
ABSTRACT
Stroke is an important cause of death and disability throughout the world. Most strokes are ischaemic, caused by thrombotic or embolic occlusion of blood vessels. The advent of thrombolysis for acute ischaemic stroke has revolutionised the treatment of acute stroke in the developed world.
The benefit of thrombolysis in acute stroke is very time-dependent, with the greatest benefit achieved when administered within 90 minutes of ictus, but trials demonstrating some benefit up to 4.5, and possibly 6 hours. This has revolutionised stroke treatment, with redesign of clinical pathways to try to ensure patients with suspected stroke reach a hospital with a thrombolysis service as quickly as possible. Clinical stroke services need to ensure that all acute stroke patients can be scanned, treated and admitted to stroke units without delay. Future research needs to address the prevention and better management of complications, such as secondary intracerebral haemorrhage and angioedema. In addition, the evidence base for direct intra-arterial intervention such as thrombectomy needs to be established.
Introduction
Stroke is the third most common cause of death and the most significant cause of complex adult disability in the developed world. In 2008–9, direct costs were estimated to be £3 billion annually, with a total economic burden of £7 billion in England.1 The management of stroke has been revolutionised over the last 20 years with advances in acute intervention, rehabilitation and the organisation of services.
Most strokes are ischaemic (around 80%), with vascular occlusion causing cerebral ischaemia and brain damage. It is estimated that for each minute of cerebral ischaemia 1.9 million neurons, 14 billion synapses, and 12 km of myelinated fibres are destroyed,2 underlining the importance of rapid intervention and the ‘Act FAST’3 message. Increased awareness of the symptoms of stroke in the community, immediate paramedic triage to hospitals able to manage acute stroke, rapid assessment by a dedicated stroke team in hospital and immediate computed tomography (CT) scanning has greatly increased the numbers of patients with ischaemic stroke presenting at hospital within the thrombolysis time window, and increased the national percentage of stroke admissions thrombolysed in England from 0.2% in 20064 to 11% in 2012.5
The evidence for intravenous thrombolysis in acute ischaemic stroke
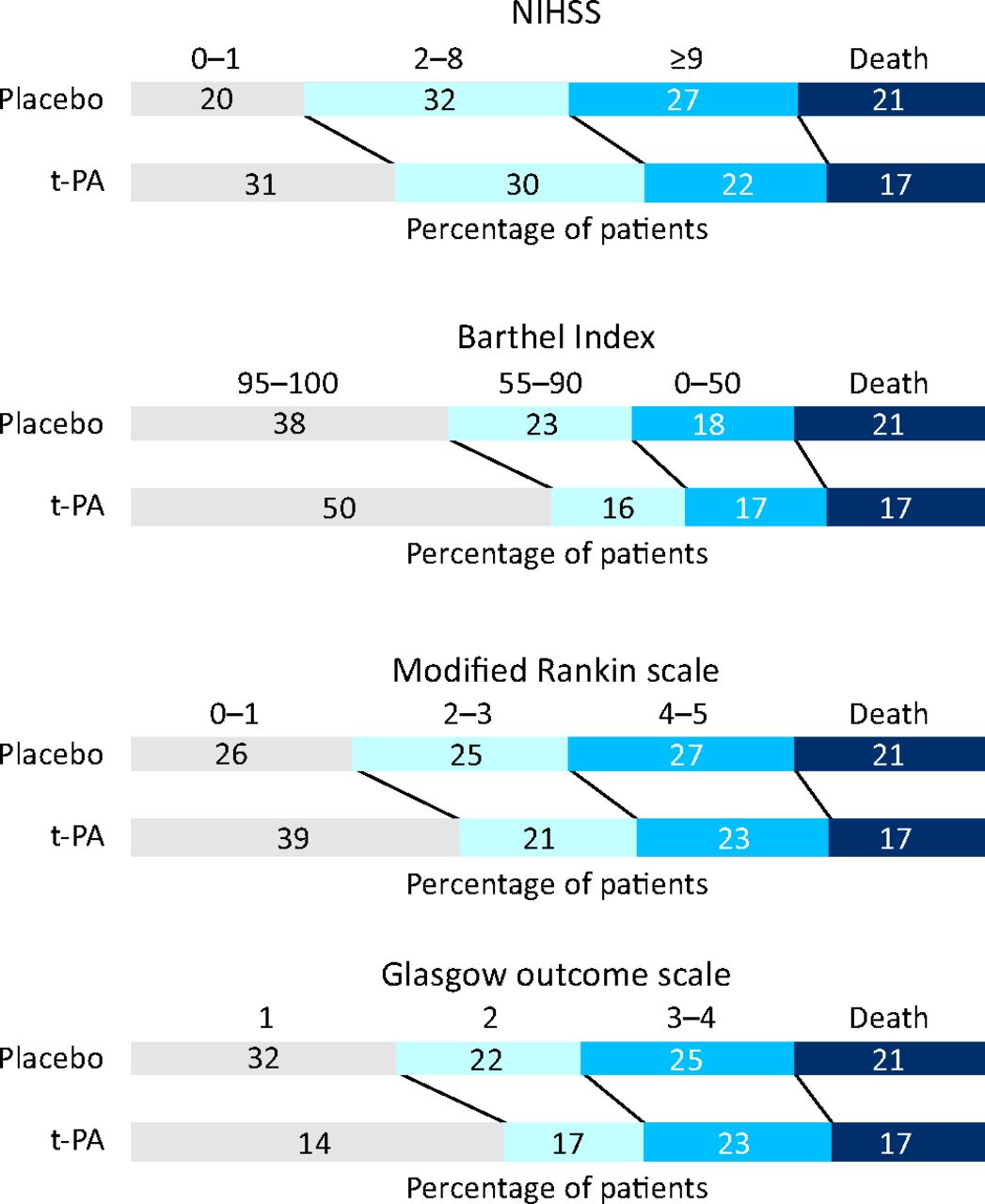
Plasmin is a powerful endogenous protease that is responsible for fibrinolysis. It is formed from its precursor, plasminogen, by plasminogen activators, including urokinase and tissue-type plasminogen activator (t-PA). t-PA preferentially activates plasminogen on the surface of blood clots.6,7 Recombinant tissue plasminogen activator (rt-PA, alteplase) was licensed in North America in 1996 for intravenous use within 3 h of ischaemic stroke