Article Text

Statistics from Altmetric.com
Reperfusion strategies in the early phase of treatment of acute myocardial infarction aim to rapidly normalise and maintain tissue perfusion. Primary angioplasty is probably the best current treatment but it can only be applied to a minority of patients and has its own problems. Thrombolysis remains the most commonly used treatment. It has well demonstrated benefits, saving lives and reducing left ventricular damage, but is far from perfect.1 The mega-trials have sent a clear message that the greatest benefits are seen with patients who are treated early. Clinical efforts have therefore been concentrated on educating the population to heed the early symptoms, encouraging rapid admission to hospital (sometimes with thrombolytic treatment being administered in the ambulance) and minimising “door to needle” times. Continuous and widespread use of audit increases the number of patients treated and the speed with which treatment is administered.
Key points
Failure of thrombolytic treatment at 1–2 hours is associated with a 30 day mortality > 15%
The diagnosis of failed thrombolytic treatment is currently best achieved with repeat 12 lead ECGs
The absence of chest pain 1–2 hours after the onset of thrombolytic treatment does not imply reperfusion
Conversely, the presence of chest pain does not imply failure to achieve TIMI-3 flow at coronary angiography
Angiographic coronary patency at 60–90 minutes is achieved more frequently after t-PA or r-PA compared with streptokinase, but there is no significant difference in vessel patency at 6–12 hours between these agents
Angiographic TIMI-3 flow is achieved in only 25–50% of patients with modern thrombolytic agents at 90 minutes after onset of treatment
Normal tissue perfusion is achieved in < 40% of patients treated with current thrombolytic agents
Repeat thrombolysis has not been shown to reduce mortality associated with failure of initial treatment
Rescue angioplasty has been shown to confer some clinical benefits in patients with first time anterior infarction as long as it is delivered within 6–8 hours of onset of chest pain
The optimal timing of rescue angioplasty after the onset of thrombolysis is unknown
Rescue angioplasty has not yet been shown to reduce the mortality associated with failure of thrombolysis
Ongoing clinical trials hope to establish the role of repeat thrombolytic treatment and rescue angioplasty
Having been treated with thrombolytic therapy and aspirin (and heparin if tissue plasminogen activator (t-PA) is used), patients fall into two groups—those who do benefit, and those who do not benefit. The former can be further categorised into those who respond rapidly and those who appear to reperfuse relatively late. The management of lytic failures and slow reperfusers is perhaps the most vexing current problem facing doctors working in coronary care units and interventional catheter laboratories.
The use of terminology should be precise in this context.2 Reperfusion implies perfusion at tissue level. This can only be assessed accurately by modern imaging techniques (not conventional coronary angiography) or by near complete normalisation of the 12 lead ECG. Vesselpatency implies that there is flow down the vessel, however ineffective. Recanalisationimplies that a previously occluded vessel has re-opened. Recanalisation and patency are best assessed by angiography. Tissue perfusion does not necessarily imply patency, as sometimes tissue is supplied by collateral vessels. Conversely, patency does not necessarily imply perfusion—for example, as with the “no-reflow” phenomenon.
Mechanisms of failed thrombolysis
Certain clinical features predisposing to failure of thrombolysis have been identified, but the precise mechanisms are not well established. Patients with failure of thrombolysis are generally older, non-smokers, more likely to have had a previous infarct, and have a greater delay to lytic treatment.3 ,4 A number of mechanisms of lytic resistance have been postulated, separable into two groups:
- (a)
- Resistance to thrombolysis. Proposed factors implicated in resistance to thrombolysis are shown in the box above. Genetic differences between patients may exist but have not been studied in depth. Varying levels of circulatory factors and thrombin release in response to thrombolysis are likely to be important.5 Mechanical factors are also implicated.
- (b)
- Resistance to tissue perfusion. It is well recognised that tissue flow can be impaired even with normal epicardial flow, and that no- or slow-flow appearances can be found in the absence of a significant epicardial coronary obstruction. A number of reasons are thought to be responsible. The most plausible relates to embolisation of platelet aggregates, cholesterol crystals, and other atheromatous debris after plaque rupture. Endothelial swelling and distal vessel vasoconstriction may also play a role.
Some possible mechanisms of failure of thrombolytic treatment
As yet unspecified genetic differences
Varying levels of circulating factors
fibrinogen
lipoproteins
thrombin/antithrombin III complexes, etc
Mechanical factors
arterial pressure proximal to occluding thrombus
myocardial wall tension
thrombus burden
lesion complexity when reperfusion starts
residual stenosis after initial reperfusion
subintimal haemorrhage
Incidence of failed thrombolysis
It is difficult to define the incidence of failed thrombolysis precisely as it is dependent on multiple factors, not least the timing and method of evaluation of efficacy and the definition of success and failure. Others include the thrombolytic agent used, the dosing regimen, the clinical characteristics of the patients being treated, and the time from symptom onset to start of treatment.
