
ABSTRACT
Background Holistic approach to the clinical management pathway for malignancy of undefined primary origin (MUO)/carcinoma of unknown primary (CUP) patients remains an unmet clinical need. To address this, an MUO/CUP service was implemented during conception of a new acute oncology service (AOS).
Methodology Over a comparable 17 months’ duration, patient outcomes pre-MUO/CUP service implementation was retrospectively analysed and compared prospectively with post-service implementation database. Performance measures of MUO/CUP service were compared against national recommendations.
Results In the retrospective cohort (n=32), median age was 71.5 years and median length of hospital stay (LOS) was 11.25 days. In the prospective cohort (n=42), median age was 75.5 years, median LOS was 7.75 days (p=0.037). Post-service implementation, 100% patients were discussed in MUO/CUP multidisciplinary team meeting; 96% of inpatient referrals were reviewed by oncology within 24–48 hours. In the prospective group, median overall survival (OS) was 73 days vs 35 days in the retrospective group (p=0.045; hazard ratio (HR) 1.61). Out of 20 patients suitable for anti-cancer treatment in the prospective group, 85% were treated within 31 days from the decision-to-treat; 90% were treated within 62 days of referral. Within the prospective group, median OS was 214 days in the treated sub-group, compared with 44 days in patients receiving best supportive care only (p<0.0001; HR 3.19).
Conclusion Timely specialised input from AOS with a dedicated MUO/CUP team can achieve enhanced patient-centred and healthcare-centred outcomes, both in terms of survival and hospital stay. However, heterogeneity in both retrospective and prospective study groups, as well as discrepancies in coding, makes direct comparison between both groups challenging.
Introduction
Historically, enigmatic terminology ‘carcinoma of unknown primary’ (CUP) has been loosely used for patients diagnosed with cancers of unknown primaries based upon limited investigations. In the UK, the National Institute for Health and Care Excellence (NICE) has now defined a clinical spectrum of this disease.1 Malignancy of undefined primary origin (MUO) refers to metastatic cancers that do not have immediately identifiable primary site on initial work-up. Once tissue diagnosis has confirmed epithelial/neuroendocrine malignancy, patients are deemed to have ‘provisional carcinoma of unknown primary’ (pCUP) and should be referred to specialists. If identified to have clinico-pathological parameters suggestive of a tumour site-specific (TSS) disease (overt or occult primary), TSS therapies can be offered. Prognostic stratification into favourable (approximately 20%) and unfavourable (approximately 80%) sub-groups take into account multiple parameters like age, performance score (PS), tumour differentiation, morphology, sites and number of metastases, as well as biomarkers like lactate dehydrogenase (LDH) and albumin.2–5 Confirmed carcinoma of unknown primary (cCUP; primary tumour origin unknown despite exhaustive investigations) usually have aggressive chemotherapy/radiotherapy resistant biology and, consequently, poor clinical outcomes with reported median survival being 4–12 months.2,3,6
Seminal reports published by the National Confidential Enquiry into Patient Outcome and Death (NCEPOD; 2008) and the National Chemotherapy Advisory Group (NCAG; 2009) were critical in identifying fragmented pathways for acutely unwell cancer patients with poor patient experience.7,8 This led to the conception of the acute oncology service (AOS). An integral part of AOS is optimal management of patients with MUO/CUP. Subsequent to NICE guidelines mandating that all cancer centres should have a MUO/CUP service, several cancer networks have developed their own service model while many others have struggled to set up a robust and sustainable service.1 This is mainly due to scarcity of resources in terms of workforce and finance, perception that this patient cohort is encompassed within multiple TSS groups, as well as clinical complexity which demands protected time and broad experience.