in selected patients following publication of the trial undertaken by the National Institute of Neurological Disorders and Stroke (NINDS) in 624 patients.8 This showed overall significant benefit in terms of 3-month disability (Fig 1), despite an excess of secondary symptomatic intracerebral haemorrhage (sICH) in the treated group, and provided the basis for a revolution in the management of acute ischaemic stroke with rapid triage to stroke centres and early imaging.

Outcome at 3 months in part 2 of the NINDS study, according to treatment. NIHSS = National Institutes of Health Stroke Scale. Reproduced with permission from The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group (1995).8
A restricted conditional licence for rt-PA in stroke was granted in Europe in 2002 following the publication of the ECASS9 and ECASS II10 trials and a systematic review of 5,727 patients.11 Full licensing followed the publication of the SITS-MOST (Safe Implementation of Thrombolysis) audit in 2007.12 Similar audits in the USA (STARS)13 and Canada (CASES)14 reinforced the efficacy and safety of alteplase in acute ischaemic stroke administered within licensing indications (under 80 years of age and within 3 h), with a sICH rate similar to that seen in the NINDS study. A pooled analysis of three major trials15 suggested that rt-PA might be of benefit up to 4.5 h post stroke, with the findings confirmed in 2008 with the ECASS III trial of people aged under 80 years treated between 3 and 4.5 h post onset.16
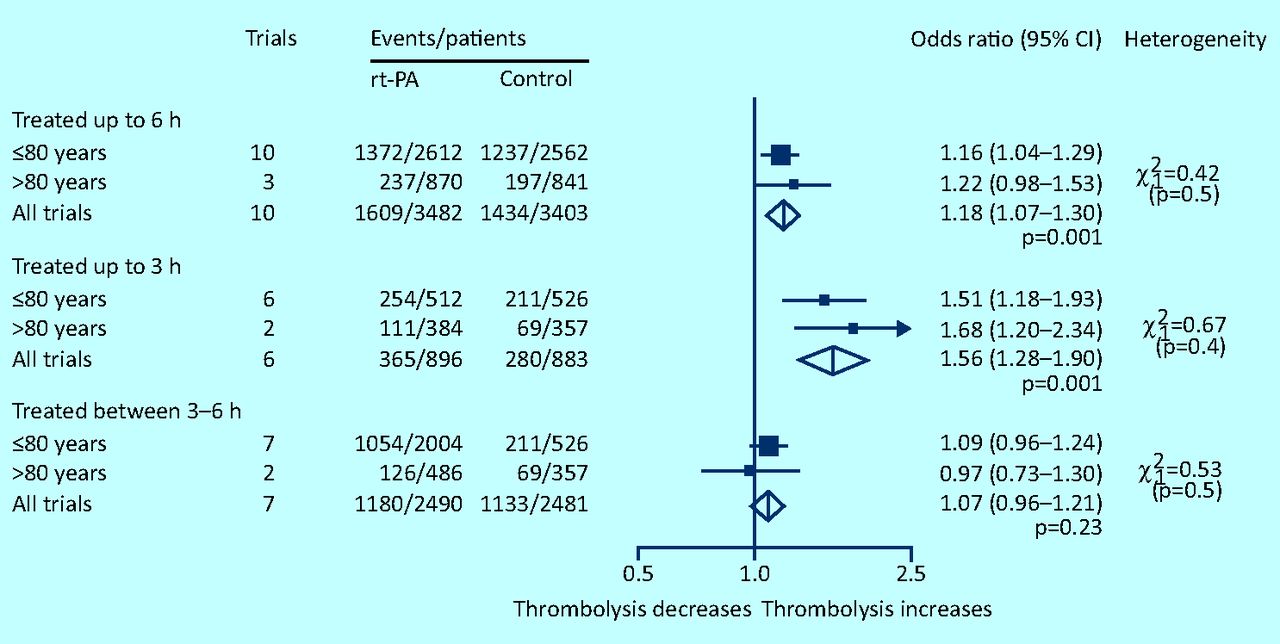
Concerns remained about the safety and efficacy of rt-PA for people treated outside of the licence, in particular, people aged over 80 years (who represent a significant proportion of patients with stroke), and whether rt-PA remained safe up to 6 h post onset, together with the effect of factors such as stroke severity, subtype and comorbidities on outcome. The Third International Stroke Trial (IST-3) was initiated in 2000 and reported in 2012, with the aim of providing more evidence for the use of rt-PA in a wide range of patients. Only 2% of the patients randomised in IST-3 met the European Union licensing requirements of age and time window; 53% were over 80 years. An ordinal analysis showed a significant shift in Oxford Handicap Scale (OHS) scores: common odds ratio (OR) 1.27 (95% confidence interval [CI] 1.10–1.47). More deaths occurred within 7 days in the rt-PA group than in the control group, but there were fewer deaths in this group between 7 days and 6 months, so that by 6 months, similar numbers (27%) had died in both groups.17 The most recent systematic review analysed 12 trials of 7 012 patients and found that rt-PA given up to 6 h post stroke significantly increased the odds of being alive and independent (modified Rankin Scale 0–2) at final follow up (OR 1.12, 95% CI 1.06–1.29, p=0.001) (Fig 2). 