
Key learning points
Hypomagnesaemia is a potentially fatal cause of seizures that is easily treated.
Proton pump inhibitors (PPIs) are increasingly recognised to cause symptomatic hypomagnesaemia often after years of highly-compliant therapy.
H2-receptor antagonists do not cause this adverse effect though they may not be effective in controlling symptoms.
Hypomagnesaemia is common in patients who abuse alcohol.
A serum magnesium of less than 0.4 mmol/l is severe enough to warrant intravenous correction.
Case presentation
A 63-year-old lorry driver presented with 36 hours of recurrent vomiting. He had been having two loose motions a day for three months and had become increasingly lethargic. He was previously generally fit and well although a traumatic left arm radiculopathy had prevented him working for seven months. He was taking amlodipine for hypertension and simvastatin for primary prevention. He was also taking omeprazole 20 mg twice daily, commenced four years previously, after an upper gastrointestinal endoscopy showed reflux oesophagitis and moderate duodenitis. Helicobacter pylori was not demonstrated. Discontinuation of the proton pump inhibitor (PPI) was followed by an episode of melaena, so his general practitioner recommenced omeprazole treatment. He was advised to continue on long-term PPI therapy. He drank up to 42 units of alcohol per week.
When examined on admission, blood pressure was 131/88 mmHg, pulse rate 101 beats per minute and cardiovascular, respiratory and abdominal examinations unremarkable. A few myoclonic jerks were noted on neurological examination. Random blood glucose concentration was 10.3 mmol/l. Neutrophil count was elevated (at 15.5×109 per litre), serum concentrations of potassium 3.0 mmol/l, urea 8 mmol/l, and creatinine 229 micromoles/l (normal range 44–133). Three hours after presentation he suffered a generalised seizure. Examination soon after showed a Glasgow Coma Scale of 3/15 improving to 11/15. Arterial blood gas analyses, taken on high flow oxygen, were as follows: pH 7.11, paO2 39.1 kPa, paCO2 5.5 kPa, lactate 2.1 mmol/l, base excess–17.4 mEq/l and arterial bicarbonate concentration 12.3 mmol/l. Further venous blood results became available: total calcium 1.90 mmol/l (normal range 2.2–2.6) and an unrecordably low serum magnesium concentration of <0.10 mmol/l (normal range 0.7–1.0). Computed tomography head scan showed no intracranial lesion.
What is the differential diagnosis and the most likely diagnosis?
The possible causes of seizure included primary epilepsy or a seizure secondary to infection; a structural intracranial lesion, stroke or metabolic derangement and alcohol withdrawal. The raised white cell count supported the possibility of sepsis. When the severe hypomagnesaemia was found, this was sufficient to explain the seizure. PPIs,1,2 loose motions3 and alcohol consumption3 have all been linked to hypomagnesaemia.
What is the initial management?
The patient was fluid resuscitated with up to seven litres of crystalloid per day, for the first two days, (Hartmann's and 0.9% sodium chloride solution) as he was dehydrated and in pre-renal failure. Renal function returned to normal within 24 hours. A rapid intravenous infusion of magnesium sulphate 8 mmol in 100 ml 5% glucose was followed by a further infusion of 20 mmol in 500 ml 5% glucose over 12 hours with further similar infusions on Days 2 and 5. Calcium was replaced with 10 ml 10% calcium gluconate by bolus injection, followed by 10 ml 10% calcium gluconate diluted in 250 ml 0.9% sodium chloride infused over four hours. The latter was repeated on Day 3. The potassium deficit was corrected by infusing a total of 180 mmol potassium chloride with the sodium chloride solution over 48 hours.
