
ABSTRACT
Climate change is already expanding the geographic footprint of arboviral infections. In this article we consider the impact of climate change on three arboviruses with particular consideration of the effect on Europe.
Key points
Climate change is already resulting in changing epidemiology of a variety of arboviruses meaning doctors in all clinical settings need to be aware of these infections
The relationship between climate change and arboviral expansion is not linear – changes in land use and housing design may actually result in a decrease in the incidence of arboviruses
Climate change is likely to have a significant impact on human and animal movement further adding to the complexity of arboviral emergence
Tackling the health threat of arboviruses will require a collective approach encompassing vaccines, vector control and the development of therapeutics and diagnostics
Introduction
The earth is warming and there is almost universal consensus that human activities are contributing to this in an unprecedented way.1 In view of this, experts have proposed that we are now living in the Anthropocene epoch, an era where human activities are the dominant geophysical influence on the environment.2 Climate change is accompanied by altered rainfall patterns, flooding and an increased likelihood of extreme weather events. These phenomena are potentially linked to the expansion of the geographic range of permissive vectors and, thus, the potential increase and spread of a variety of arboviral threats.3,4 In contrast, climate change may lead to changes in land use and alterations in human behaviour that may paradoxically reduce the risk of arboviral transmission. In this article, we will consider the implications of climate change on a number of arboviruses with a focus on implications for Europe.
We will discuss viruses transmitted by Aedes mosquitoes, focusing on dengue, viruses transmitted by Culex mosquitoes, focusing on West Nile virus (WNV), and finally tick borne encephalitis (TBE).
Dengue
Dengue is globally the most important arboviral infection, in terms of number of annual infections and global morbidity and currently endangers half the world's population.5 Dengue is a Flavivirus and is transmitted by Aedes mosquitoes. Dengue infection results in a range of clinical presentations ranging from a self-limiting febrile illness through to life-threatening manifestations including shock, organ impairment and occasionally haemorrhage. There are no specific therapeutic agents and currently the only licensed vaccine has limited efficacy, and due to the potential for disease enhancement in flaviviral naïve subjects, most countries have either suspended or are re-evaluating their vaccination strategies.6 The principal vector in tropical countries is the highly domesticated urban adapted mosquito, Aedes aegypti (Fig 1). However, the past few years has seen an expansion in the range of the competent dengue vector, Aedes albopictus. A albopictus has been introduced into Europe and has become established in several countries raising the possibility of dengue transmission.7 Temperature and humidity are significant factors in influencing dengue transmission dynamics – an increase of these may lengthen the dengue ‘season’ in endemic areas and, potentially, promote the establishment of dengue transmission in new areas such as southern Europe or the southern United States. Prediction models (Fig 2) demonstrate the global limits that temperature places on dengue virus transmission, taking into account seasonal variations in temperature and how this differs for A aegypti and A albopictus.8

Photo of an Aedes Aegypti mosquito. Photo courtesy of Cameron Simmons and Lauren Carrington – Oxford University Clinical Research Unit insectary.