Methodology
MUO/CUP service setup
Funding to support consultant oncologists and a clinical nurse specialist (CNS) for AOS in North West Cancer Centre (NWCC) was confirmed by Northern Ireland Health and Social Care Board Public Health Agency in 2015. Inclusive of AOS posts, 12 consultant oncology posts were funded in the new cancer centre, changing the historical visiting model to that of resident consultant model in February 2015. By the time AOS was set up in 2017, eight substantive consultants were in place, and one more has joined since. Significant preparation was carried out, which included promotional posters and a dedicated trust intranet website. The AOS went live in June 2017 and started accepting hospital inpatient referrals. In parallel, a new MUO/CUP service was developed, led by medical oncology and supported closely by clinical oncology, palliative care team (PCT), pathology and radiology. An acute oncology CNS acted as the MUO/CUP ‘key worker’. The service consisted of weekly multidisciplinary team meetings (MDMs), an inpatient hospital liaison service, dedicated outpatient clinics and fast-track pathways for TSS MDMs. Referral and clinical management guidelines were adapted from national recommendations for usage by the wider trust (supplementary material S1 and S2).
Strict inclusion and exclusion criteria were identified (Table 1). New AOS e-referral was utilised for CUP referrals (supplementary material S3).
Inclusion and exclusion criteria for referrals to malignancy of undefined primary origin/carcinoma of unknown primary service
Data analysis and performance measures
For comparative purposes, retrospective data was compiled from patients coded as ‘malignant neoplasm without specification of site’, from October 2015 to February 2017 (17 months). This data included patient demographics, survival and treatment outcomes. A prospective histopathological database was constructed to capture data for all CUP service referrals from its inception in June 2017 until October 2018 (17 months). All patients referred to the MUO/CUP service also had their electronic/paper records reviewed.
Additional performance measures were utilised: median length of inpatient hospital stay (LOS), number of patients receiving anti-cancer treatment, number of patients receiving PCT input, median overall survival (OS) and place of death.
In the prospective database, other outcome measures were analysed to reflect on different aspects of pathway. These included:
time from referral to first oncology specialist review/input
time from decision-to-treat (DTT) to first treatment
time from referral to first definitive treatment
time from referral to first inpatient review
time from referral to first outpatient review.
These data were also compared against nationally recommended guidelines on cancer waiting time performance measures and NICE recommendations on CUP.1,9
Study approval from the audit department and Trust Acute Services was obtained. Formal ethics approval was not required as this study was not classified as research project.
Statistical analysis
Univariate analysis of patient outcome data was performed using Fisher’s exact test. Mood’s median non-parametric hypothesis test was applied to determine significance in relation to median LOS. Kaplan–Meier survival analysis was generated and the log-rank (Mantel–Cox) test employed to determine significance. A p<0.05 was considered significant.
Results
Patient outcome data
In the retrospective cohort, 32 patients in total were coded as MUO/CUP (14 female; 18 male). AOS was not active at this stage. Median age of this cohort was 71.5 years. For 26 patients, PS was unrecorded or unavailable (supplementary material S4 and S5). For 11 patients, oncology input was sought regarding their clinical care. Out of 32 patients, 12 patients had tumour sites identified, seven patients had cCUP and 13 patients were classified as MUO with no available tissue diagnosis (Table 2). Only three patients in this group (one with identified tumour site, one with MUO without any tissue diagnosis and one with squamous cell carcinoma of unknown origin) received anti-cancer treatment, while the majority (n=29) received best supportive care (BSC). Twenty-seven out of 32 patients received PCT input (Table 2).
Comparative analysis between pre- and post-carcinoma of unknown primary service
In the prospective cohort, out of total AOS referrals (n=210), one-fifth were MUO/CUP patients (n=42). Of the 42 patients, 17 were female and 25 were male. Median age across the group was 75.5 years. Sixteen patients had a PS of 0–2 and 19 had PS of 3–4 (supplementary material S4). Over 50% of patients (n=22) had a tumour site identified, while six patients were diagnosed with cCUP. Twelve patients were classed with MUO and were considered too frail/unwell to have further tissue diagnosis and two patients were diagnosed with a non-epithelial malignancy (Table 2). Twenty patients in this cohort (15 identified with tumour sites, one with cCUP, two with MUO without any tissue diagnosis and two with non-epithelial malignancy) received some form of anti-cancer treatment (Table 2).
