
ABSTRACT
Schistosomiasis is one of the major parasitic diseases of the tropics, causing acute and long-term clinical syndromes. Almost all schistosomiasis is now imported from sub-Saharan Africa. This article summarises the aetiology, clinical presentation, diagnosis and management of schistosomiaisis for clinicians in non-endemic countries.
Schistosomiasis (also known as bilharzia) is one of the major parasitic diseases of the tropics, with more than 240 million people in over 70 countries infected.1 90% of these cases are in sub-Saharan Africa and almost all schistosomiasis seen in the UK is now imported from there. Rare cases are still imported from Asia and Latin America, although the incidence in these continents is reducing as a result of successful schistosomiasis control programmes, most notably in China.
Schistosomiasis infection in returning travellers is one of the most common imported tropical infections with potentially serious acute and long-term complications. These complications are preventable if infection is identified early and treated. This article is written for clinicians in non-endemic countries where patients generally have light infections, and summarises the epidemiology, transmission, clinical features, diagnosis and management of schistosomiasis
Transmission/life cycle
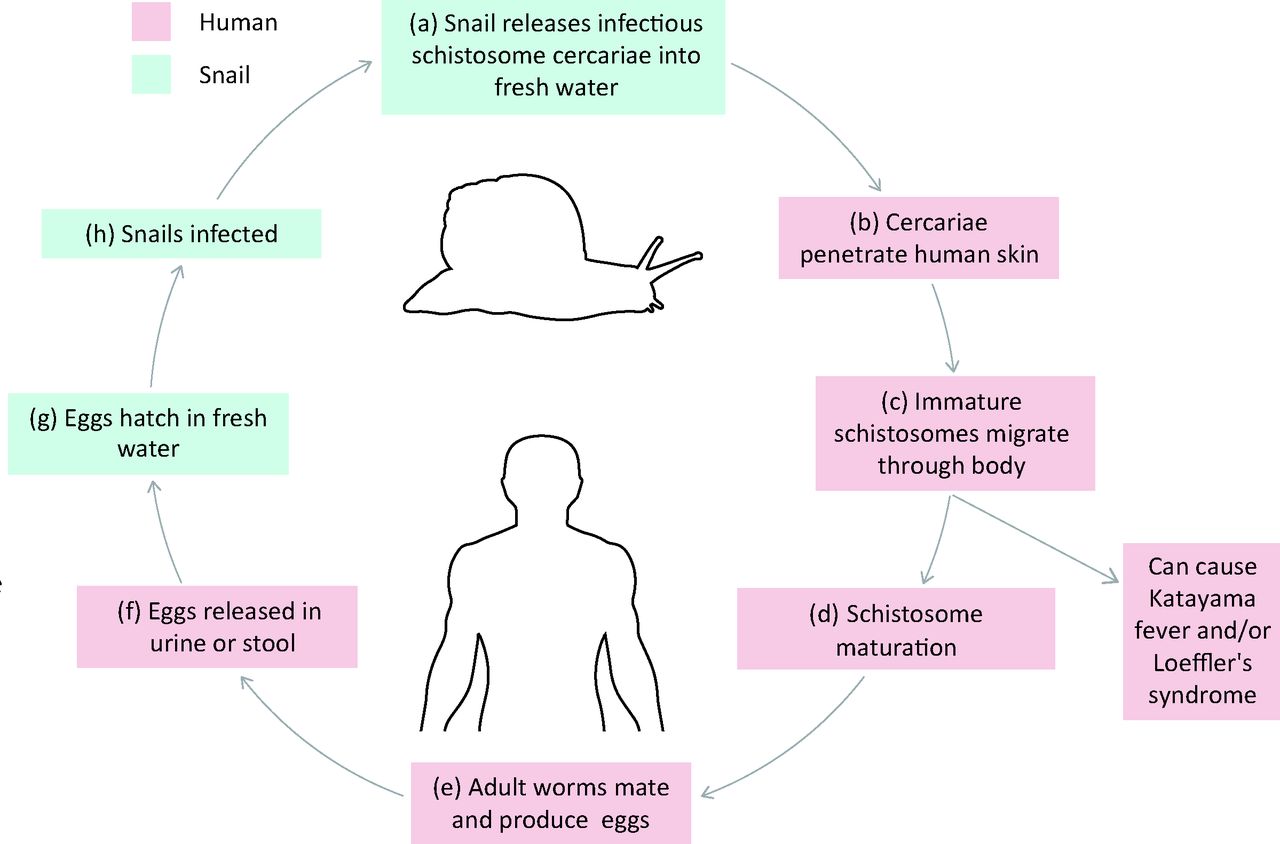
The life cycle of the schistosomiasis fluke is shown in Fig 1. Schistosomiasis infection invariably comes from contact with fresh water, usually by swimming or washing. Travellers may not remember their freshwater contact, so this is not a reliable screening question; in asymptomatic travellers from Africa, up to 11% have been reported as infected.2,3

Schistosomiasis life cycle. Schistosomiasis flukes undergo a lifecycle involving a specific species of freshwater snails, which are the intermediate host. (a) These snails release infectious schistosome cercariae into fresh water, which infect humans. (b) Infection occurs when cercariae penetrate the skin during freshwater exposure. (c) Immature schistosomes migrate through the body, via the circulation and lymphatics to the lungs where they migrate through the pulmonary capillaries into the heart. At this stage they can cause can cause Katayama fever and/or Loeffler's syndrome. (d) Schistosomes mature and ultimately settle in the venous vasculature (the site of which is species dependent: S mansoni and S intercalatum near the colon, S haemotobium near the urinary bladder, and S japonicum and S mekongi near the small intestine). (e) The adult worms mate producing eggs. Mating pairs live on average about 5 years, but this can be much longer (up to 20 years). (f) Eggs are released and excreted in the urine or stool. (g) Eggs hatch on contact with freshwater and can (h) reinfect freshwater snails to complete the lifecycle.