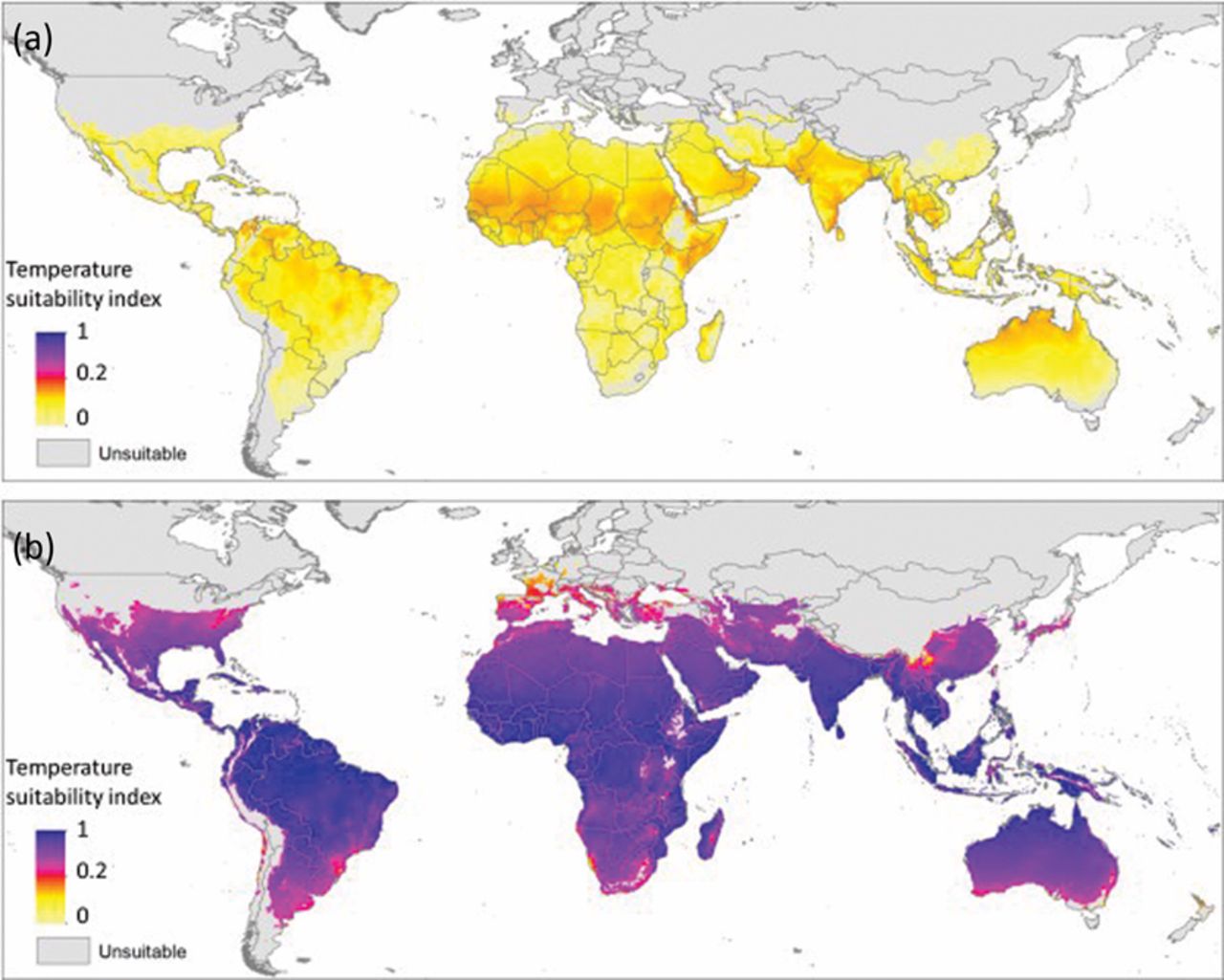
Comparative temperature suitability of Aedes aegypti (a) and A albopictus (b).8 The annualised temperature suitability index (X(T)) normalised relative to the maximum value of both species and plotted on a logarithmic scale. On average the temperature suitability index for A albopictus is around 42 times higher than for A aegypti, meaning that suitability is predicted to be far higher for A albopictus. Reprinted with permission from Brady O, Golding N, Pigott DM et al. Global temperature constraints on Aedes aegypti and A albopictus persistence and competence for dengue virus transmission. Parasit Vectors 2014;7:338.
For Europe, risk mapping projects that further expansion of A albopictus will occur around southern Europe, especially around the Mediterranean coast spreading east to Greece, Turkey and the Balkan countries. Incorporating climate change in these projections, it is suggested the majority of Europe could sustain A albopictus establishment in the next decade, especially countries in western Europe including parts of Germany and the southern UK, due to increased temperatures and rainfall projections. Despite the expansion of A albopictus in Europe, the vector implicated in the outbreak of dengue in Madeira in 2012 was A aegypti, and despite vector control efforts, it has also become established in this setting.9,10
In addition to temperature changes, effects of climate change such as rural flooding may result in significant migration into urban environments.11 This has the potential to further increase the population density in already overcrowded settings, potentially enhancing the transmission risk.12
Comprehensive surveillance systems are required in areas identified to be at risk, combined with innovative vector control measures. Recent advances in biocontrol utilising the intracellular bacterium Wolbachia, which is able to interfere with viral replication of a wide variety of arboviruses, is an exciting area.13 Successful and sustained introduction of Wolbachia into wild Aedes mosquito populations in field sites in Australasia have been demonstrated.14 Recent evidence suggests this could have a significant impact on dengue transmission, as, since mass releases started in 2011, there have been no dengue outbreaks despite the increase in imported cases into the area.15 Results from large-scale trials are awaited from Indonesia and Vietnam.16
West Nile virus
WNV is another Flavivirus, however its predominant vector is Culex mosquitoes, in particular Culex pipiens.17 Although the predominant route for transmission is through the bite of an infected mosquito, transmission can also occur through handling of blood or tissues of infected animals and also through organ transplant and blood transfusions. There are no antivirals for WNV, and only an equine vaccine exists. WNV is maintained through a zoonotic cycle between mosquito and birds. Various species of bird are reservoir hosts and most species do not display symptoms, however it can be pathogenic for certain species particularly members of the crow family. Humans and horses are dead-end hosts, meaning they can become infected but do not contribute to the transmission cycle. More than 80% of infections are asymptomatic, and the remaining usually present with a self-limiting infection with symptoms of fever, headache, vomiting and lymphadenopathy. Neuroinvasive infection occurs in less than 1% of cases but is associated with a high morbidity and a significant mortality rate.18 Neuroinvasive disease includes a spectrum of syndromes from meningoencephalitis through to flaccid paralysis. Severe illness can occur at any age, but more frequently occurs in older age groups and immunocompromised patients, particularly transplant recipients.