Studies using angiography and contrast echocardiography have been performed on selected groups of patients. For those patients eligible for thrombolytic trials, overall patency is achieved with current agents in 60–85% of patients, but only 50–60% achieve TIMI 3 flow and significantly fewer achieve this in the first 90 minutes (between 25–50%). Of the most commonly used drugs, alteplase and reteplase achieve earlier patency and TIMI 3 flow than streptokinase, but there is a catch up phenomenon with the latter over the next few hours. Overall, only 25–40% achieve normal perfusion; many patients shown to have normal angiographic flow can be shown to have incomplete tissue perfusion. In addition, over 10% will reocclude while still an in-patient (overtly or silently) and 30% by three months.1 ,2 ,5-7
On this basis, currently used thrombolytic agents fail to achieve patency in at least 15–40% of patients (the average is about 30%); they fail to achieve normal TIMI 3 flow in approximately 40–50% (50–75% at 90 minutes), and fail to achieve normal tissue perfusion in 60–75%. Figures for all comers (including those not eligible for trials) are likely to be significantly worse.
Significance of failed thrombolysis
However defined, failed thrombolysis is associated with a much higher chance of early death and greater left ventricular dysfunction.3
Following the GUSTO angiographic trial, other studies have evaluated the relation between angiographically defined TIMI flow and outcome. In a meta-analysis, TIMI 3 flow was associated with a 4–6 week mortality of 3.7%, compared to 7% for TIMI 2 and 8.8% for TIMI 0 and 1 combined.8 Although TIMI 2 is associated with a numeric value of mortality between that of TIMI 3 and TIMI 0/1 flow, it is far nearer the result of no patency than full flow. Thus, when angiography is performed, TIMI 3 flow is the desired end point. Angiographic studies, however, have been performed on a selected group of patients treated relatively early after symptom onset. One study investigating a consecutive series of unselected patients suggests that the early mortality of failed reperfusion defined electrocardiographically is associated with a mortality of 16–20%.9
Diagnosis of failed thrombolysis
Patients whose ECGs return to normal early do well with low mortality and preserved left ventricular function. Unfortunately this situation is not common. Relief of chest pain together with normalisation of ST segments and the identification of reperfusion arrhythmias only occur together in 15% of patients. Also, chest pain is diminished or abolished with opiates in many, including those with a persistently occluded vessel. Conversely, a persistent ache often occurs in those with an open vessel (possibly because of lack of tissue perfusion). As age, diabetes, pain threshold, and the development of pericarditis also influence pain, then the presence or absence of pain is limited as a diagnostic test. However, consideration of rescue techniques for those with continuing ischaemic pain may be one method of targeting those most likely to benefit. The situation is further clouded by the fact that reperfusion is sometimes characterised by an increase in pain and further temporary elevation of ST segments; patients with these features usually have large infarcts.
There is an obvious need to define failed thrombolysis clinically, as then efforts can be made to treat patients with an alternative strategy. As time is essential, a successful diagnostic technique must be simple, easy to use, and the results must be made available rapidly. It may not matter which test is applied within a single coronary care unit as long as the diagnostic limitations of the chosen test are understood. A sensitive test will detect all those with failed reperfusion but may have low specificity—that is, it may lead to further investigation or treatment of many patients who have reperfused. A specific test (that is, if positive, failed reperfusion is almost certainly the correct diagnosis) may have low sensitivity, so a compromise is needed.
Tissue perfusion
The ideal method of diagnosing failure of thrombolytic treatment would be some test of myocardial perfusion. Possibilities include positron emission tomography and contrast echocardiography. Although they have been used to demonstrate the inadequacies of thrombolysis as well as its angiographic analysis, they have not been used prospectively in studies of diagnostic power. In addition, they require equipment or training that is not commonly available.
Angiographic flow
Although angiography has been considered by many to be the gold standard for diagnosis, it has major limitations. The act of angiography itself can influence the efficacy of thrombolytic agents, opening up some occluded vessels.10 Although the TIMI flow rate is the established method of analysis, this does not actually measure tissue perfusion. However, until techniques for measuring the latter are perfected, this will probably remain the methodology used for analysing new reperfusion strategies.
