
ABSTRACT
Acute pancreatitis (AP) is a medical emergency associated with significant morbidity and mortality. Hypertriglyceridaemia is a well-established but often neglected cause of AP, associated with delayed diagnosis and worse outcome than other more common causes of AP. Although oestrogen-induced hypertriglyceridaemia is known to be a rare cause of AP in females, it is much less well-recognised in biological males. We report the case of a 52-year-old transgender woman receiving high-dose oral oestrogen therapy who was admitted with abdominal pain and found to have AP caused by severe hypertriglyceridaemia. We describe the features underlying the management of AP caused by hypertriglyceridaemia and review the link between oral oestrogen, hypertriglyceridaemia and AP.
Given the growth in transgender medicine leading to increasing use of therapeutic high-dose oestrogens in biological males for gender reassignment, it is important that clinicians are alert to the phenomenon of oestrogen-induced-hypertriglyceridaemia and its associated risk of AP.
Case presentation
A 52-year-old transgender woman was admitted as an emergency with severe epigastric pain of acute onset. There was no prior history of pancreatitis nor hyperlipidaemia. She had a prior diagnosis of gender dysphoria and had undergone gender reassignment 5 years previously. This treatment included bilateral orchidectomy and feminising genital reconstructive surgery with subsequent high-dose oral oestrogen therapy. At the time of her admission she was taking oral oestradiol 8 mg daily. There was no history of diabetes and she was not taking any lipid-lowering medication and did not consume alcohol.
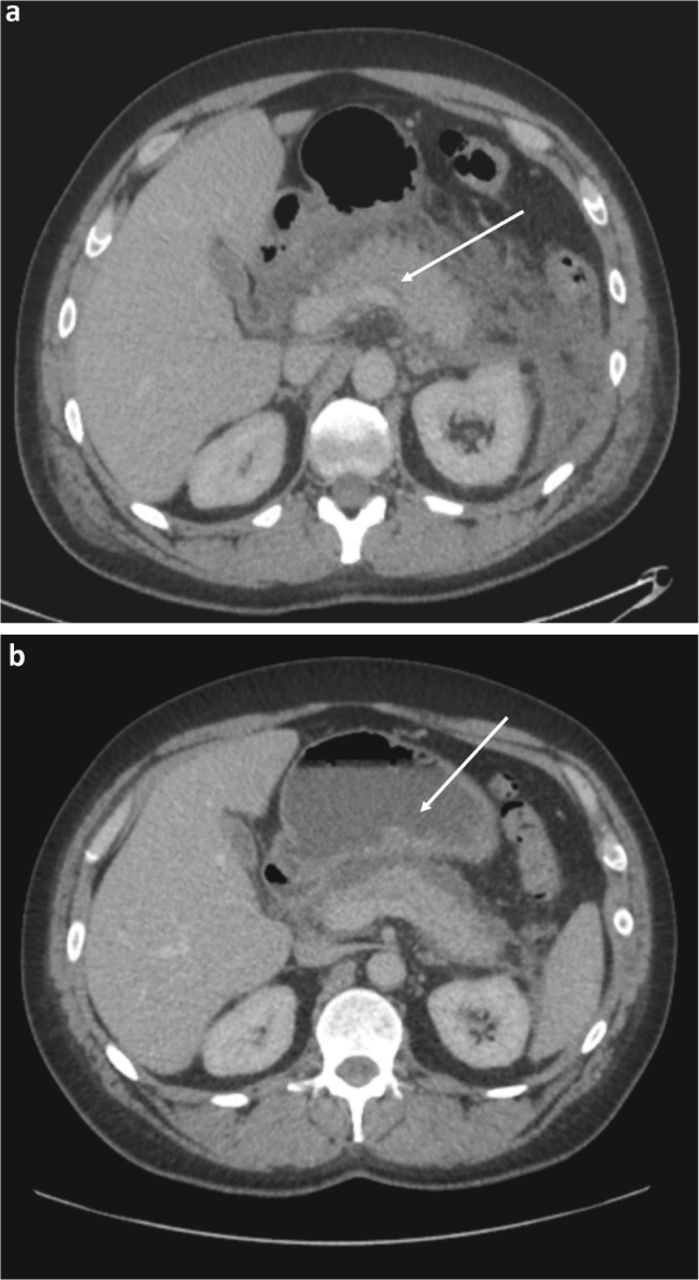
On examination, she appeared acutely unwell with epigastric tenderness and guarding. Results of laboratory investigations (Table 1) demonstrated lipaemic samples with severe hypertriglyceridaemia. A raised serum amylase result was suggestive of acute pancreatitis and this diagnosis was confirmed following abdominal imaging with computed tomography (CT; Fig 1).