WNV was prevalent throughout Africa, parts of Europe, Middle East, West Asia and Australia, and since 1999, when it was introduced into the USA, the virus spread throughout the American continent and is now widely established from Canada through to Venezuela.19
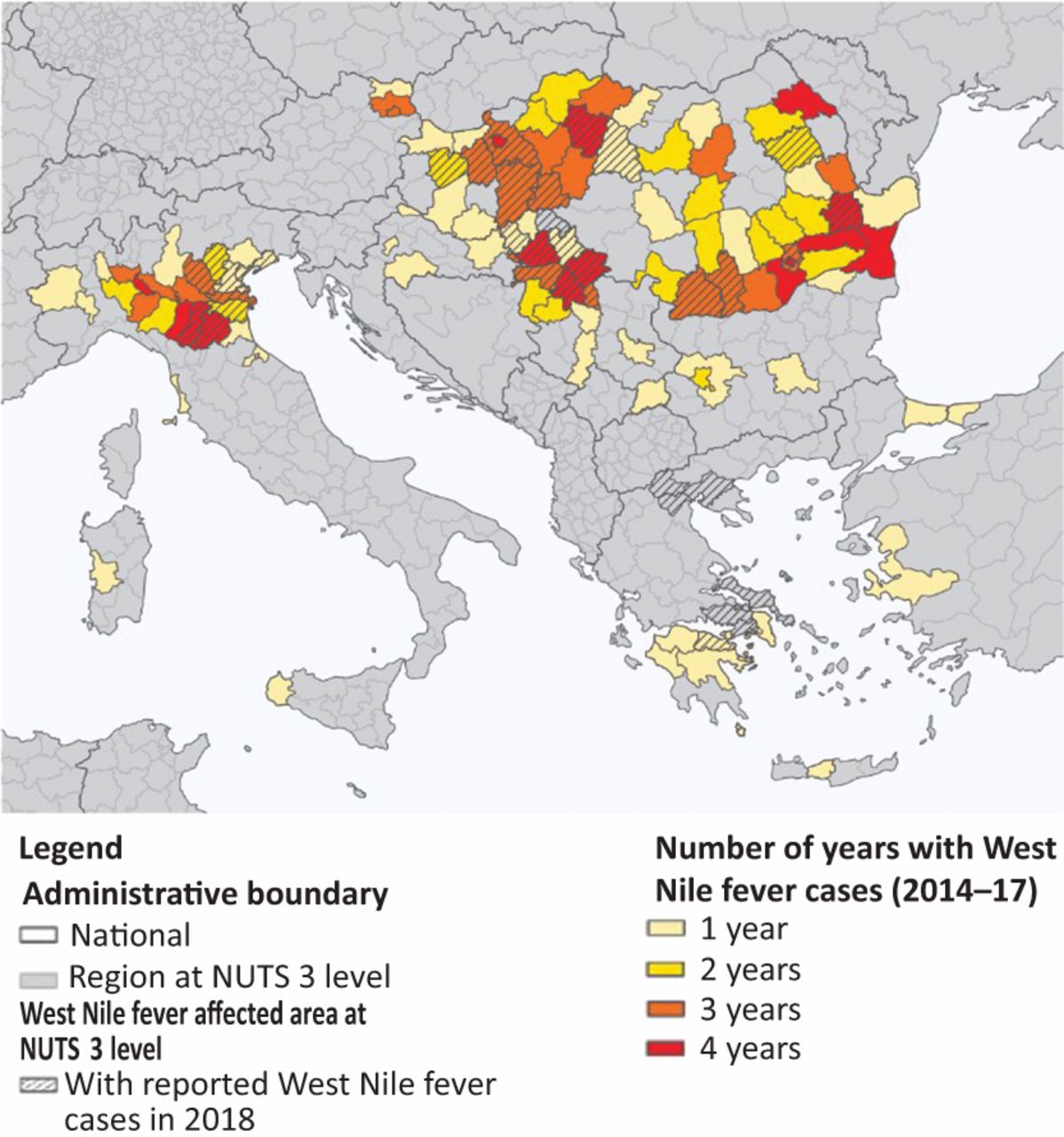
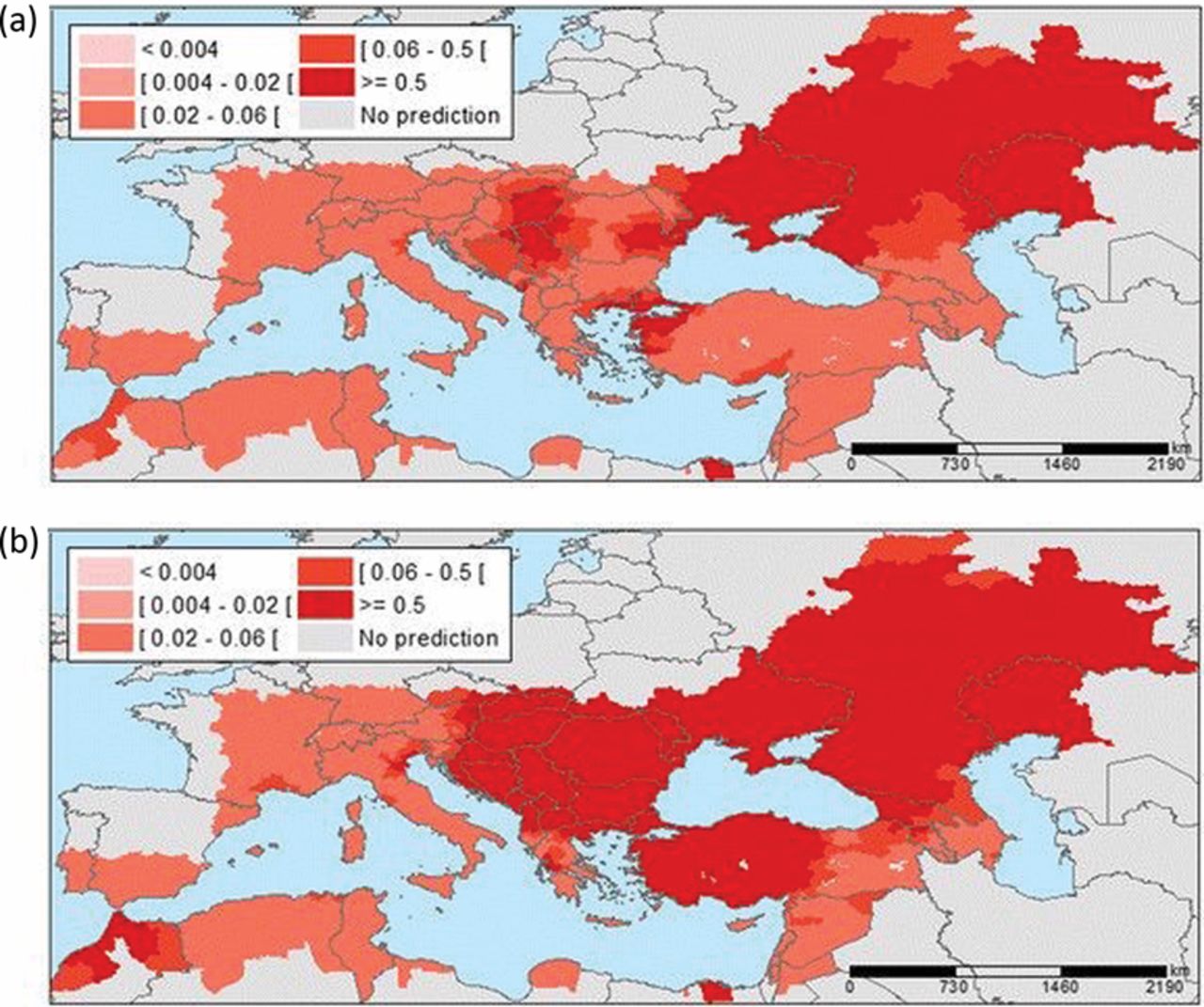
WNV is already established in parts of Europe (Fig 3) and competent vectors are present throughout the continent.20 Recent outbreak sites have been on major birds’ migratory routes, with the largest recent outbreaks in the last two decades occurring in Greece, Israel, Romania, Russia and USA. It is possible that changes in bird migratory patterns secondary to climate change may result into changes to WNV epidemiology, in addition to the expansion of the Culex mosquito vector. Risk projection maps estimate large parts of Europe will be suitable for West Nile virus transmission by 2050 (Fig 4). Robust surveillance systems are essential for the real-time monitoring of WNV cases to ensure that public health systems receive early warnings about the onset of a potential outbreak and any unusual seasonal patterns, to trigger local outbreak response teams and vector control.

