
Key Points
The diagnosis of a seizure can be difficult; the gold-standard is rapid assessment by a specialist interested in epilepsy in a ‘first-seizure’ clinic
Rapid brain magnetic resonance imaging is the imaging of choice
Standard UK practice is to start antiepileptic drugs only after a second seizure when a diagnosis of epilepsy is confirmed
For a first isolated seizure, DVLA regulations have recently changed from a 12-month to six-month off-driving stipulated period, if investigations reveal no propensity for further seizures
An epileptic seizure is a dramatic life event. When attributing the diagnostic label of ‘seizure’ or ‘epilepsy’ physicians should bear in mind that, although such a diagnosis directs investigations, the greatest impact can be to place social restrictions on the individual. An erroneous diagnosis leads to inappropriate investigations and treatment, and can result in loss of driving privileges and employment. It is increasingly recognised that misdiagnosis is common, and what is considered best practice in assessment, investigation, prognosis and treatment of a first seizure continues to develop.
Assessment
National guidelines recommend that assessment of a potential seizure is undertaken within two weeks in the setting of a first seizure clinic by a specialist in epilepsy.1,2 Acute care settings should have care pathways for safe discharge. Such patients should have fully recovered, be alert and orientated, apyrexial and safe to discharge with a carer.
Most attacks of transient loss of consciousness with rapid recovery presenting to primary care will represent faints (named here ‘vasovagal syncope’ (VVS)). Similar to the experience of other clinics,3 about half the referrals to the University Hospital Birmingham First Seizure Clinic are typically not epileptic. The most common alternate diagnosis is VVS. Thus, understanding the clinical features of VVS, cardiac syncope and seizure remains essential to allow for accurate diagnosis.
Diagnosis and misdiagnosis
The misdiagnosis of a VVS as a seizure most commonly occurs following an isolated event that may be only partially witnessed, in which the assessor places too much diagnostic weight upon a feature erroneously thought to indicate a seizure. The physician should form their own opinion and not assume a colleague's diagnosis is correct, for this may well not be the case,4 with a clear mind's eye picture of before, during and after the collapse. The ubiquitous ownership of mobile phones within the UK now means a witness is rarely uncontactable. Table 1 highlights some of the features that can be useful in differentiating a seizure, VVS and cardiac syncope.5 Certain features such as incontinence are a poor differentiating factor, while the presence of postictal confusion is most differentiating. It is not universally appreciated that convulsive-like movements (jerks) are commonly seen in syncope – as shown by Lempert's video of German medical students self-inducing VVS.6 The mechanism of the jerky movements is cerebral hypoxia, originating from the brainstem rather than an epileptic phenomenon. Syncope of cardiac origin has typically no or very brief prodromes, with loss of consciousness and fairly rapid recovery. Specialist cardiological assessment with echocardiography should be considered with a background of cardiac disease, family history of sudden death or an abnormal electrocardiogram (ECG).
Features helpful and unhelpful in differentiating seizure from syncope.5
Unusual causes of collapse
Causes of collapse which are more rare and from which there is rapid recovery include:
Psychogenic attacks: these are not a realistic differential of a single isolated event, but recurrent and frequent attacks may be hard to differentiate from epilepsy and require specialist assessment.
Cataplexy: in this condition attacks of complete loss of muscle tone are provoked by sudden emotions. Consciousness is retained throughout and the patient reports feeling paralysed and unable to breathe. Symptoms of narcolepsy are invariably present.
Transient ischaemic attack: this rarely causes loss of consciousness, but a posterior circulation event with brainstem ischaemia can lead to impairment of consciousness. In such cases, other symptoms of brainstem dysfunction such as diplopia, hemiparesis or ataxia are commonly reported.
Hypoglycaemia: this metabolic imbalance causes attacks of altered mentation, confusion and/or seizures, usually in the early mornings or after prolonged fasts. Recurrent attacks would be expected. All acute care settings will undertake a random blood sugar in a patient with recent loss of or reduced consciousness.
Determining cause
All patients with an episode of transient loss of consciousness should have an ECG. Patients with VVS should not have neurological investigations. If it is possible that a seizure has occurred, it is worth considering whether this was provoked, for example by medications such as selective serotonin reuptake inhibitors or by biochemical abnormalities. Provoked seizures have a low risk of recurrence once the provoking factor is removed and carry different regulations for driving. Drugs know to provoke seizures are listed in Table 2.
Drugs that may provoke seizures.