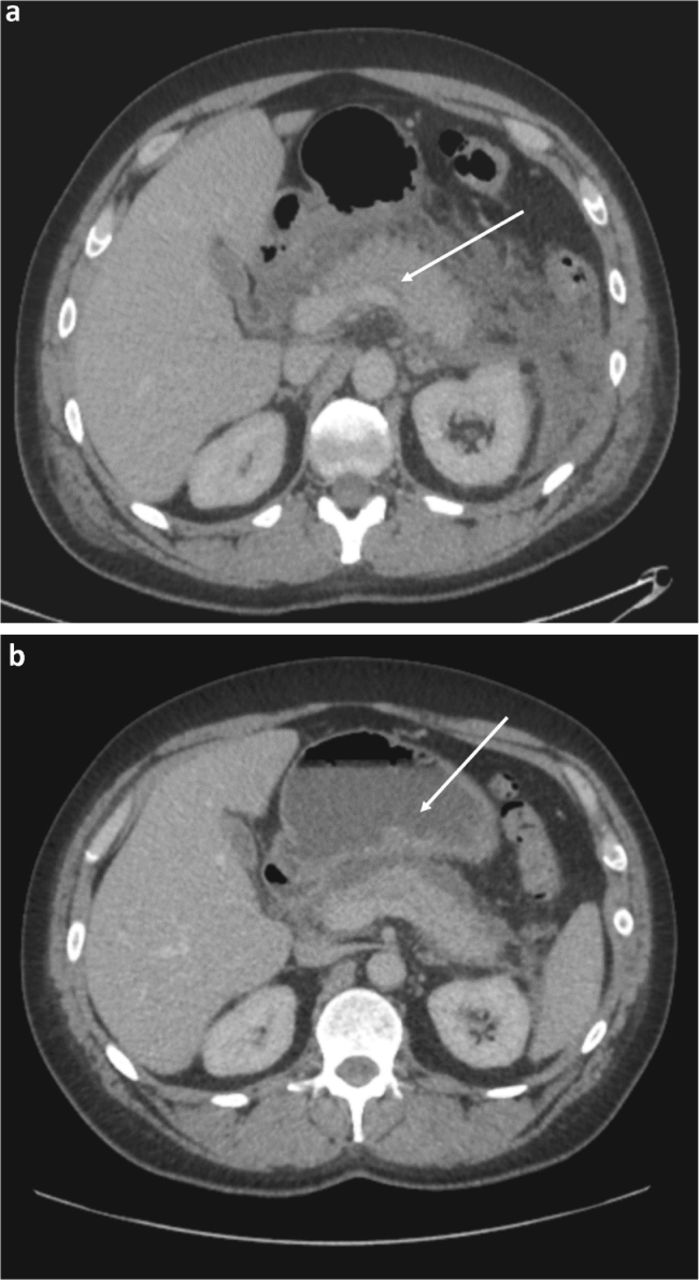
Axial computed tomography (CT) of the abdomen a) CT at presentation. The pancreas (white arrow) showed features indicative of acute pancreatitis with swelling, oedema, indistinct margins and surrounding fat stranding. The liver showed a diffuse increase in echogenicity in keeping with fatty change. No biliary duct dilatation was seen and the gall bladder did not contain stones. b) A repeat CT 14 days post-presentation showed resolving pancreatic inflammation but with the development of a pancreatic pseudocyst measuring 4 cm × 3 cm × 1.8 cm (white arrow).