Electrocardiographic techniques
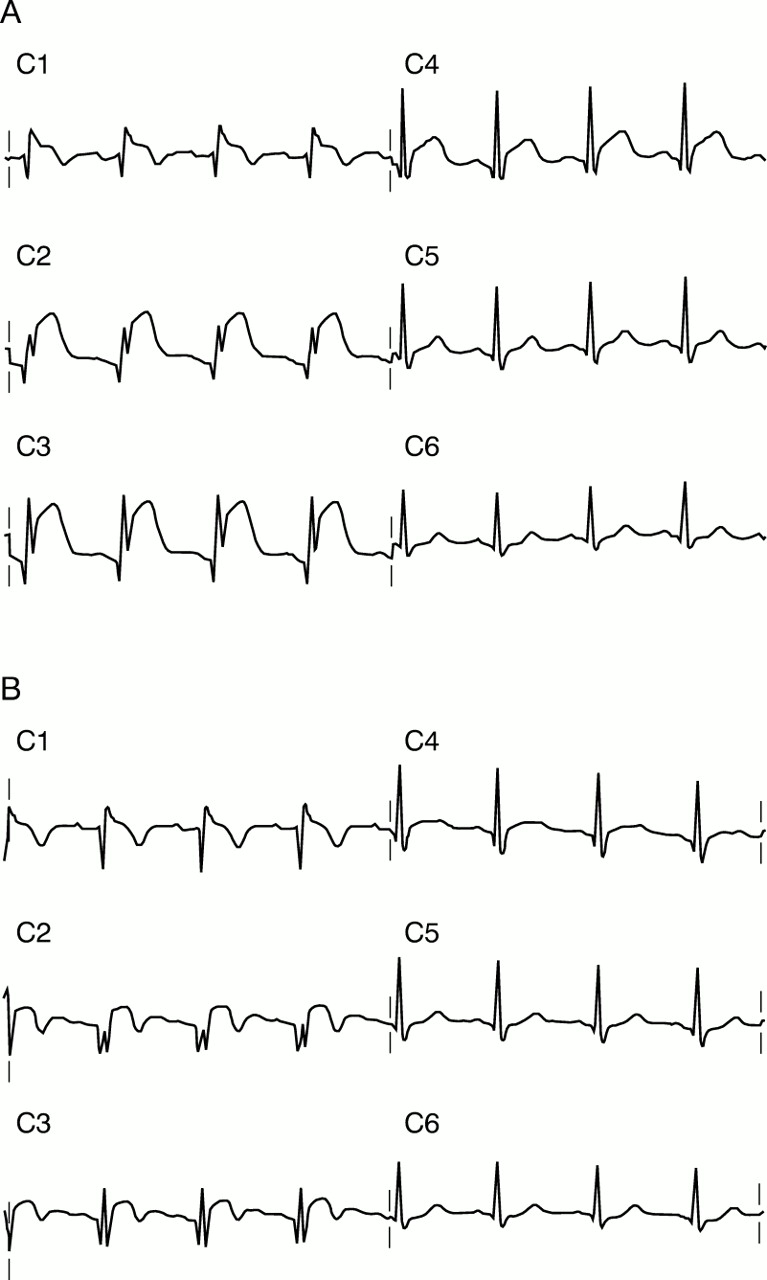
Many ECG criteria have been examined. These include the ratio of the height of maximum ST elevation before and after treatment (usually measured 80 ms after the J point), the ratio of sums of ST segment elevation and/or depression, and the height of the T wave. There are few prospective studies where the ECG has been analysed at predetermined times following thrombolytic treatment with respect to the results of angiography. The criterion that appears to be most established is failure of the elevated ST segment (measured 80 ms after the J point in the lead of the 12 lead ECG with maximal ST elevation at baseline) to fall by 50% or more (figs 1 and 2). If measured two hours after the start of thrombolysis the diagnostic accuracy is about 80–85% for failure to achieve TIMI 3 flow.10 This means that 15% of patients will, however, be wrongly classified. Some patients will have a fall in ST elevation but the vessel remains occluded (false negative for failed thrombolysis). It has been demonstrated, however, that those who have early ST falls are in a good prognostic group, and so it is possible that those who fail to achieve patency are protected in some way (possibly by collaterals). If the 12 lead ECG is used, an ECG recorded at 60 minutes after onset of thrombolysis identifies a high risk group with as much accuracy as one recorded at 90 and 180 minutes.9

ECG diagnosis of successful thrombolysis. The baseline ECG before thrombolytic treatment shows significant ST elevation in the anterior leads, with maximal ST elevation of 7 mm in lead V3 80 ms after the J point (A). Two hours after the start of thrombolysis with streptokinase, the ST segments have reduced (B). Although the ST elevation in C3 is 2–3 mm, the fall in ST elevation from baseline is greater than 50% of the initial elevation. The patient was shown at angiography to have TIMI 3 flow in the left anterior descending artery (the infarct related vessel).

