
An 86-year-old female presented to the emergency department with a history of worsening breathlessness for 3 days and decreased level of consciousness.
On examination, she was drowsy, in respiratory distress, tachycardic and hypotensive. On auscultation of the chest, crackles were heard in the lower zones bilaterally, and a pansystolic murmur was audible over the precordium, with radiation to the axilla. Arterial blood gas analysis showed severe type II respiratory failure.
She had suffered a myocardial infarction 20 years previously.
She was treated with non-invasive ventilation, antibiotics and diuretics. Over the next 24 hours, there was marked improvement in her clinical condition.
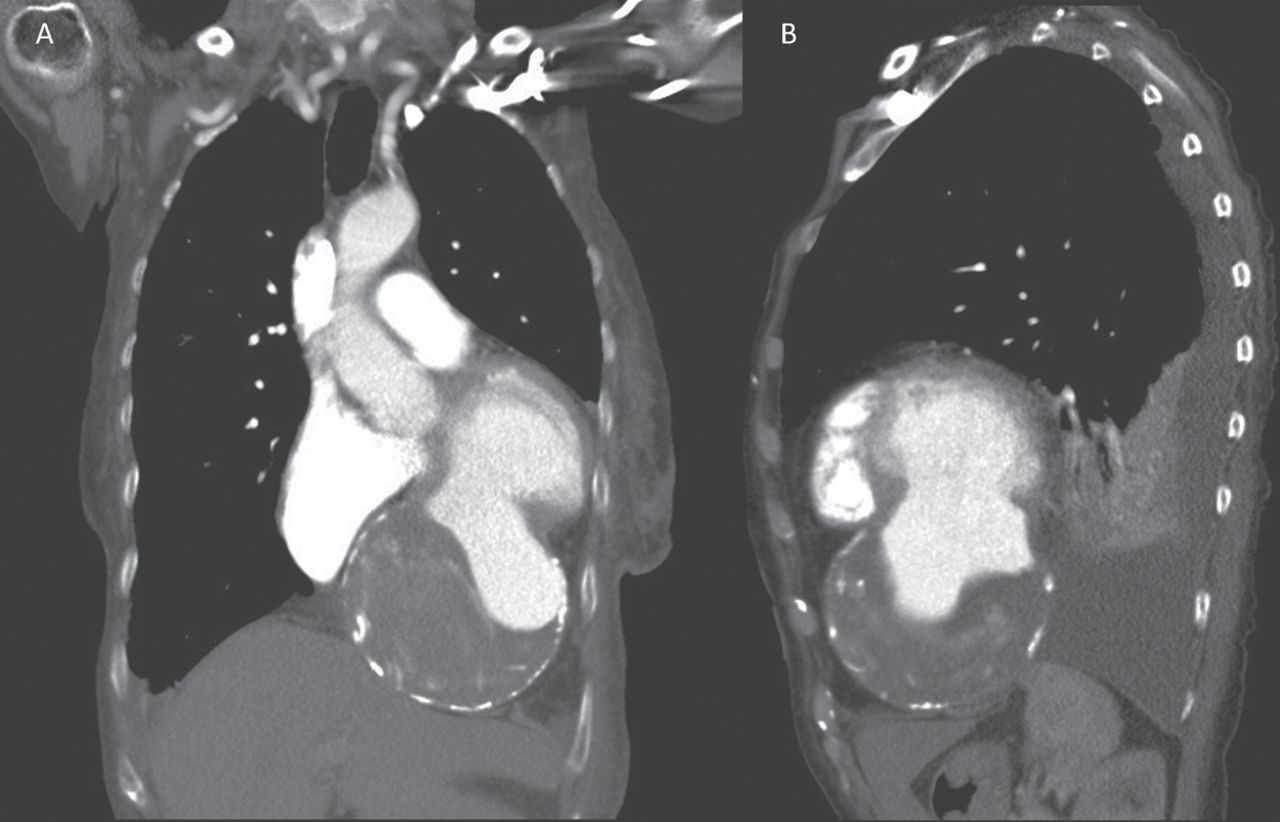
To investigate the cause of her respiratory failure, a computerised tomography scan of the chest was obtained (Fig 1), which showed cardiomegaly and a large left ventricular (LV) aneurysm projecting inferiorly, with a large mural thrombus. It had compressed the right atrium and displaced the inferior vena cava. There was bilateral pleural effusion.