Results of laboratory measurements at the time of admission
A diagnosis of acute pancreatitis precipitated by severe hypertriglyceridaemia was made. Given concern regarding the effect of high-dose oral oestrogen on triglyceride levels, this medication was discontinued immediately. During the first 24 hours, a variable rate intravenous insulin infusion administered at a dose according to capillary blood glucose was commenced alongside a 10% glucose infusion, with the specific aim of lowering serum triglyceride levels and maintaining blood glucose within a target range of 4–10 mmol/L.
The patient's clinical condition improved steadily over a 14-day period. Oral diet was re-introduced after 48 hours with a recommendation to follow a low-fat diet. Oral oestradiol medication was not re-introduced due to concerns over the risk of recurrent hypertriglyceridaemia. Fig 2 shows the serial change in serum triglyceride concentration during the hospital admission following acute management, and in the period following discharge from hospital.
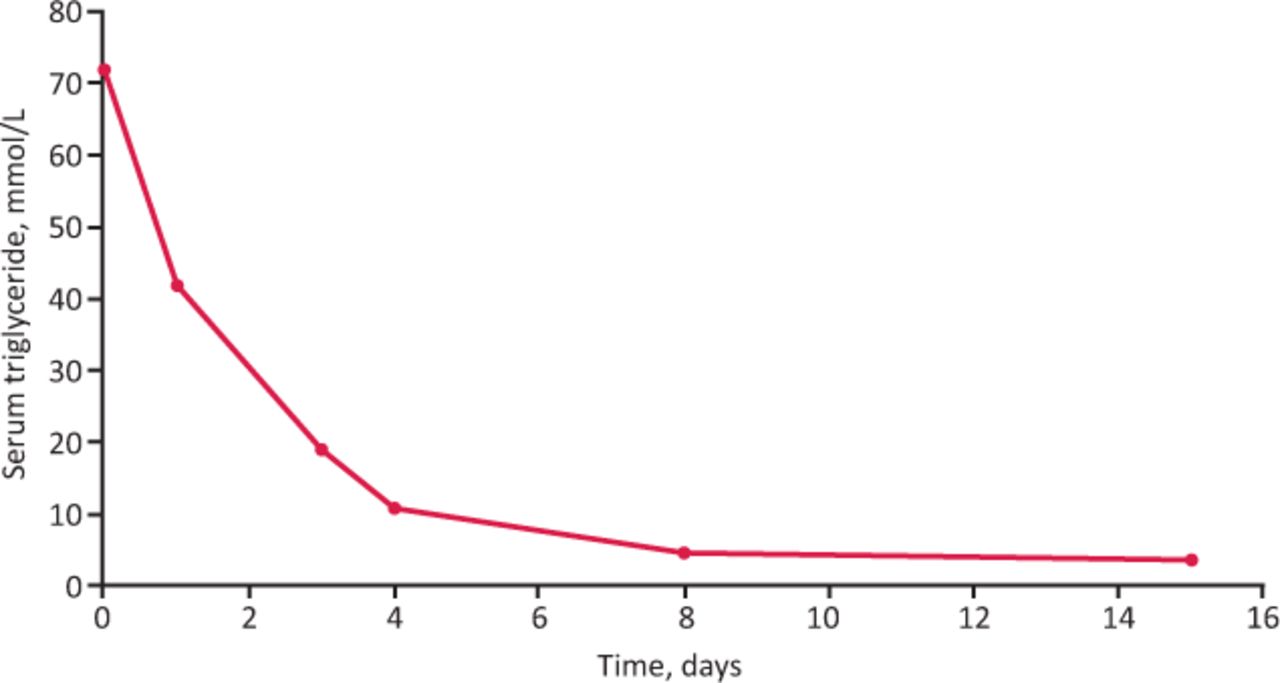
Serial change in serum triglyceride concentration over time following acute management.
The patient was subsequently reviewed in a lipid clinic. Examination was unremarkable with no cutaneous stigmata of hyperlipidaemia. A repeat fasting lipid profile showed mildly raised serum triglyceride of 6.6 mmol/L with total cholesterol of 5.9 mmol/L. Genetic testing was negative for lipoprotein lipase deficiency, ruling out the possibility of familial chylomicronaemia syndrome (FCS). No other secondary causes of hypertriglyceridaemia were apparent, with no dysglycaemia, renal or thyroid disease. Fenofibrate 200 mg daily was commenced. A repeat fasting lipid profile 3 months after the introduction of fenofibrate showed a significant improvement with total cholesterol 3.6 mmol/L, triglyceride 3.6 mmol/L, high-density lipoprotein cholesterol 0.8 mmol/L and LDL cholesterol 1.2 mmol/L. This improvement was sustained with a follow-up test 6 months later. To date, the patient has not recommenced oestrogen therapy.
