
Dermatologic lesions can reflect cutaneous manifestations of systemic diseases thus furnishing clues for a precise diagnostic hypothesis. In the present case, the appearance of fever and reddish lesions on the palms of both hands led the patient to seek medical consultation. The patient was a 30-year-old male with a history of intravenous drug addiction admitted to the emergency room with septic stigmas. Vital signs showed hypotension (90/60 mmHg) and sinus tachycardia (120 bpm). On physical examination, a significant heart murmur was noticed alongside several signs of phlebitis. The palms of the hands and soles of the feet revealed multiple millimetric non-tender red lesions (Fig 1). Blood cultures yielded methicillin-susceptible Staphylococcus aureus and transthoracic echocardiogram confirmed the diagnosis of aortic endocarditis (Fig 2).

Janeway lesions on the sole of the foot (A) and palm of the hand (B).
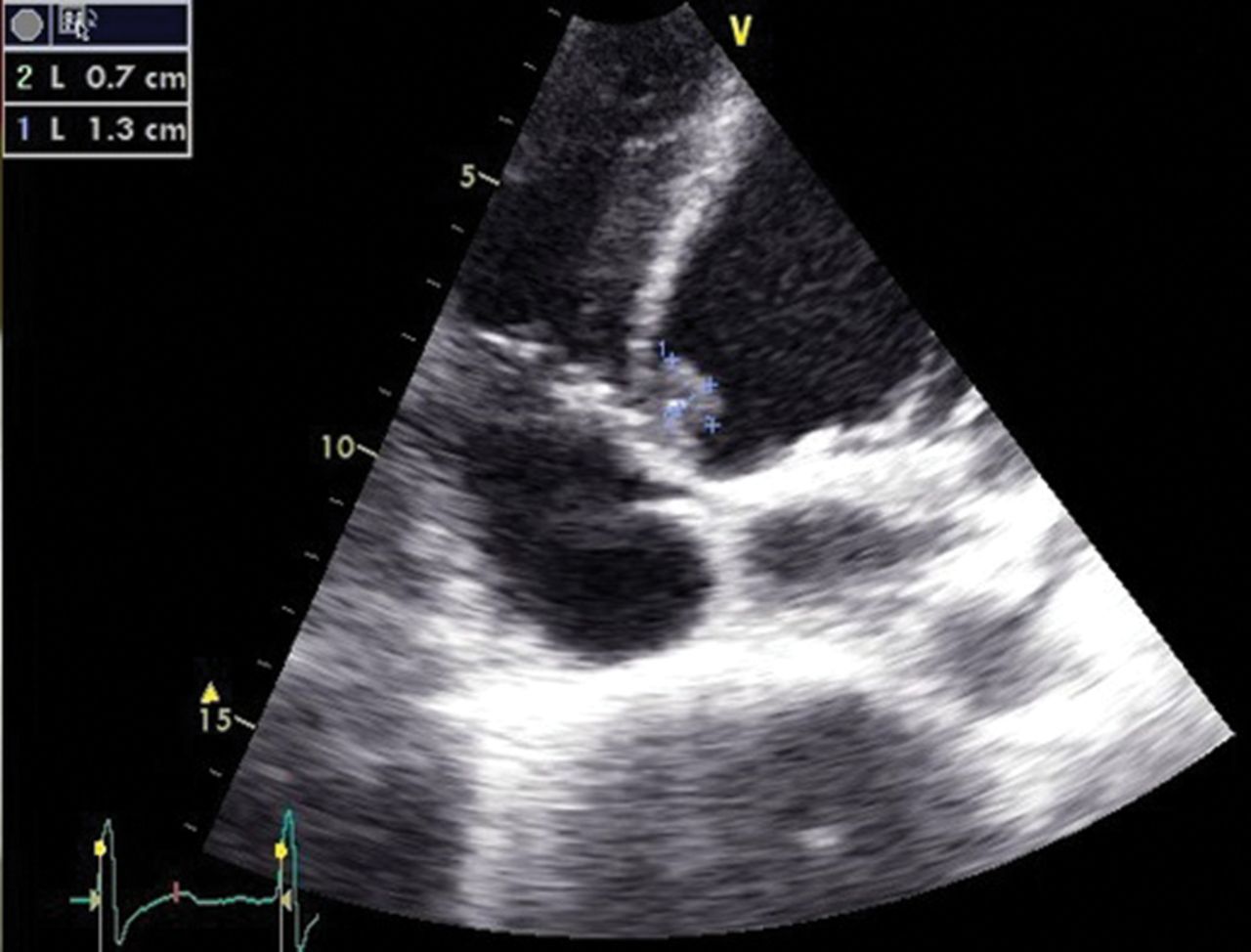
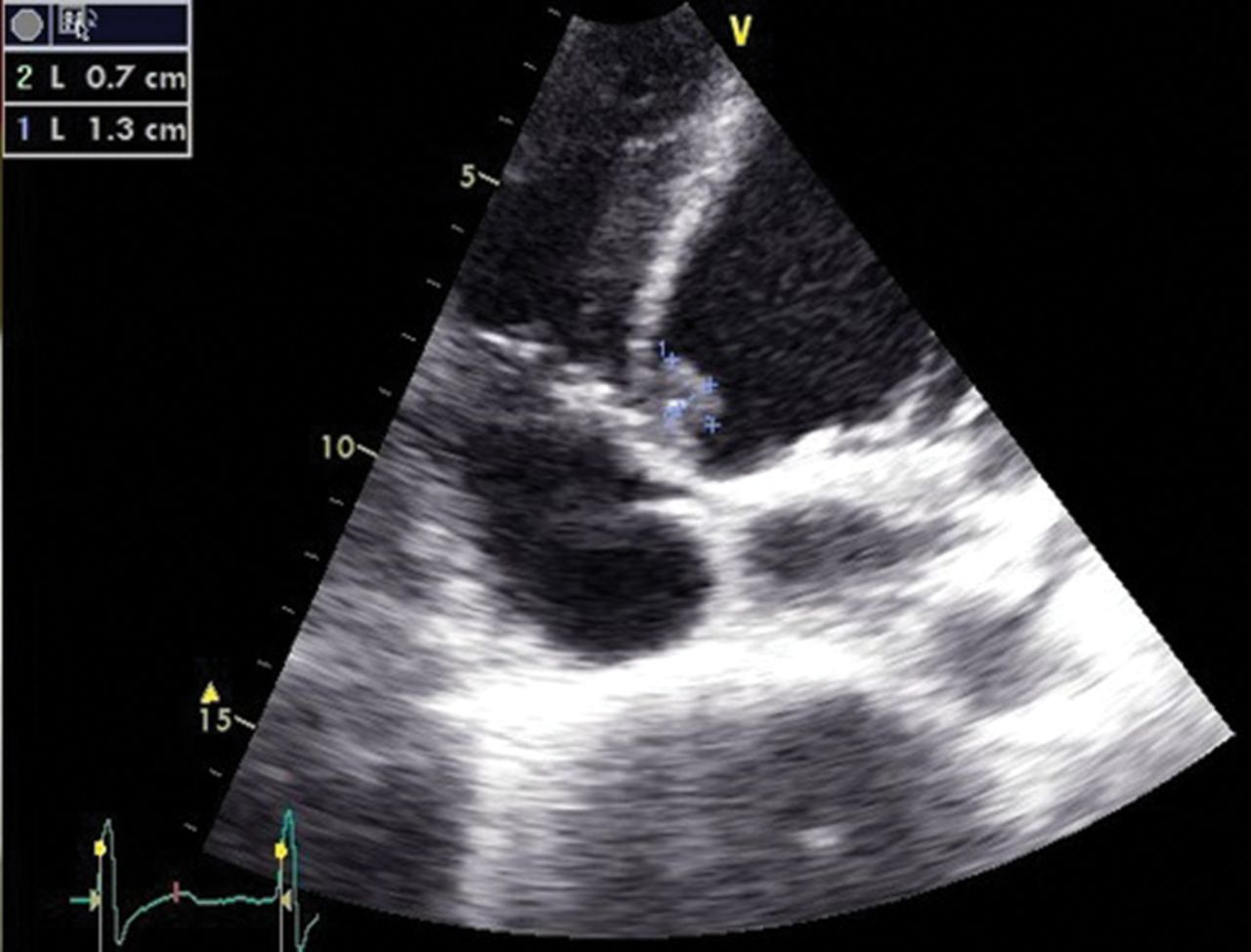
Echocardiogram showing endocarditis vegetation.
Janeway lesions are painless, macular, haemorrhagic lesions that occur most commonly on the palmar surface of the hands and feet. These lesions are non-tender, in contrast to the exquisitely painful Osler’s node. Most histological studies of Janeway lesions have revealed dermal micro-abscesses, without evidence of vasculitis.1 Distinguishing between Janeway lesions and Osler nodes is not that easy. The second ones disappear within a few days without sequelae, occasionally in a few hours, while Janeway lesions tend to last days to weeks before healing completely.2 Bacterial cultures are often positive, leading to the conclusion that these lesions are caused by septic micro-emboli.1 Microbiological cultures of classic dermatological lesions can be performed to assist in therapeutic management and to improve our knowledge.2
Janeway lesions are associated with embolic events other than cerebral emboli. Patients with dermatological manifestations of infective endocarditis have significantly higher complication rates.2 The presence of Janeway lesions, Osler’s nodes or Roth’s spots, although rare, is classically regarded as an excellent clue to the diagnosis of infective endocarditis; in fact, they are all included in the minor diagnostic elements of the modified Duke criteria for endocarditis.4 Although not pathognomonic for endocarditis (leukocytoclastic vasculitis involving the palms on occasion may mimic Janeway lesions3), Janeway lesions are quite specific and a careful physical examination could promptly direct the clinician toward a clinical suspicion of bacterial endocarditis.
Conflicts of interest
The authors have no conflicts of interest to declare.
Acknowledgements
Consent was obtained from the patient for publication of the clinical details and images in this article.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.