ECG diagnosis of failed thrombolysis. The pre-thrombolysis ECG shows significant ST elevation, maximal at just over 4 mm in lead V3 (A). Two hours after the start of thrombolysis, there is no change in the ST elevation in this lead (B). The patient was shown to have an occluded left anterior descending artery at angiography just after the ECG was taken.
Continuous ST monitoring using a varying number of ECG leads has been studied by several groups. This technique has revealed the very dynamic nature of the reperfusion process. ST segment monitoring is attractive in concept as this provides a means of assessing peak ST elevation, rather than its baseline level just before treatment starts. This could improve accuracy, but additional equipment is necessary and results must be available on-line for meaningful clinical use. ST segment and QRS vector analysis are other methods under evaluation but are not in routine clinical use.
Reperfusion arrhythmias are well recognised but are very insensitive for prediction of reperfusion. The early and frequent appearance of automatic idioventricular rhythm is perhaps the most useful marker of reperfusion and the absence of this rhythm can be incorporated as one of several criteria to help make the diagnosis of failed reperfusion.10
Biochemical markers
Measurement of cardiac enzyme release has become an integral part of the retrospective diagnosis of myocardial infarction, and the peak concentrations are useful in the process of risk stratification. In general, though, they have not proved very useful for immediate decision making in the management of acute myocardial infarction. Although enzyme concentrations can now be measured rapidly, a single measurement is not useful and even sequential measurements are difficult to interpret as the shape of the release curve relates to the time from onset of infarction (which is very variable) and, of course, to the thrombolytic agent used.
Early peaking of creatine kinase or its isoforms is seen with reperfusion (the “washout” phenomenon), but the time course is such that its identification occurs too late to add a second treatment, and there is considerable overlap with non-reperfused patients. Moreover, its assessment needs multiple blood tests and rapid delivery of laboratory results. More productive research has aimed at investigating the concentrations of enzymes and the rate of change of plasma enzyme concentrations in the first two hours or so, making use of the fact that those patients who reperfuse have a much earlier and a higher peak than those who do not. Early studies investigated creatinine kinase isoforms but predictive accuracy was disappointing. More recently, attention has turned to the use of myoglobin or troponin (T or I) concentrations.4 These proteins can be identified earlier and the hope has been that their measurement would lead to greater accuracy in assessing the efficacy of thrombolysis. This has not yet proved to be the case and they are unlikely to be used on a widespread basis until studies comparing their predictive accuracy with ECG markers are performed.
Timing of diagnosis
Lytic trials have shown that the greatest impact of treatment is seen in those individuals treated within three hours of onset of symptoms, with a smaller impact for those presenting within 3–6 hours. Thereafter, although benefit can be identified out to 24 hours, the magnitude of benefit is considerably less—the number needed to treat increases exponentially with time. With relatively inexpensive therapy such as thrombolytic treatment, cost effectiveness issues are not so important, especially as relatively few patients nowadays present late. However, with more expensive strategies such as angioplasty, the cost effectiveness arguments become a real issue. With this in mind, and given our current lack of knowledge, it is probably inappropriate to offer rescue angioplasty to patients who are more than 12 hours into infarction, and some might argue that there may be little to gain for those considered after eight hours.
Although the concept of “time is muscle” might argue in favour of a rescue strategy being offered early after thrombolytic treatment, a number of issues should be considered.
First, reperfusion rates after thrombolysis increase with time, and providing a second treatment too early may result in it being offered to patients who were going to do well anyway. If offered too late, then many patients are denied any potential benefit, and there is less myocardium to salvage.
Secondly, success rates and risks of rescue treatment, and the way these may change with time after thrombolytic treatment, are poorly characterised. Repeat thrombolysis carries an obvious potential for increasing the risk of clinically important bleeding. Potential problems related to rescue angioplasty include those associated with angiographic contrast load, late reperfusion injury, and embolisation. Previous studies of angioplasty used as a routine after thrombolysis demonstrate a potential for doing harm—the need for targeting those who will benefit is clear. If the risks of rescue angioplasty are not time dependent, then offering it relatively late aims to benefit a truly high risk subset of patients (but success rates might be low for this subset). If the risks increase with time, then offering it late may worsen the outcome of this already high risk group. The balance between early risks and late benefits is crucial to the overall efficacy of treatment (fig 3).

Theoretical considerations in evaluation of interventional treatment in acute myocardial infarction. The treatment will only be justified if the late benefit greatly exceeds early hazard. Currently, the areas between the curves and the time to crossover in relation to rescue angioplasty are unknown.