The clinical impression was that of a likely underlying tendency to mixed dyslipidaemia. This was exacerbated by high-dose oral oestradiol therapy, which led to severe hypertriglyceridemia, culminating in the episode of acute pancreatitis.
Discussion
Acute pancreatitis (AP) is a medical emergency associated with significant morbidity and mortality.1 Hypertriglyceridaemia is a well-established but often neglected cause of AP, being responsible for around 7% of cases and often associated with delayed diagnosis and worse outcome than other more common causes of AP.2
The underlying pathophysiological mechanisms of hypertriglyceridaemia-induced AP are still poorly understood but are likely to involve accumulation of triglyceride-rich-lipoproteins in the pancreatic capillary bed; these are then hydrolysed by pancreatic enzymes to free fatty acids which exert a direct toxic effect on pancreatic tissue, leading to AP.2
Although there are no firmly established treatment guidelines specifically addressing the problem of hypertriglyceridaemia in AP, a number of treatment modalities to suppress circulating triglyceride concentration have been used successfully in the acute setting.2,3 These include the use of intravenous insulin infusion, as in the present case, to acutely lower triglyceride-rich lipoproteins through activation of lipoprotein lipase activity.
In susceptible individuals with a pre-existing tendency to hypertriglyceridaemia, exogenous oestrogen is known to exert direct effects on the metabolism of triglyceride-rich lipoproteins with a clear dose response relationship between oestrogen and hepatic very-low-density lipoprotein (VLDL) production, capable of triggering clinically significant hypertriglyceridaemia.4 This effect appears to occur with oral oestrogen administration of both conjugated and natural oestrogen preparations but not with transdermal administration, an observation that is indicative of a first pass metabolic effect, mediated through supraphysiological oestrogen delivery via the portal circulation to hepatocytes and likely to be occurring independently of lipoprotein lipase activity.4 Oestrogen-induced hypertriglyceridaemia causing AP was first reported many years ago in females taking the combined oral contraceptive pill but more recently has also been reported in the field of assisted reproduction.5,6 The occurrence of oestrogen-induced hypertriglyceridaemia causing AP is much less recognised in males but has historically been reported in males receiving high-dose oestrogen therapy for advanced prostate cancer.7
The use of therapeutic high-dose oestrogens in biological males for gender reassignment purposes has increased considerably in recent years. It is estimated from recent surveys that approximately 0.6% of the USA population identifies as transgender and specialist transgender clinical services have expanded considerably in the UK and in Western Europe within the last decade.8,9 To date, the occurrence of oestrogen-induced hypertriglyceridaemia causing AP in male to female trans patients is not a well-recognised phenomenon.10 Furthermore, in a recent comprehensive clinical practice review of transgender people, there is no mention of the possibility of oestrogen-induced hypertriglyceridaemia.8
The development of oestrogen-induced hypertriglyceridaemia severe enough to provoke AP appears to be unpredictable but is likely to be associated with a tendency to pre-existing hypertriglyceridaemia.4,5 It appears to be more likely to occur with the use of high-dose oral (as opposed to transdermal) oestrogens and is less likely to occur with conventional doses of oestrogens used for contraception and hormone replacement therapy (HRT) in women.
We suggest that clinicians working in the field of transgender medicine should be alert to the possibility of oestrogen-induced hypertriglyceridaemia. Furthermore, we would recommend that serum triglyceride concentrations are monitored in trans patients commenced on high-dose oestrogens, especially those who may have pre-existing risk factors for hypertriglyceridaemia. We would advocate that extreme caution should be exercised with consideration of transdermal rather than oral preparations in those with a history of significant pre-existing hypertriglyceridaemia.
- © Royal College of Physicians 2021. All rights reserved.








{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.