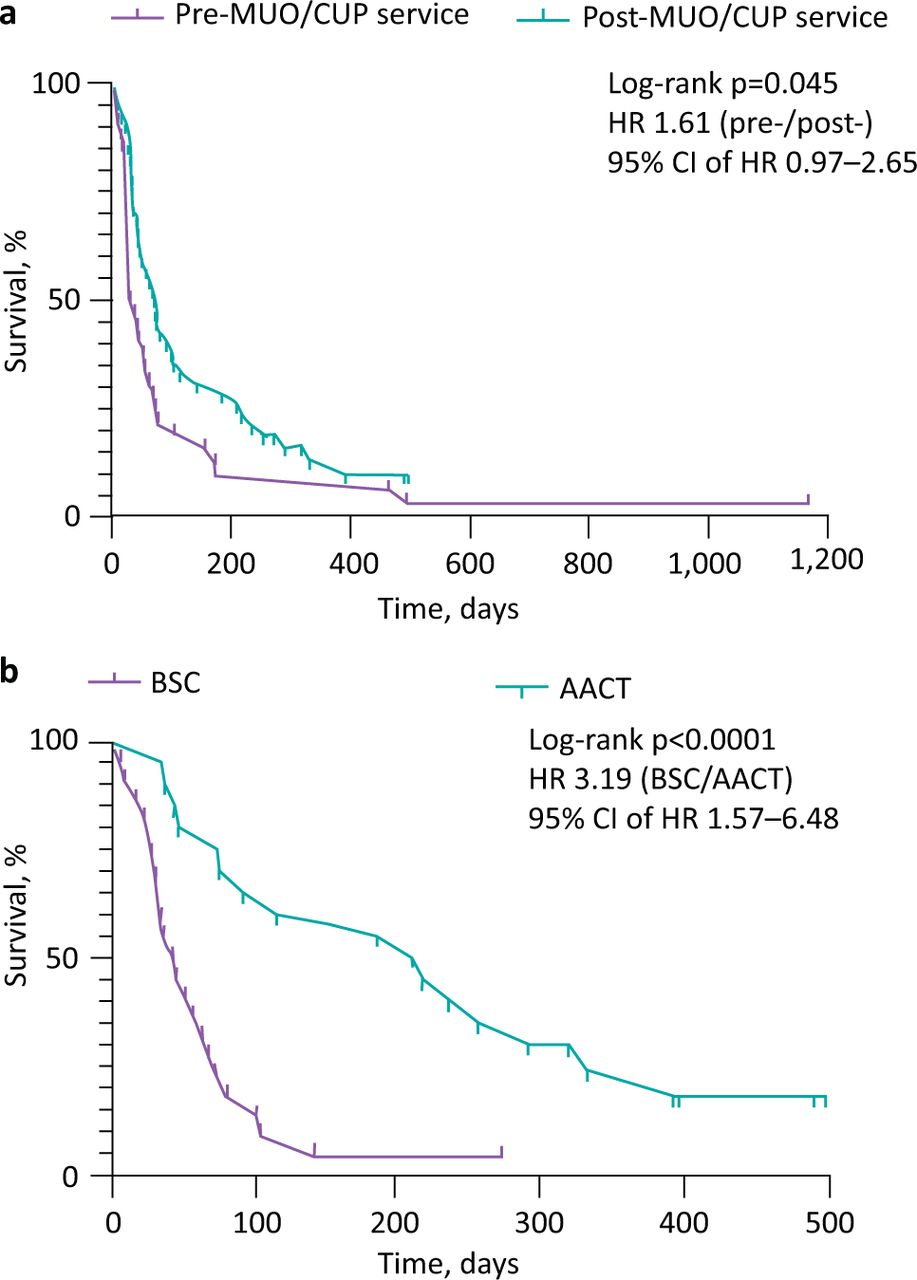
Median LOS was 11.25 days in the retrospective cohort versus 7.75 days in the prospective cohort (p=0.037; Table 2). Median OS was 35 days in the retrospective cohort versus 73 days in the prospective cohort (p=0.045; hazard ratio (HR) 1.61; 95% confidence interval (CI) 0.97–2.65; Fig 1a). Specifically in the prospective cohort, median OS was 214 days in patients who received some form of anti-cancer treatment, compared with 44 days in patients who received BSC only (p<0.0001; HR 3.19; 95% CI 1.57–6.48; Fig 1b).