18 The benefit of rt-PA was greatest in those treated within 3 h. There was an increase in the numbers of deaths within 7 days, but by final follow up the excess of deaths was no longer significant. Symptomatic intracranial haemorrhage accounted for most of the excess early deaths, and patients aged over 80 years achieved similar benefit to younger patients, particularly when treated early. This data strengthen previous evidence to treat people as early as possible after ischaemic stroke, although some patients might benefit up to 6 h. For the NHS, the National Institute for Health and Care Excellence (NICE) reviewed data within licence in 2012 (currently up to 4.5 h post stroke in people aged between 18 and 80 years)19 and recommended use up to 4.5 h, again emphasising the importance of early treatment.

Effect of rt-PA on the odds of being alive and independent at the end of follow-up, subgrouped by age and time to treatment. Reproduced with permission from Wardlaw et al (2012).18
The Intercollegiate Working Party for Stroke reviewed all of the available data for its 2012 National Clinical Guideline for Stroke, and recommended that all patients should be considered for thrombolysis if presenting within 3 h or if aged under 80 years and presenting before 4.5 h. Those between 3 and 6 h after symptom onset should be considered on a case-by-case basis; the benefits are likely to be reduced but the risks of worse outcome are not significantly increased at this later time point, however, the guidelines emphasise the benefits of early treatment.20 A review of the Stroke Improvement National Audit Project (SINAP) data, published in 2012, analysed process of care and mortality data from over 3,374 people treated with thrombolysis in the NHS, 21% of whom were aged over 80 years. Their care was as timely as younger people receiving treatment, with no higher risk of receiving it, but mortality rates among elderly patients remain high whether treated or not.21
Stroke service design
An effective acute stroke service requires community recognition of stroke symptoms, rapid transport to centres able to manage patients with stroke at whatever time of the day they present, and an efficiently functioning acute stroke team with access to clinical skills, imaging and stroke unit beds.20 In the NHS, change was led until 2013 by the cardiac and stroke networks as part of the Stroke Improvement Programme. A number of models have been established across the UK, with some conurbations such as London and Manchester adopting a stroke centre model, where patients are transported by ambulance from the scene to specialist hospitals, whereas more rural areas have adopted other models such as telemedicine.22 The essential components of a thrombolysis service, whatever the service model, require that people with acute stroke can access specialist expertise, neuroimaging and stroke unit care without delay.