Two species of human schistosomiasis predominate; Schistosomiasis haematobium, which mainly affects the bladder and urogenital system, and S mansoni, which mainly affects the liver and gut. The much rarer species, which are S intercalatum, S japonicum and S mekongi, all present similarly to S mansoni, with the latter two being found in Asia.
Clinical presentation
Schistosomiasis presentation can be divided into a number of syndromes.
Acute schistosomiasis – Katayama syndrome: presents 4–8 weeks after exposure with some combination of fever, malaise, rash (generally urticarial), wheeze, hepatosplenomegaly and significant eosinophilia (often more than double normal eosoniophil counts). Katayama syndrome is an immune complex-mediated response to the immature schistosome migrating through the body.
Asymptomatic/non-specific: over half of proven imported cases of schistosomiasis will be asymtomatic or picked up secondary to an incidental finding of eosinophilia.4 Some patients may report a pruritic rash at the site of infection one day after exposure, commonly called ‘swimmers itch’, which is self-limiting. Others present with low-grade fever, urogenital symptoms or gastrointestinal symptoms. There is benefit to identifying these patients early, as prompt diagnosis and treatment prevents long-term complications.
Haematuria/urogenital: the next most common syndrome in travellers is haematuria, either frank haematuria (patients are likely to present) or microscopic haematuria (incidentally identified). All patients with unexplained haematuria should be asked about African exposure. Gynaecological presentations also occur including vulva schistosomiasis5 and men may complain of haematospermia or lumpy semen. S haematobium causes almost all urogentital schistosomiasis, which carries a slightly increased risk of HIV transmission in discordant couples.
Diarrhoea: schistosomiasis is a rare cause of chronic diarrhoea, and the combination of diarrhoea and eosinophilia should prompt questions about tropical travel.
Chronic infection: the main serious effects are caused by eggs settling in tissues causing permanent scarring of the bladder, liver and urogenital system. This is often cumulative and so the sooner patients are treated the less likely significant damage will have occurred. In heavy chronic infections there is a small increased risk of bladder carcinoma (S haematobium), or liver scarring and/or portal hypertension with ascites (S mansoni or S japonicum). In travellers with light exposure this latter complication is almost unknown.
Neurological schistosomiasis: a very rare but important syndrome due to an immune reaction to egg deposition in the brain and spinal cord. This generally presents as acute lower limb paraplegia after return from Africa. The prognosis is good if treated early.
Key points
Almost all schistosomiasis is now imported from sub-Saharan Africa and is invariably associated with fresh water exposure.
Five species of schistosoma occur, but two cause the vast majority of human disease: S haematobium and S mansoni.
The clinical presentation is diverse; from asymptomatic or mild non-specific symptoms to acute Katayama fever and chronic long-term sequaelae.
The mainstay of diagnosis is microscopy for ova, but eosinophilia and serology can aid diagnosis.
Treatment is with praziquantel.
Diagnosis
In imported cases, with the exception of Katayama syndrome, the gold standard for diagnosis of schistosomiasis in clinical practice depends on finding ova by microscopy on filtered urine (S haematobium) or stool (all other species). In light infections this is highly specific but has a sensitivity of less than 50%. Serology for egg antigen is the standard screening method, which has a sensitivity of over 90% for travellers and slightly less for people originally from endemic countries.6 It is worth doing all three tests as false negatives occur with all diagnostic methods. Dipping urine for blood or identifying eosinopilia are insufficiently sensitive to exclude schistosomiasis, although positive tests should raise the possibility in travellers.7 Occasionally schistosomiasis is unexpectantly found in tissue histology, particularly of bladder or bowel specimens.
Katayama fever occurs before schistosome flukes mature, mate and begin to lay eggs. As the specific tests for schistosomiasis are either finding eggs or serology for egg antigens, schistosomiasis tests are usually negative at this stage. Thus, negative tests do not rule out Katayama fever.
Treatment and follow up
Standard treatment of schistosomiasis is with praziquantel (Box 1). Follow up of schistosomiasis patients is only useful if ova or eosiniophilia were found, to ensure resolution within 3 months. Persisting eosinophilia should trigger investigation for other helminths. Serology for schistosomiasis may remain positive for years following successful treatment, and is therefore not useful for follow up. Most cases of schistosomiasis, once treated, will cause no long-term sequelae, although there should be a low threshold for investigating patients with a history of schistosomiasis and haematuria (including microscopic haematuria) with cystoscopy, due to the slight increased risk of bladder carcinoma in prolonged S haematbium infection.
Box 1. Treatment for schistosomiasis.
- © 2015 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.