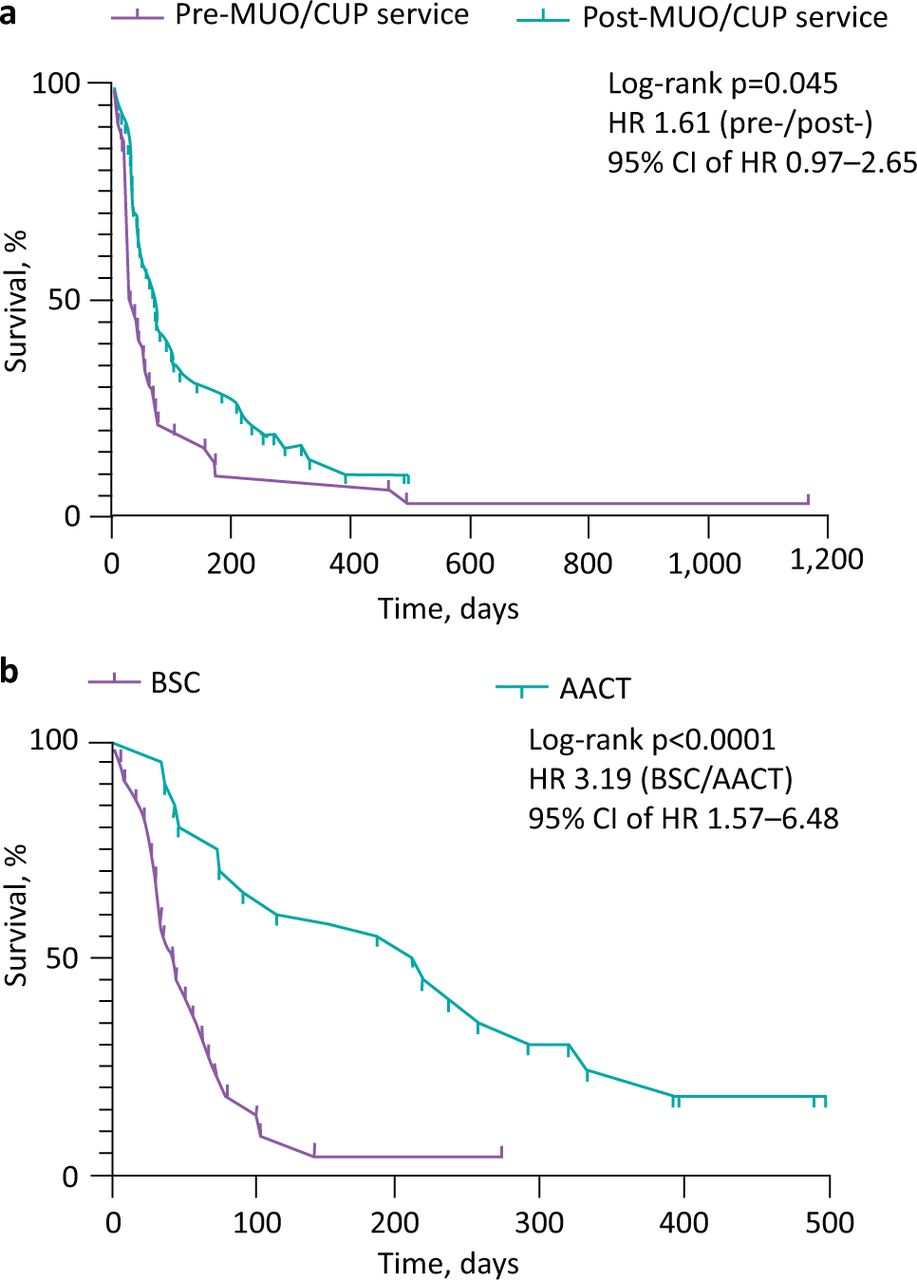
Kaplan–Meier curves comparing survival. a) Pre-malignancy of undefined primary origin (MUO)/carcinoma of unknown primary (CUP) service cohort versus post-MUO/CUP service cohort. b) Best supportive care versus active anti-cancer treatment in post-MUO/CUP service cohort. AACT = active anti-cancer treatment; BSC = best supportive care; CI = confidence interval; CUP = carcinoma of unknown primary; HR = hazard ratio; MUO = malignancy of undefined primary origin.