Audit
Regular audit of process and outcome in stroke is essential to maintain and improve services for people with stroke. The UK national stroke audit, the Sentinel Stroke National Audit Programme (SSNAP) (www.rcplondon.ac.uk/projects/sentinel-stroke-national-audit-programme; formerly the Stroke Improvement National Audit Programme [SINAP]), is a web-based national audit that allows clinicians to record data from all stroke admissions throughout their hospital stay and community care up to the 6-month post-stroke assessment. Data is linked with mortality through the Office of National Statistics.
Reducing the hazards of thrombolysis
The main hazard of thrombolysis is sICH, occurring in up to 8% of patients.18 This is the main contributor to the excess of early deaths in treated patients and is commonest in those with hypertension and impaired coagulation. An elevated international normalised ratio (INR) of 1.7 or greater in people on warfarin is associated with a significantly elevated risk of sICH23, so immediate INR estimation is essential in patients taking warfarin. Patients on newer anticoagulants will not have an abnormal INR, so it is essential to take a clear history and avoid thrombolysis in anyone who has taken a new anticoagulant or had heparin within the last 48 h.
Results from the prospective SITS registry12 suggest that high pre-treatment blood pressure (BP) and high BP up to 24 h following initiation of rt-PA are associated with sICH and adverse 3-month outcomes. However, precipitous lowering might feasibly be expected to worsen cerebral ischaemic injury.24 Most thrombolysis trials have excluded patients with BP in excess of 185/110 mmHg,8,16,25 so current guidelines for reduction of high BP in hypertensive patients being considered for thrombolysis patients is based on expert consensus rather than randomised controlled trials (RCTs).26 ENCHANTED is an international collaborative RCT that is seeking to discover whether intensive BP lowering improves outcome and reduces the risk of sICH after thrombolysis (http://clinicaltrials.gov/ct2/show/NCT01422616).
Angioedema is an increasingly recognised side effect of stroke thrombolysis and is reported to occur in 1.3–5.1% of cases.14, 27 For the most part, it manifests as mild, transient, painless hemifacial swelling, usually contralateral to the ischaemic cerebral hemisphere. However, life-threatening oedema, leading to airway compromise, is reported to occur in 0.2–0.8% of all alteplase-treated patients.28 The risk of angioedema is highest in people on angiotensin-converting enzyme inhibitors (ACE-I) because of mast cell degranulation and the release of histamine resulting from bradykinin formation.29,30 People with insular and frontal cortical ischaemia are also at higher risk, which is thought to be related to autonomic derangement secondary to insular cortex damage.27, 31
Clinicians need to be aware of the risk of angioedema when thrombolysing, particularly in those people at risk, and have protocols in place to treat any evidence of angioedema promptly and to effectively manage threatened airway compromise.
Intra-arterial interventions
Despite the evidence for the efficacy of rt-PA in acute ischaemic stroke, particularly when administered within 3 h of symptom onset, there remain a significant number of patients for whom rt-PA does not improve outcome, or where it may be contra-indicated (for example, pregnancy, recent surgery or anticoagulant treatment). Patients who have large-vessel occlusions (carotid T occlusion, proximal middle cerebral artery or basilar artery) may fail to recanalise with intravenous thrombolysis.32
There have been a number of trials of intra-arterial thrombolysis but these are small and generally underpowered.33 Recently, the IMS III trial reported a comparison of intravenous alteplase with or without subsequent intra-arterial intervention, finding similar safety outcomes and no significant difference in functional independence between the two groups.34 It is noteworthy that not all patients had a CT angiogram prior to treatment, few had mechanical thrombectomy, and the study was stopped early and therefore was underpowered.34 There has been increasing interest in mechanical thrombectomy, particularly with newer devices such as TREVO-235 and SWIFT36, and there remains an urgent need for RCT evidence to support the use of intra-arterial intervention. Further evidence of the efficacy and safety of mechanical thrombectomy, and in particular how it compares with intravenous thrombolysis, will be provided by the Pragmatic Ischaemic Stroke Thrombectomy Evaluation (PISTE) trial, which has just commenced recruitment in the UK (http://clinicaltrials.gov/ct2/show/NCT01745692).
Conclusions
The advent of thrombolysis as an effective treatment for stroke has revolutionised stroke medicine over the last two decades. Community awareness, rapid paramedic transfer to hospital, urgent imaging and 24/7 availability of brain imaging and stroke expertise with rapid transfer to stroke units has had beneficial effects for all stroke patients, not just those suitable for thrombolysis. There remains an urgent need to ensure that all stroke services are able to provide rapid, safe and effective stroke care in all areas at all times of day and night to reduce death and disability from stroke.
- © 2013 Royal College of Physicians








{kind=link}
{kind=link}