Distribution of regions reporting at least one case of West Nile fever, Europe, 2014–2018.26 Reprinted with permission from Haussig JM, Young JJ, Gossner CM et al. Early start of the West Nile fever transmission season 2018 in Europe. Euro Surveill 2018;23:1800428.

Predicted probability of districts with West Nile virus (WNV) infections for (a) 2025 and (b) 2050.27 Predicted probability of districts with West Nile Virus infections based on July temperatures for 2025 and 2050. The maps show a progressive increase of areas with a higher probability for WNV infections, particularly at the edges of the transmission areas. Reprinted with permission from Semenza JC, Tran A, Espinosa L et al. Climate change projections of West Nile virus infections in Europe: implications for blood safety practices. Environ Health 2016;15(Suppl 1):S28.
Tick-borne encephalitis
TBE is a Flavivirus transmitted by Ixodes ticks, principally Ixodes ricinus. TBE typically causes a biphasic illness with an initial viraemic phase that is indistinguishable from other viral illnesses followed by a secondary phase where neurological features predominate.21 TBE is endemic in Europe and it is likely that climate change has already impacted its transmission dynamics.22 Higher temperatures result in faster tick development cycles and higher population densities. In addition, warmer climates lengthen the duration of tick active periods and promote the expansion of the vector into higher altitudes. This has been seen in Sweden where there has been an increase in TBE cases since the mid-1980s – this increase correlates with shorter, warmer winters and, thus, an increase in the potential disease transmission season.4 In addition, in the Czech Republic, TBE transmission is occurring at higher altitudes – again, this is linked to increased temperatures that support the establishment of the vector in new, previously hostile areas.23 However the impact of global warming and TBE transmission is not entirely clear-cut. I ricinus typically feeds on roe deer. Sweden had a very harsh winter in 2010–2011 which resulted in a reduction in the deer population. This meant that ticks fed on small rodents that were more likely to be TBE viraemic and thus infectious to ticks.24 This resulted in an increased number of TBE cases. In addition, the expansion of ticks closely correlates with the expansion of roe deer which is partly due to the demands of game hunters. While there is little doubt that climate change has increased the rates of TBE transmission, it is clear that the dynamic is more complex than a simple case of cause and effect.
Conclusions
Successful arboviral transmission requires optimal environmental conditions for both vector and virus. Climate change is likely to contribute to the expansion of the outer limits of arboviral transmission. Using the most extreme climate scenarios modelling experiments suggest that there may be dengue transmission in the UK summer by 2100.25 What is perhaps more likely is occasional autochthonous transmission events resulting from a viraemic individual travelling to a non-endemic area inhabited by permissive vectors. This has already been seen with outbreaks of dengue and chikungunya in parts of southern Europe. Additionally, climate change is likely to result in significant human movement with the increased emergence of ‘climate refugees’. This new phenomenon will have associated health challenges that will go beyond infectious diseases. While climate change is certainly a factor in the increased rates of arboviral transmission it should not be viewed in isolation – other contributing factors such as human behaviour, human movement and land use (which may themselves be affected by climate change) are also likely to play a role.
Conflicts of interest
The authors receive consulting fees from Janssen pharmaceuticals for their work on dengue antiviral development.
- © Royal College of Physicians 2019. All rights reserved.








{kind=link}
{kind=link}
{kind=link}
{kind=link}