Service outcome data in prospective database
Out of 42 referrals to the MUO/CUP service, 25 patients were referred as inpatients and 17 as outpatients. Twenty-one of the 25 inpatients were referred within a week of suspected diagnosis, while 12 out of 17 outpatients were referred within 2 weeks of suspected diagnosis. Time from suspected diagnosis to referral was greater than 2 weeks for seven patients (Table 3).
Time interval from suspected diagnosis of malignancy of undefined primary origin/carcinoma of unknown primary to referral to service
All 42 patients were discussed in the MUO/CUP MDM, with 36 patients being discussed within 2 weeks from referral. Twenty-four of 25 inpatients were reviewed by AOS/CUP service within 24 hours of referral. For one inpatient who was an outlier in a peripheral hospital, remote advice was given. Thirteen of a total of 17 outpatients were reviewed within 2 weeks (Table 4). Out of the total patient cohort, 20 patients were deemed suitable for some form of active treatment. For those patients receiving anti-cancer treatment, 17 patients were treated within 31 days from DTT and 18 patients were treated within 62 days of initial referral (Table 4). Thirty-five patients of 42 had PCT review, the remaining seven patients either declined or did not require PCT input (Table 2).
North West Cancer Centre’s performance for MUO/CUP patients matched against national cancer waiting targets and recommended NICE targets for MUO/CUP patients
Patient satisfaction survey outcome in prospective cohort
MUO/CUP patient satisfaction survey was launched a few months after the service was embedded. Feedback questionnaires were constructed and distributed to patients at either a new patient appointment or at a subsequent hospital visit. The questionnaires were anonymised, and patients were requested to post them in pre-paid envelopes. Before the questionnaires went live, they were adapted several times based on our own learning from the complex needs of the service. Thus, we managed to send out only eight forms in the latter part of study. Compiled data from six responders has been largely positive (Table 5).
Malignancy of undefined primary origin/carcinoma of unknown primary patient feedback survey outcome; total n=6
As the majority of new referrals came from a non-oncology medical specialty in secondary care, informal feedback from physicians was sought. One hospital respiratory consultant commented, ‘Referring to CUP-MDM has halted unnecessary investigations and further delay in patient pathway. This is a much better journey for these patients/carers.’
Discussion
Despite advances in imaging, biomarkers and companion diagnostics in MUO/CUP patients, putative primary sites of tumour origin often remain elusive.2,6 Consequently, patients undergo multiple investigations and MDM discussions; face delayed diagnosis and oncology/palliative team input. A combination of these factors are major barriers in outlining an early and definite management plan, which can either be prompt and personalised therapeutic strategies in fit patients; or early cessation of inappropriate investigations and institution of BSC in unfit patients. In the absence of a streamlined approach, MUO/CUP patients are subject to poor patient/carer experience as well as poor survival outcomes.
To address this unmet need, a dedicated MUO/CUP service was set up in NWCC. Joined-up working both at the oncology outpatient clinic as well as the inpatient service, with medical oncology, clinical oncology and PCT consultants, has allowed patients to be seen during one hospital episode. Single e-referral capturing both AOS and MUO/CUP patients simultaneously has ensured simplicity and easy acceptance by the wider trust.
