need for hospital admission. In asthma or COPD, failure to respond to the initial dose of a β2 agonist (for example, nebulised salbutamol) is also an indication for considering hospitalisation, as is a history of a previous near fatal attack—regardless of the severity of the current episode. All patients with a first episode of pulmonary oedema or an acute exacerbation of a chronic problem should be admitted to hospital for further investigation and treatment.
Findings from secondary survey suggesting need for hospital admission
Pneumothorax
Spontaneous pneumothorax is most common in tall, thin, fit young men (see table 6). It is an uncommon complication of asthma and COPD. There are some rarer causes but these will be very uncommon in the community setting. If a pneumothorax is suspected, the patient will need to be referred to hospital for a radiograph and further evaluation.
Pulmonary embolism
Half of all patients suffering for pulmonary embolism will develop this condition while in hospital or long term care. The remainder will have an unknown aetiology or will have been exposed to a known risk factor (see table 6). If a pulmonary embolism is suspected the patient will require urgent transfer to hospital for possible heparinisation or thrombolysis.5
TREATMENT AND DISPOSAL (PLAN)
The initial out of hospital treatment of each of the four key conditions is given in table 7 and boxes 8 to 10. Interventions recommended in the JRCALC guidelines for paramedic use are asterisked.6
Treatment of asthma2
Pitfall
Tension pneumothorax is a rare complication of asthma. Monitor for its signs and perform needle thoracocentesis (decompression) if these are present
Tip
Check the inhaler technique of patients left at home.7
Pitfall
Tension pneumothorax is a rare complication of COPD. Monitor for its signs and perform needle thoracocentesis (decompression) if these are present
Pitfall
Rule out acute MI: if present consider opioids, nitrates, aspirin, heparin, and thrombolysis according to relevant guidelines
Box 8 Treatment of COPD3
-
Protect and maintain airway as necessary*
-
Position for comfort (usually sitting upright)*
-
Salbutamol 5 mg via nebuliser*
-
Ipratropium 0.5 mg via nebuliser (may be mixed with salbutamol)
-
Re-assess: if patient’s condition returns to their normal state, consider managing at home:
-
Confirm appropriate technique when using inhalers
-
Consider increasing dose of bronchodilator
-
Consider oral corticosteroids if:
-
– Previous recorded response to corticosteroid therapy
-
– Dyspnoea is increasing despite prior increase in bronchodilator dose
-
-
Consider antibiotics if two or more of the following are present:
-
– Increasing dyspnoea
-
– Increasing sputum volume
-
– Development of purulent sputum
-
-
Refer to GP for appointment for re-assessment within 24 hours,
-
If no response to initial nebuliser, transport to hospital. On route:
-
– Repeat salbutamol 5 mg nebuliser at 5 min intervals until symptoms are controlled*
-
– Administer oxygen at 24 to 28% via Venturi mask initially
-
– Monitor Spo2 and adjust oxygen concentration to maintain at “usual” level for patient or at 90 to 92% if unknown (see North West Oxygen Group guidelines)