A third factor that must be considered is the time delay between a decision to offer a second treatment and the ability to provide it. Repeat thrombolysis can be delivered immediately (although it will take time to be effective), but rescue angioplasty will often require the calling out of an out-of-hours cardiac catheterisation laboratory team and/or the transfer of the patient from one hospital to another. This time delay would argue for a decision being made earlier than might be the case for repeat thrombolysis.
Fourthly, most of the studies looking at the non-invasive diagnosis of failed thrombolysis have looked at the results of tests obtained 60–180 minutes after the onset of treatment. The diagnostic accuracy of tests performed later is not known.
Previous studies have not helped provide the answer for the optimal time for a second treatment (whether angioplasty or repeat thrombolysis), and current studies are not designed to look at this point. Although there is an intrinsic desire to open vessels as fast as possible, rushing in to do so may be inappropriate, particularly if angioplasty is then offered routinely to all patients, including those whose vessels have already recanalised with normal flow (see below). Either a delay might be appropriate or angioplasty should only be offered to those with occluded vessels, as both might swing the risk:benefit ratio in favour of the treatment.
Arguments for immediate rescue treatment can thus be countered to some extent by an argument for delay. Our current understanding suggests that the timing of intervention should be as follows: (a) should repeat thrombolysis be considered, then fibrinogen concentrations should be measured at 60 minutes and a 12 lead ECG recorded at 90 minutes and treatment targeted at those who appear not to have reached a lytic state (see below); (b) should rescue angioplasty be offered, two diagnostic strategies can be considered. In one, a non-invasive diagnostic test performed at 60–120 minutes allows the treatment to be delivered to selected patients at a reasonable time after thrombolysis. The other offers immediate angiography as soon as possible after thrombolysis, with rescue angioplasty being offered only to those with persistently occluded vessels.
Management options
In the majority of coronary care units, failure of thrombolysis is either not looked for or a second treatment is not considered. Even if the early response to thrombolysis is poor, many hope that, given more time, the thrombolytic agent will be effective. Although these patients are clearly at a disadvantage for the reasons outlined above, the lack of activity cannot be unduly criticised as current research does not clearly identify a “correct” strategy. The other options are considered below.
Repeat thrombolysis
Although further thrombolysis can be offered successfully to those who reinfarct after initial reperfusion, there has been only one study of a strategy of repeat thrombolysis for failure of initial treatment.11 The Newcastle protocol was to record a 12 lead ECG 90 minutes after streptokinase. Failure of the baseline ST elevation to fall by 25% or more in the lead showing the greatest elevation was used to define failed reperfusion. These patients were randomised to receive either standard dose alteplase or placebo. Improved left ventricular function was seen in the treatment group, but only in those with failed fibrinogenolysis, defined as a 60 minute fibrinogen level > 1 g/l. This small study (37 patients) was not powered to look at survival benefits, nor for an adequate analysis of bleeding risks (it should be remembered that the combined thrombolytic arm of GUSTO-I doubled the risk of haemorrhagic cerebral events). At this stage, this study cannot be used to support a widespread use of this strategy.
Rescue angioplasty
The literature on rescue angioplasty is dominated by observational series and the few randomised studies have been on relatively small groups of patients.12-15 Current knowledge of rescue angioplasty can be summarised as follows:
- (1)
- transferring patients from community hospitals to revascularisation centres in the setting of acute myocardial infarction is associated with an acceptably low risk;
- (2)
- unless delivered very early after thrombolysis, rescue angioplasty is less likely to achieve patency compared to primary angioplasty (80–90% v 90–95%) and less likely to achieve TIMI-3 flow; moreover, reocclusion rates with standard balloon angioplasty are higher in this setting (15–30%) than after primary angioplasty (5–15%);
- (3)
- rescue angioplasty is applied later than primary angioplasty (because of the time taken for thrombolytic treatment to be administered and the additional delay until the diagnosis of failed thrombolysis is made);
- (4)
- by definition, rescue angioplasty is associated with the downside of the thrombolytic agent initially administered (allergy, hypotension, and haemorrhage);
- (5)
- although patients with successful rescue angioplasty do relatively well (in-hospital mortality between 5–10%), failed rescue is associated with a high mortality (25–40%)—overall, the mortality of the entire cohort undergoing rescue angioplasty is higher than the mortality associated with primary angioplasty (probably because the treatments are offered to patients with different risk profiles, but an early hazard associated with rescue angioplasty cannot be excluded).