A clinico-pathological database was constructed as quality improvement tool to enhance service/patient outcomes. In the retrospective database spanning over a comparable 17-month period, total number of patients were low. We suspect some eligible patients were inadvertently excluded due to inadequate coding. With introduction of AOS to the trust and rolling education sessions, engagement with the MUO/CUP service improved over time. This is reflected in more robust numbers in the prospective database. We observed not only a steady increase in the number of referrals over time (Fig 2), but also a shorter time interval from suspected diagnosis to referral to the service (data not shown).

Number of referrals to malignancy of undefined primary origin/carcinoma of unknown primary service over time.
We observed that time from DTT to definite management is wide ranging (0–99 days); this is partly because once patients were handed over to TSS groups, the pathway became complex and was impacted by multifactorial issues independent of the MUO/CUP team. A strong relationship between multidisciplinary site-specific teams working closely with the MUO/CUP team will hopefully be able to achieve better outcomes from joined-up care.
Overall, compared with the retrospective database, we found higher percentages of patients not only identified to have site-specific cancers, but also receiving active treatment with a wider range of anti-cancer therapies. A limitation of this study is that the retrospective database was dependent on appropriate coding to capture MUO/CUP patients and preceded a well-established AOS service; whereas the prospective database was dependent solely upon AOS-referrals. Thus, in the prospective database, oncology input was 100%, data was more comprehensive (eg more recordings of PS) and an active AOS ensured patients had early interventions; this naturally would impact on cancer outcomes. Additionally, both cohorts of MUO/CUP were quite heterogeneous, consistent with the nature of this diagnosis, and direct head-to-head comparison is thus challenging. With those limitations in mind, we see statistically significant improvement in survival in the prospective cohort. We note that only one additional consultant oncologist was recruited in the 3 months between completion date of retrospective study and start date of prospective study, thus difference in oncology consultant staffing alone was less likely to have a profound impact. Interestingly, a comprehensive palliative team-led MUO/CUP service, despite demonstrating value in terms of early PCT input (which is a key component of care in this group), failed to show any survival advantage, albeit having limitations of modest sample size and single-site study.10 In our study, variation in clinical outcomes between the two groups undoubtedly is reflective of a new AOS (with a dedicated AOS CNS) providing early specialist access embedding comprehensively within existing infrastructure of the trust over time. Because CUP service went live more or less in parallel with overarching AOS, it is difficult to tease out the specific survival-related benefit from CUP team intervention in isolation. We note that overall prognosis remained grave in the majority; active treatment was in the form of palliative radiotherapy for several patients. This reinforces the need for timely oncology as well as PCT involvement in order to achieve dual aims: be prompt and selective in choosing appropriate patients for active treatment, while focusing on quality of life and patient journey in the wider group. Contemporary studies have published dismal survival rates in CUP patients, although our data (Fig 1b) and published reports demonstrate that favourable sub-groups can do significantly better.4,11,12
The majority in the retrospective group and 100% of patients in the prospective group were offered palliative care (16.67% did not need it or refused in the prospective group). Yet, we note that hospice placements in both groups were overall quite low as compared with reports published by English peers; this may be reflective of some uniqueness in cultural differences and social values specific to Northern Ireland that can influence patient choice and carer support.10 As compared with the retrospective group, in the prospective group, hospice placements were lower, more patients died in hospital and fewer patients died at home. The results are in contrast to reports published by other groups using a similar analytic model, where hospital deaths were fewer and home deaths more with an established MUO/CUP service.10,13 Our results may well be indicative of local variations in availability/accessibility to hospice placements and social packages during the study periods. Additionally, in the prospective group, more patients underwent comprehensive work-up including invasive investigations and active anti-cancer treatment, which may have inadvertently resulted in more hospital deaths. It is difficult to formulate a working hypotheses regarding negative impact of service intervention on home versus hospital deaths, as the numbers are small in both groups. We are also conscious that dying at home may not always be used as a surrogate marker of quality or experience of end-of-life care; as such, there was no significant difference between the datasets.14,15