-
– Consider supporting ventilation if Spo2 cannot be maintained, patient becomes exhausted or respiratory rate or effort declines inappropriate
-
Box 9 Treatment of acute pulmonary oedema
All patients with an acute exacerbation of pulmonary oedema require hospitalisation
-
Protect and maintain airway as necessary*
-
Position for comfort (usually sitting upright)*
-
Oxygen via non-rebreathing mask*
-
Use continuous positive airway pressure ventilation (CPAP) if available: otherwise consider assisting ventilations with BVM if respiratory failure evident
-
400 μg glyceryl trinitrate spray if systolic BP>90 mm Hg*
-
Consider recording 12 lead ECG
-
Start transportation to hospital*
-
Consider second dose of GTN if SBP>90 mm Hg*
-
Give furosemide 40 mg IV*
-
Give morphine 5–20 mg IV (monitor respirations and assist ventilation if respiratory depression becomes evident)
-
Consider repeating furosemide 40 mg IV at 10 minute intervals to a maximum dose of 120 mg*
-
Consider salbutamol 5 mg via nebuliser in the presence of wheeze*
-
Consider further GTN 400 μg if SBP>90 mm Hg
Box 10 Treatment of pneumonia4
-
If no evidence of respiratory failure or severe respiratory distress, and the patient has adequate carer support and can manage normal daily activities of living (see chest pain article):
-
– Position for comfort (usually sitting upright)
-
– Antibiotic therapy
-
– Refer to GP for appointment for follow up within 24 hours
-
-
In the absence of adequate carer support and if unable to manage daily tasks of living, or if tachycardia, tachypnoea or chest pain are present:
-
– Consider hospital admission
-
– Oxygen via non-rebreathing mask if required to maintain Spo2 above 95%
-
– Consider intravenous crystalloids in the presence of dehydration
-
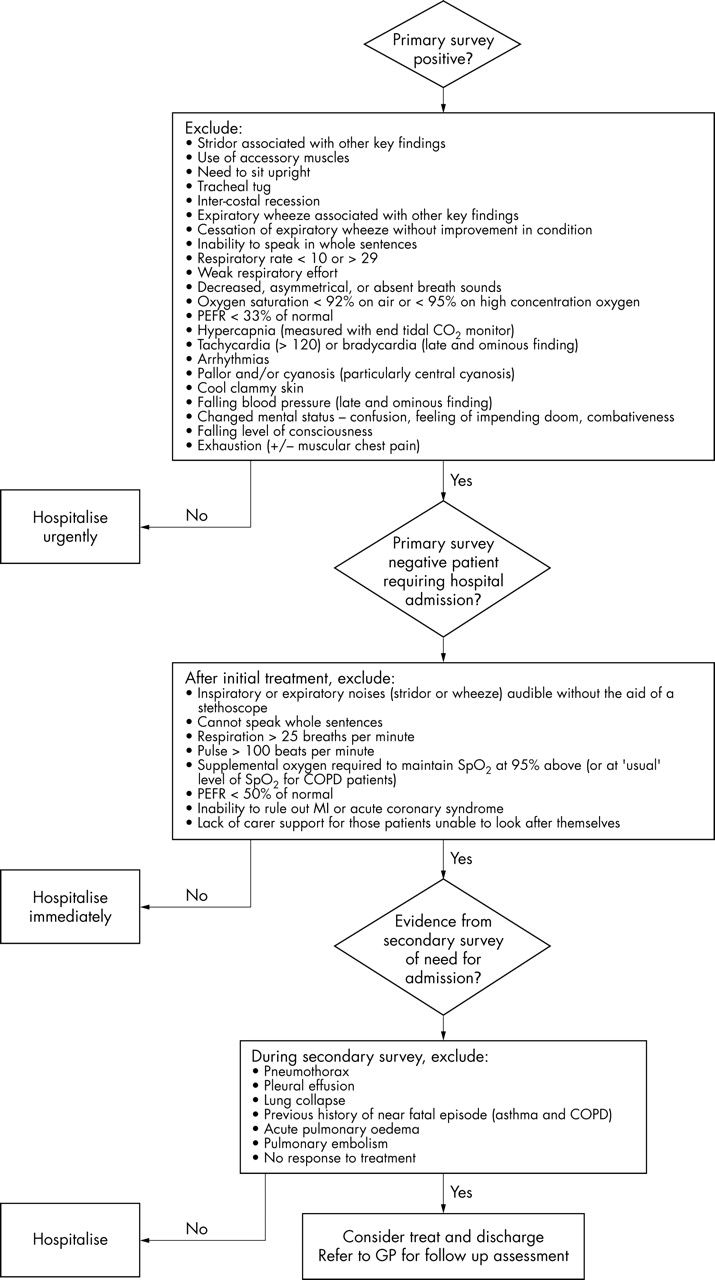
DISPOSITION FLOW CHART
Figure 3 describes the decision making process for patient disposition.

{kind=link}
{kind=link}
{kind=link}
Disposition flow chart (shortness of breath).
FOLLOW UP
Patients with an acute exacerbation of the conditions discussed in this paper but not requiring hospital admission should be advised to request further assistance if their condition deteriorates once the carer has left. Reassessment of the need for hospital admission is then mandatory.
All patients provided with home care should be referred for an appointment with their general practitioner within a suitable time frame for further assessment. This will include consideration of the patient’s ongoing condition, their ability to use inhalers correctly, measurement of their respiratory function (FEV1), and lifestyle management advice (for example, smoking cessation, weight control, exercise).
Acknowledgments
Thanks to Jim Wardrope, Peter Driscoll, and Colville Laird whose feedback resulted in valuable improvements to earlier drafts of this paper.
Contributions Malcolm Woollard wrote the first draft of the paper. Malcolm Woollard and Ian Greaves edited all subsequent drafts.
REFERENCES
Further reading
Supplementary materials
Web-only Appendix
The appendix is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [View PDF] - Appendix Information on tactile vocal fremitus