Investigations
Serum prolactin
A serum prolactin test is not recommended in the routine assessment of a possible seizure.1 There are several limitations to using postictal serum prolactin elevation:
it cannot be used to differentiate simple partial seizures or absence seizures from non-epileptic seizures
prolactin levels may increase following VVS and elevations have been observed following tilt table testing
complex partial seizures that do not arise from the temporal lobe do not lead to prolactin elevation
a postictal prolactin rise may not be shown by 10–20% of patients with tonic-clonic seizures
ambiguous test results, such as a twofold elevation, are difficult to interpret. Prolactin level rises predictably only after a single seizure
patients who have more than two seizures in 12 hours have progressively smaller elevations, presumably because stored prolactin from the pituitary lactotrophs is exhausted.7
Magnetic resonance imaging and computed tomography
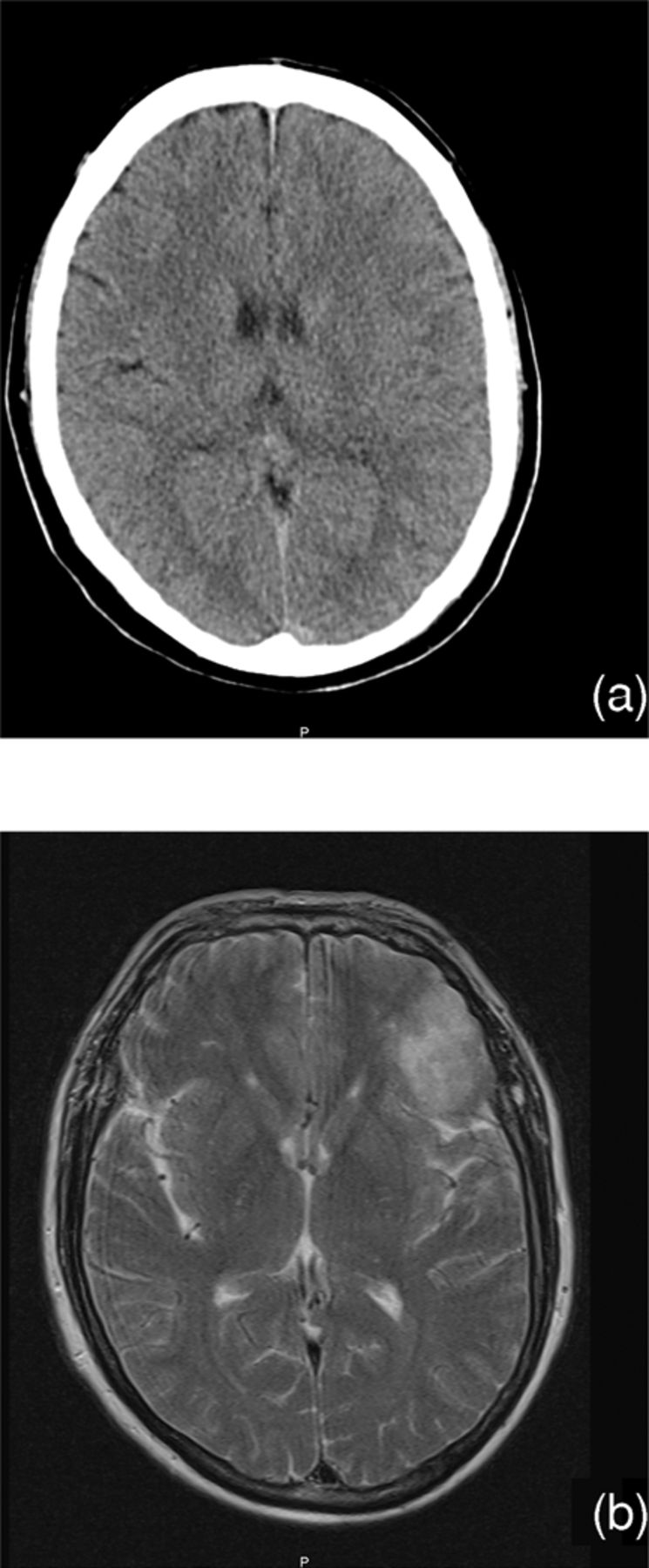
The gold standard of cerebral imaging is brain magnetic resonance imaging (MRI), recommended to be performed within four weeks of request.1 MRI is more sensitive than computed tomography (CT),2 as illustrated in Fig 1. However, CT scanning is the imaging to undertake in the acute setting because of other advantages: it is readily accessible, rapid and more sensitive for detecting acute cerebrovascular events.

Different resolution of in vivo head scan imaging techniques: (a) computed tomography, (b) magnetic resonance imaging.