The latter possibility is suggested particularly from data obtained in the GUSTO-1 angiographic substudy, in which rescue angioplasty was a prespecified end point. Operators performing angiography at 90 or 180 minutes were permitted but not required to perform rescue angioplasty if the vessel was occluded. The overall mortality for the whole rescue group was actually 11.1% (8.6% for successful rescue, 30% for failed rescue), which was higher than the 7.9% for the lytic failure, no rescue group. Although this may simply have represented a higher risk group, it is suggestive that rescue angioplasty may be associated with early harm in some patients.16
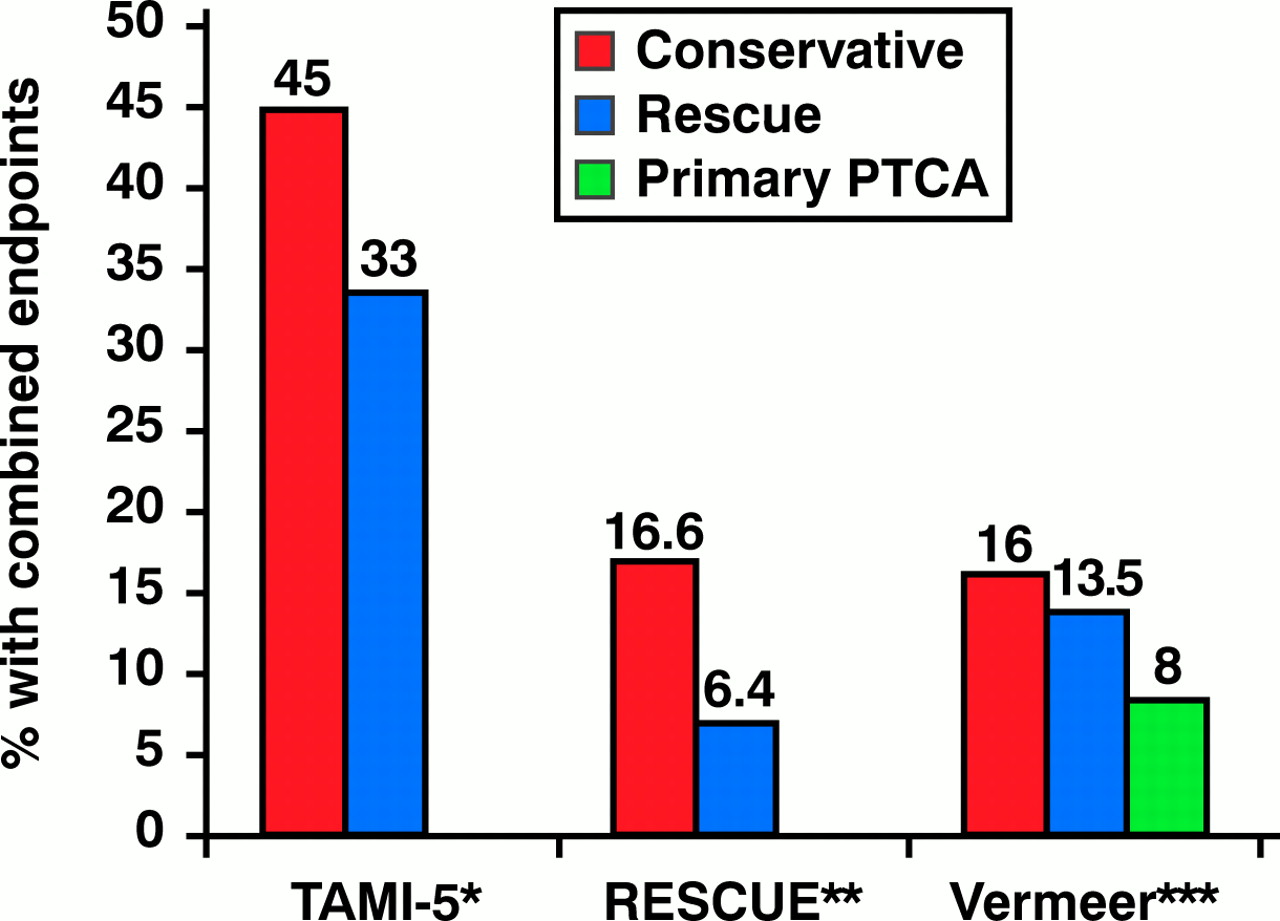
The most favourable data come from the TAMI phase 5 and the RESCUE studies. In both, angioplasty was targeted at those with failed thrombolysis, although randomisation to rescue angioplasty or conservative treatment was performed only in the RESCUE study (fig 4). Other smaller studies have not shown consistent results with some suggesting a worse outcome for patients treated with a strategy of early invasive assessment with a view to rescue angioplasty.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results from three studies of rescue angioplasty: *TAMI-512; **RESCUE13; ***Vermeer et al.14 Combined end points: TAMI-5—death, stroke, reinfarction, reocclusion, heart failure or recurrent ischaemia during hospitalisation (rescue v conservative, p = 0.004); RESCUE—death or congestive failure at 30 days (rescue v conservative, p = 0.05); Vermeer et al—death or recurrent infarction within 42 days (comparison between groups, p = NS).