Early identification, accelerated decision-making and timely intervention facilitated by AOS/CUP service has been associated with statistically favourable LOS (our data and others).13 However, it is important to acknowledge that in our prospective study, wide variations existed for inpatients in terms of waiting times from diagnosis to MUO/CUP service referral. This was especially prominent for inpatients in peripheral hospitals, and in the early part of the study where engagement with the service was gradually evolving. In the treated patients, prolonged postoperative recovery after surgical intervention, or administration of inpatient systemic therapy/radiotherapy, also impacted on overall LOS. Additionally, the study group was a modest size at best. Notwithstanding these limitations, as compared with median LOS of 15 days in a descriptive study done on a historical cohort of 7,599 MUO/CUP patients, in our prospective group, median LOS of 7.75 days was considerably lower.12 As such, we feel that defining performance indicators for MUO/CUP patients should go beyond conventional markers such as LOS, readmission rates, survival outcomes and place of death. Additional parameters such as quantifying MDM discussions, invasive/non-invasive investigations, as well as timeframe from diagnosis to referral, from referral to DTT and from DTT to definitive management in the pathway perhaps can be explored. The challenge of capturing patient/carer experience in a group with limited prognosis, who are often overwhelmed by the uncertainty of the cancer diagnosis, is also considerable. Our overall patient feedback, although positive, is from a limited number of patients and an extended capture of patient/carer experience is required.
Our data on proportion of MUO/CUP AOS referrals, patient-profile and tumour profile is comparable with published reports.10,11,13 Our study is unique in that it projects conception of the first oncology-led MUO/CUP service as an offshoot of a newly setup AOS in a single cancer centre in Northern Ireland and its positive impact on overall patient journey and outcomes. Apart from NICE published recommendations on CUP-specific waiting times, there are no robust MUO/CUP-specific national guidelines on performance indicators.1 We have extrapolated national gold standard of cancer waiting times (CWT) as a benchmark and retrospectively measured compliance of the new service against this.9 Statistically powered future studies are needed with robust numbers to assess the impact of active treatment versus BSC on survival, LOS and quality of life. Moreover, an economic model is needed to interrogate financial benefits of a comprehensive oncology-driven CUP service in an overall poor prognostic group of patients. Our aim is to quantify the advantages reaped in terms of avoiding duplication in MDM discussions, reducing unnecessary investigations/LOS/readmissions etc versus impact on hospital resources in terms of funding clinical sessions for team members, diversity in active anti-cancer treatment for treatable sub-group, as well as much needed recruitment to clinical trials/translational studies.
For sustainability of a consultant-led MUO/CUP service, job planning needs to reflect time commitment and that deputies for all core members are identified as per NICE recommendations. Given the complexity and poor prognostic implications for these patients, the entire MUO/CUP team should work together to ensure that investigations are focused, personalised for each patient and kept to a minimum. Time from referral to diagnosis and assessment should be as short as possible; and input from a specialist oncologist and PCT should be accessed from the outset through the MUO/CUP MDM. Hospital clinic follow-up should only be carried out if deemed appropriate, with early handover to general practitioner, district nursing and community PCT accessed closer to the patient’s home, where appropriate. The goal of maximising lifespan as well as quality of life for these patients and their carers should be the focus of care.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj:
S1 – Schema outlining the MUO/CUP referral pathway.
S2 – Clinical pathway for initial management and work-up of MUO/CUP patients before referral to oncology specialty.
S3 – Acute oncology service and MUO/CUP e-referral form.
S4 – Patient demographics in both pre- and post-MUO/CUP service cohorts.
S5 – World Health Organization performance status classification (NICE, 2007).16
Acknowledgements
CUP service: Dr Michael Reilly (consultant radiologist), Dr Ciara Lyons (consultant clinical oncologist), Dr Damien McMullan (consultant in palliative medicine) and Dr Michael McKenna (consultant histopathologist).
North West Cancer Centre: Dr David Stewart (consultant clinical oncologist and cancer lead), Ms Bridget Tourish (cancer service manager) and Dr Margaret McCloskey (respiratory consultant physician).
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.