Case progression
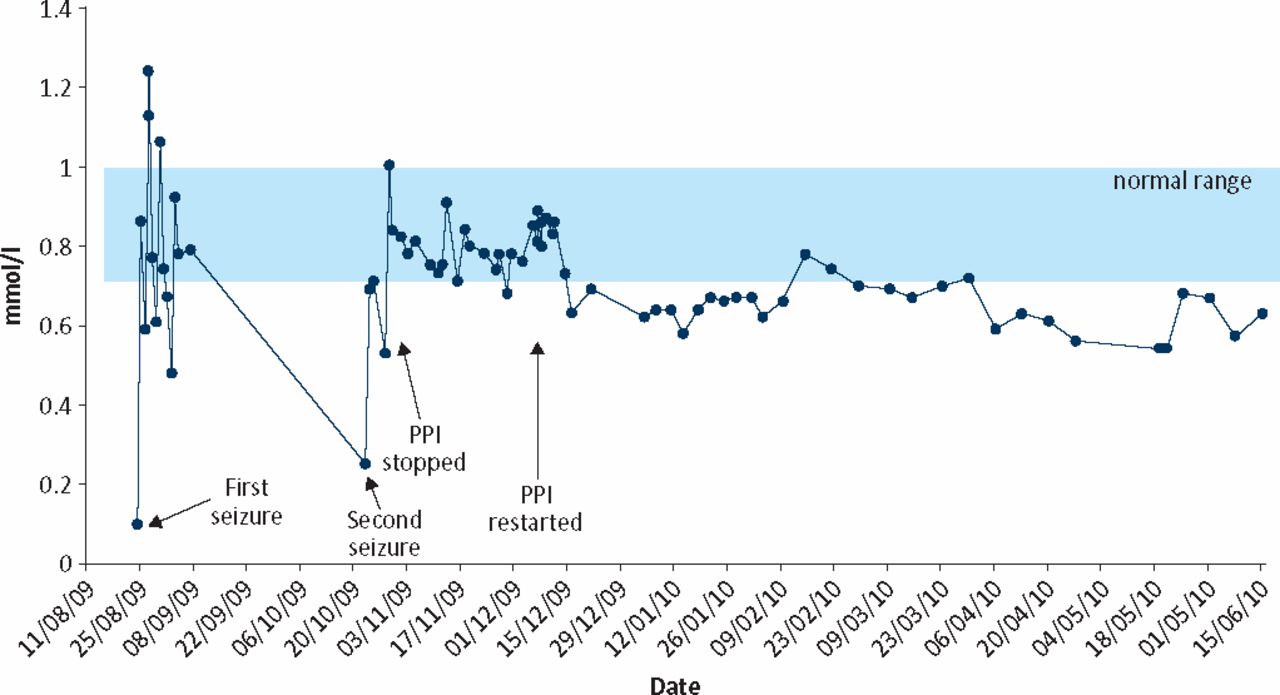
Upper gastrointestinal endoscopy showed erosive gastritis with duodenitis and omeprazole 20 mg twice daily was continued. Twenty-four hour urinary magnesium excretion was low at 0.9 mmol (normal range 1.7–8.4). The patient was discharged two weeks after admission on omeprazole 20 mg twice daily plus Helicobacter pylori eradication therapy, as magnesium concentrations had been stable for five days. He was readmitted after six weeks following a further seizure. Serum magnesium concentration had fallen to 0.25 mmol/l. He received further intravenous magnesium sulphate and was discharged taking oral magnesium glycerophosphate 8 mmol three times per day. Omeprazole was discontinued and ranitidine commenced as there was concern that PPIs were exacerbating the hypomagnesaemia (Fig 1); but as further endoscopy six weeks later showed Barrett's oesophagitis with significant duodenitis, another PPI, (lansoprazole 30 mg) was commenced.

Serum magnesium concentration in the patient. PPI= proton pump inhibitor.
Parathyroid hormone concentration was normal at 55 pg/ml (normal range 15–65), tissue transglutaminase antibodies, stool for ova, cysts and parasites, faecal elastase, colonoscopy, duodenal biopsies and barium follow through were all normal or negative. The patient developed abdominal pain when the dose of lansoprazole was reduced to 15 mg daily, and went back to taking 30 mg. Reduction of the lansoprazole dose to 15 mg eight months later caused abdominal pain so the dose was kept at 30 mg, despite concerns about PPI-induced hypomagnesaemia. Ranitidine aggravated diarrhoea. During nine months of follow up he required one ‘top-up’ infusion of magnesium despite continuing oral magnesium replacement. Codeine phosphate was ineffective at controlling diarrhoea but aluminium hydroxide worked.
Discussion
Magnesium deficiency is associated with weakness, tremor, apathy, psychosis, depression, seizures and cardiac arrhythmias.4 A serum magnesium concentration of less than 0.4 mmol/l is considered severe enough to warrant intravenous replacement.3 PPIs are increasingly recognised to cause hypomagnesaemia, which is often only apparent after years of highly compliant therapy and which resolves on discontinuation of treatment.2 Rechallenge with an alternative PPI causes hypomagnesaemia making this phenomenon likely to be a class effect.2 The hypochlorhydria associated with PPIs reduces the solubility of magnesium salts, possibly causing less magnesium absorption.1 H2-receptor antagonists, such as ranitidine, do not show this effect.
Serum magnesium concentration is controlled by intestinal absorption and urinary excretion. The transmembrane receptor protein channel, TRPM6, is important at low intraluminal concentrations of magnesium, allowing active transport against a gradient, both in the gut and kidney; TRPM7 channels may also play a role. Loss-of-function mutations (heterozygote) of the genes encoding these TRPM6 channels, combined with long-term PPI use may cause magnesium deficiency.2 Substituting ranitidine for PPI in this patient caused magnesium concentrations to rise but they fell again on recommencement. Hypomagnesaemia related to alcohol excess is thought to be due to tubular dysfunction that reverses on abstinence.3 This patient probably had several causes of hypomagnesaemia. The PPI is necessary to control his dyspepsia and oral magnesium replacement causes diarrhoea, making long-term management difficult. Table 1 lists those circumstances in which hypomagnesaemia should be considered.5
When to measure serum magnesium. Adapted with permission from RSM Press.5
Acknowledgements
The authors are grateful to Christopher Anton and Sarah McDowell for reading through the draft and making helpful suggestions.
- © 2011 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.