In determining the cause of a seizure and epilepsy, specialist high-field MRI imaging with specific protocol for epilepsy interpreted by an ‘expert’ neuroradiologist is far more sensitive in detecting the subtle abnormalities than standard MRI protocols interpreted by ‘non-experts’. If undertaken at an early stage, such imaging can detect potential surgical candidates should a drug-refractory epilepsy develop.8
Electroencephalography
An electroencephalogram (EEG) should rarely be ordered to answer the question ‘What was this attack?’. The clinical assessment must try to answer this question. It is important to remember that about 1% of the healthy population will have an EEG with epileptiform abnormalities9 and a higher frequency is found in elderly or learning disability populations. Inappropriate use of EEG in collapses of non-epileptic origin can lead to misdiagnosis, with errors in assessment compounded by overinterpretation of ‘soft’ EEG abnormalities. The EEG has a useful role in the classification of epilepsy and a more limited utility in determining epilepsy risk in adults.10 The recent change in Driver and Vehicle Licensing Authority (DVLA) regulations incorporating EEG findings in the length of time driving privileges are removed may lead to an increased usage of EEG.
Treatment
The decision to start an antiepileptic drug (AED) is not taken lightly, considering the potential hazards of therapy. Moreover, in most cases treatment often continues for years. It is recommended that treatment is started by a specialist in epilepsy,1,2 and important that:
the diagnosis of epilepsy is secure
there should be a real risk of seizure recurrence
the patient be counselled as to the benefits and potential risks of therapy and feel involved in the decision-making process.
Antiepileptic drug therapy after a single seizure
Common practice within the UK is to start therapy after two spontaneous seizures as the risk of a further seizure is high. There is extensive evidence in animals to suggest seizures can themselves be pro-epileptogenic. This has influenced the practice, particularly within the USA, of starting treatment after a single seizure. However, there is no evidence that AEDs after a traumatic brain injury can prevent the development of epilepsy.11 Additionally, AED therapy after a single or infrequent seizures does not affect long-term development of epilepsy.10–14
If seizures are related to provoking factors such as metabolic disturbance or drugs, the provoking factor should be removed or treated and AEDs are not indicated. Similarly, alcohol withdrawal seizures should not be treated with long-term AEDs, but management should address the alcohol misuse and the risks carried by alcohol withdrawal.
Prospective studies reveal that the two-year risk of recurrence following a single unprovoked tonic-clonic seizure is around 30–40%.12–15 However, treatment may be started after a single seizure when the benefits are perceived to outweigh the hazards of treatment. Scenarios in which AED therapy can be started after only one tonic-clonic seizure might include:
A 42-year-old male who presents a single tonic-clonic convulsion. History reveals stereotypical attacks of déjà vu and rising abdominal sensations over the last four years. He recalls a similar sensation prior to his major convulsion. This presentation suggests epilepsy of probable temporal lobe origin – the tonic-clonic seizure was the event that revealed the diagnosis of epilepsy. The déjà vu sensations are partial seizures (‘epileptic aura’ if preceding a full-blown seizure).
Neuroimaging reveals a relevant abnormality.
EEG demonstrates unequivocal epileptiform abnormalities.
The individual has a neurological deficit.
The individual or carer considers the risk of a further seizure unacceptable. A common scenario is fear of a further loss of driving privileges.
The Driver and Vehicle Licensing Authority
There has been a recent change to the DVLA regulations for an isolated seizure.16 A six-month off-driving period has been stipulated, starting from the date of the seizure, if the licence holder has undergone assessment by an appropriate specialist and no relevant abnormality has been identified on investigation (eg EEG and brain scan, where indicated). The former 12-month removal still applies if there is a potential liability to epileptic seizures. Following a single seizure, Group 2 licence holders (HGV drivers) have a five-year driving restriction if tests fail to support an underlying predisposition for epileptic seizures. However, if a second seizure occurs, a 12-month driving ban applies to Group 1 licence holders and a 10-year ban to Group 2 licence holders.
Safety and employment
A seizure is career-ending in a few vocations such as airline pilots or HGV drivers. Given the gravity of the diagnosis we commonly refer for a second opinion if we or the patient have doubts. It is important to advise the patient who has suffered a potential seizure that they should inform their employer. For most jobs it will be reasonable to continue. Common sense advice would apply in situations such as working:
at heights or underground
near open water
with hot ovens or open fires
with high voltage/open circuit electricity
operating heavy machinery or moving vehicles with chemicals.
All patients should be advised against swimming in deep water and having baths alone.
Conclusions
As physicians we strive to do no harm – in assessing a possible seizure, this means getting the diagnosis correct. Accurate diagnosis can prevent loss of employment and driving restrictions and directs selection for appropriate tests. Through the next decade assessment of a potential seizure should increasingly take place in specialised ‘first seizure’ clinics. Investigations will routinely involve rapid (epilepsy protocol) MRI imaging. However it remains not possible reliably to predict which individual will go on to develop epilepsy after a first seizure. Moreover, we await a drug that will go beyond a short-term action of raising the seizure threshold and have a long-lasting effect on epileptogenesis so as to reduce the risk of epilepsy.
- © 2010 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.