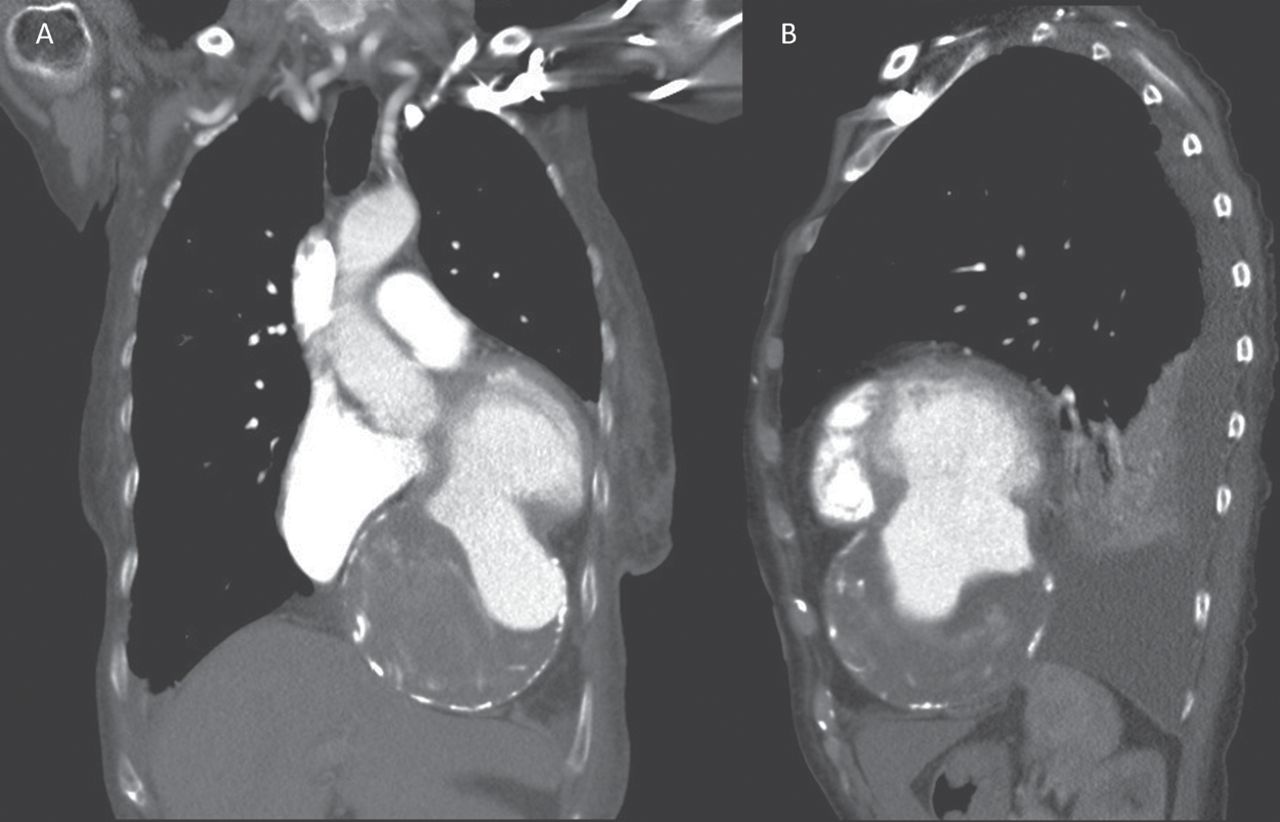
A – coronal contrast enhanced CT chest image showing a large, wide necked, aneurysm projecting inferiorly from the left ventricle. There is mural thrombus and peripheral calcification. B – sagittal CT chest image again showing large left ventricular aneurysm.
The definition of a true LV aneurysm is a discrete ballooning of scarred or fibrotic myocardial wall (often without muscle or containing necrotic muscle) arising from the left ventricle. The involved segment is either akinetic or dyskinetic with paradoxical movement during systole. LV aneurysms often occur as a result of a healed transmural myocardial infarction; however, less common causes include hypertrophic cardiomyopathy and Chagas disease.
A number of serious complications can occur as a consequence of LV aneurysm, particularly heart failure, ventricular arrhythmias and thromboembolism.
The identification of a mural thrombus in patients with post-infarction LV aneurysm indicates anticoagulation therapy should be considered; however, the risk of embolism appears to be low with a chronic aneurysm diagnosed at least 1 month after a myocardial infarction. These thrombi have presumably organised or been enthothelialised and appear to rarely embolise. Therefore, anticoagulation may not be warranted in such patients.1
Treatment is largely aimed at medical management of the complications of the aneurysm, while aneurysmectomy is considered in patients who have intractable ventricular arrhythmias and/or heart failure unresponsive to medical therapy.2
Conflicts of interest
The authors have no conflicts of interest to declare.
Acknowledgements
Written consent was obtained from the patient to publish the clinical details and images in this article.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
Related Articles
Cited By...
- No citing articles found.