Considerable gaps in our knowledge concerning rescue angioplasty can be summarised as follows.
The risk:benefit ratio of rescue strategies for allcomers is still unknown. The overall benefits of this strategy are currently being evaluated in the UK in the REACT and the MERLIN trial. The REACT trial has three arms: (1) thrombolysis with rescue angioplasty being offered to those with ECG evidence of failed thrombolysis; (2) thrombolysis with continuing standard conservative care; and (3) thrombolysis with repeat thrombolysis with reteplase offered to those in whom the first lytic agent fails. The MERLIN study compares a rescue angioplasty arm with a conservative care arm.
As discussed above, the optimal timing for a diagnosis of “failed reperfusion” after initial thrombolysis is unknown. Current trials may not answer this question.
The risks and benefits of various adjuncts to rescue angioplasty (stenting, intra-aortic balloon counterpulsation, glycoprotein IIb/IIIa receptor blockers, and embolisation protection devices) are unclear.
The management of patients with TIMI 3 flow at angiography post-thrombolysis is not clear. We have shown that those with a very tight residual stenosis (> 85%) are highly likely to require urgent re-intervention during the recovery period, suggesting that these patients should be offered early intervention, but that those with residual stenoses < 85% (and certainly those with < 75%) do not need immediate intervention.17
Patients with TIMI 2 flow at angiography post-thrombolysis present a particularly difficult problem. Some might have reduced flow because of a tight residual stenosis, but many have no significant residual obstructive lesion. The slow-flow phenomenon is probably associated with problems in the distal vasculature. Some of these may subsequently improve to TIMI 3 flow but others may subsequently reocclude. Whether the various factors that contribute to distal problems can be overcome is unknown. Although local vasodilator agents might help, mechanical devices are unlikely to reverse embolisation that has already occurred, and may even lead to further embolisation.
The duration of follow up needed to demonstrate benefit is unclear. Early risks may be acceptable if the benefits later are evident and sustained. Longer term follow up may be necessary to demonstrate the efficacy of treatment (fig 3). It is possible that any benefit of rescue angioplasty will remain hidden if follow up to only 4–6 weeks or even six months is considered. The timing of crossover from potential harm to potential benefit is unknown.
Coronary artery bypass grafting
There are no randomised trials of surgery in this context, nor are there likely to be. Angioplasty is less risky and easier to deliver. The concept of major surgery in the face of active thrombolysis or combined thrombolytic/antiplatelet treatment is clearly undesirable. Surgery, if indicated, should be delayed as much as possible. Given the lack of knowledge in this setting, the only comments to be made are based on common sense and experience.
In the face of left main stem disease or multivessel disease unsuited to total revascularisation by angioplasty, the culprit artery should be treated where possible, allowing stabilisation and delayed surgery when the risks are much lower. For multivessel disease suited to angioplasty, most operators stabilise the patient by treating the culprit vessel acutely and then deal with other lesions electively at a later date. Where anatomy precludes any attempt at angioplasty, then augmentation of the thrombolytic agent with intra-aortic balloon pumping and possibly with glycoprotein IIb/IIIa agents should be considered and surgery contemplated when bleeding risks have minimised.
Trial acronyms
- GUSTO-1: Global Utilization of Streptokinase and t-PA for Occluded coronary arteries
- MERLIN: Middlesbrough Early Revascularisation for the Limitation of Infarction
- REACT: Rescue Angioplasty versus Conservative Treatment versus repeat thrombolysis
- TAMI: Thrombolysis and Angioplasty in Myocardial Infarction
- TIMI: Thrombolysis In Myocardial Infarction
Future directions
Improve vessel patency with new lytic regimens
A number of approaches are under evaluation. New thrombolytics (reteplase, saruplase, TNK-tissue plasminogen activator, and lanoteplase) have either been introduced into the clinical arena or are under investigation. Results to date, however, do not show a clear advantage over the most commonly used agents. Combinations of different thrombolytics, or combinations of lytics with antithrombotic treatments, have also been studied, but the most promising results have been seen with low dose thrombolytics and glycoprotein IIb/IIIa inhibitors.18 Further trials are underway. The efficacy of thrombolytics can also be enhanced by intra-aortic balloon pumping, but it is not clear whether this could be easily utilised as a routine in all coronary care units.19
Early thrombolysis and angiography for all, with selected rescue angioplasty
In the past, immediate balloon angioplasty for all patients treated with thrombolytics was not shown to be beneficial and there was a suggestion of early harm. However, these studies can be criticised in a number of ways. First, angioplasty was sometimes delivered relatively late after the onset of chest pain. Some patients did not receive antiplatelet treatment in the early stages. Stenting and glycoprotein IIb/IIIa inhibitors were not available, and there was minimal use of intra-aortic balloon pumping. Angioplasty was also performed on patients with patent vessels and good flow, a group who, in retrospect, almost certainly did not benefit from the strategy. However, this approach is currently undergoing reappraisal with earlier (pre-hospital) thrombolysis, early angiography, and rescue angioplasty only where necessary but not as a routine.20 ,21 Early results of this approach are encouraging and suggest that a combination of thrombolysis and appropriate rescue angioplasty may achieve a reduction in mortality after myocardial infarction close to that achievable with primary angioplasty, and clearly offers the potential of increasing the number of patients who might achieve successful reperfusion without having to increase dramatically the facilities for angioplasty. Randomised trials of this strategy versus primary angioplasty are warranted.
Conclusions
In patients with acute myocardial infarction, the direct effect on tissue perfusion depends on mechanical, rheological, metabolic, and haematological factors. Mechanical factors include the occlusion of the vessel, the complexity of the residual stenosis once flow restarts as well as the extent of embolisation of platelet aggregates, thrombus, and atheromatous debris. Metabolic factors include reperfusion injury, the deleterious effect of activated neutrophils and tissue effects of inadequate oxygenation, enzymatic processes, and the presence of toxic metabolites. Haematological factors include the extent and type of thrombus (which themselves may be influenced by the interplay of thrombogenic and intrinsic thrombolytic factors), the haemodynamic status of the patient, and mechanical and other factors which influence rheology. Some factors may be irreversible, but an optimal management strategy for patients with infarction probably requires combinations of measures to overcome some or all of these. Coronary flow should be restored with the least possible embolisation, minimising reperfusion injury and ensuring that maximal blood flow is maintained during the healing process. It is likely that the best approach will require a combination of coronary interventional and pharmacological approaches, together with the ability to support the haemodynamic status of the patient where necessary in the early period.
Currently, however, most patients are treated with either thrombolytic agents or primary angioplasty. Thrombolytic agents on their own do well but not well enough. The re-establishment of coronary flow helps many patients, but for others these agents either do not restore flow, or do it too slowly. Patients with the diagnosis of “failed thrombolysis” fare badly, even if it is diagnosed early (one hour after onset of treatment). A number of methods are available to identify these patients, and although they are imprecise, a convenient and easy-to-use method is to examine the ST segments on the standard 12 lead ECG.
Having made the diagnosis, rescue angioplasty probably offers the best hope of restoring flow and improving the survival of these patients. Overall results are encouraging but the outcomes of larger ongoing trials and an analysis of cost effectiveness are needed before this strategy will be widely accepted.
Current management
A number of guidelines are suggested to aid the management of patients in whom thrombolytic treatment is deemed unsuccessful.
- (1)
- Make the diagnosis only if it will alter management. You cannot be criticised for considering no action with the current state of knowledge, but there probably is some benefit for rescue angioplasty if offered early enough, especially for first time anterior infarction.
- (2)
- Have a policy concerning the timing of the diagnosis. This may need to change as new information becomes available. Treatment considered and offered on an ad hoc basis is not likely to offer patients a good deal.
- (3)
- If rescue angioplasty is chosen, ensure that the management protocol is shared by both those administering the thrombolytic agents as well as those providing angioplasty.
- (4)
- If repeat thrombolysis is considered, monitor the results. More information is needed about the efficacy of this strategy and its associated bleeding risks. It is probably NOT appropriate to use repeat thrombolysis and then to ask for rescue angioplasty when that fails. As further time will have passed and with less myocardium to salvage, rescue angioplasty will probably not carry much benefit. Choose repeat thrombolysis or rescue angioplasty—but not both.
- (5)
- If rescue angioplasty is considered, accept its limitations and the uncertainties outlined above. If used, measures should be taken to minimise time of transfer and “door-to-balloon” times—measurement of both should be monitored in an audit process. Transfer for rescue angioplasty from one hospital to another is associated with an acceptably low risk.
- (6)
- Patients who are more than 8–12 hours into an infarct are unlikely to gain much benefit from a rescue strategy. It is likely (but not proved) that efficacy and cost efficacy of a rescue angioplasty service will be greatest if the rescue angioplasty is offered early.
- (7)
- Enroll patients into trials whenever possible as further information on this common but difficult question is urgently needed.
- (8)
- Widening the scope for intervention in acute myocardial infarction will certainly increase the number of patients achieving TIMI 3 flow. It is likely, but not yet proved, that this will reduce mortality.