
Abstract
Multiple myeloma (MM) is a type of haematological bone marrow malignancy. Cancer Research UK reports that MM is the 18th most common cancer in the UK, accounting for 2% of all new cancer cases, yet, non-haematologists often lack familiarity with the pathology and initial investigations. This paper aims to demonstrate the diagnostic features, relevant investigations and basic management plan for the non-specialist.
Key points
Multiple myeloma (MM) can affect people of any age; 40% of new diagnoses are in people aged 75 years or over. Overall, MM patients have a 10-year prognosis of 30% survival, although this is improving as therapeutic advances continue to occur.
MM is caused by malignant plasma cells that secrete monoclonal paraprotein; subtypes of disease can be dictated by the predominant immunoglobulin (Ig; IgG is the most common) and light chain (kappa or lambda).
Diagnostic criteria for monoclonal gammopathy of undetermined significance (MGUS), smouldering myeloma and MM are determined by the percentage of plasma cells in the bone marrow, presence of end-organ disease (‘CRAB’), paraprotein levels (more or less than 30 g/L), kappa/lambda light chain ratio (>100), bone marrow plasma cell percentage and urinary M protein levels (>500 mg / 24 hours).
Skeletal surveys are rarely used, instead, whole-body cross-sectional imaging is preferred (such as computed tomography (CT), positron emission tomography – CT and magnetic resonance imaging).
Both primary care and secondary care have essential roles in supporting patients and their families with MM, including optimising analgesia, early treatment of infection and monitoring for haematological emergencies (such as cord compression).
What is multiple myeloma?
Multiple myeloma (MM) is a type of haematological bone marrow malignancy. MM arises from clonal proliferation of defective plasma cells and the harmful effects on multiple organ systems from deposition of monoclonal paraproteins. Cancer Research UK reports that MM is the 18th most common cancer in the UK, accounting for 2% of all new cancer cases.1 At least 40% of new diagnoses per year are in those aged 75 years or over.1 The current prognosis is 80% survival at 1 year, 50% at 5 years and 30% at 10 years.1 This is a significant improvement from the 1970s, when only 5% of patients survived for 10 years, reflecting improved diagnosis and treatments for the disease.1
Plasma cells are terminally differentiated B lymphocytes that secrete antibodies or immunoglobulin. B lymphocytes play an essential role in the humoral immune system and facilitate expression of antigen specific immunoglobulin in the response to exposure to invasive pathogens.2 Immunoglobulins are secreted by plasma cells in response to infection and are polyclonal. The normal repertoire of immunoglobulins is generated through gene recombination and class switching, something that makes B cells innately prone to genetic error as they differentiate into plasma cells. Defective plasma cells develop as a consequence of genetic changes, resulting in prolonged cell survival and enhanced replication. Chromosomal translocations are seen in 35%–50% of patients and usually involve the immunoglobulin heavy chain gene on chromosome 14. In other patients, gain of chromosomes are seen (termed hyper-diploidy) that similarly cause plasma cell transformation. These events, in additional to mutations of tumour suppressor and oncogenes leads to the over-production and secretion of monoclonal immunoglobulin, termed M protein or paraprotein, that can be detected by serum protein electrophoresis.
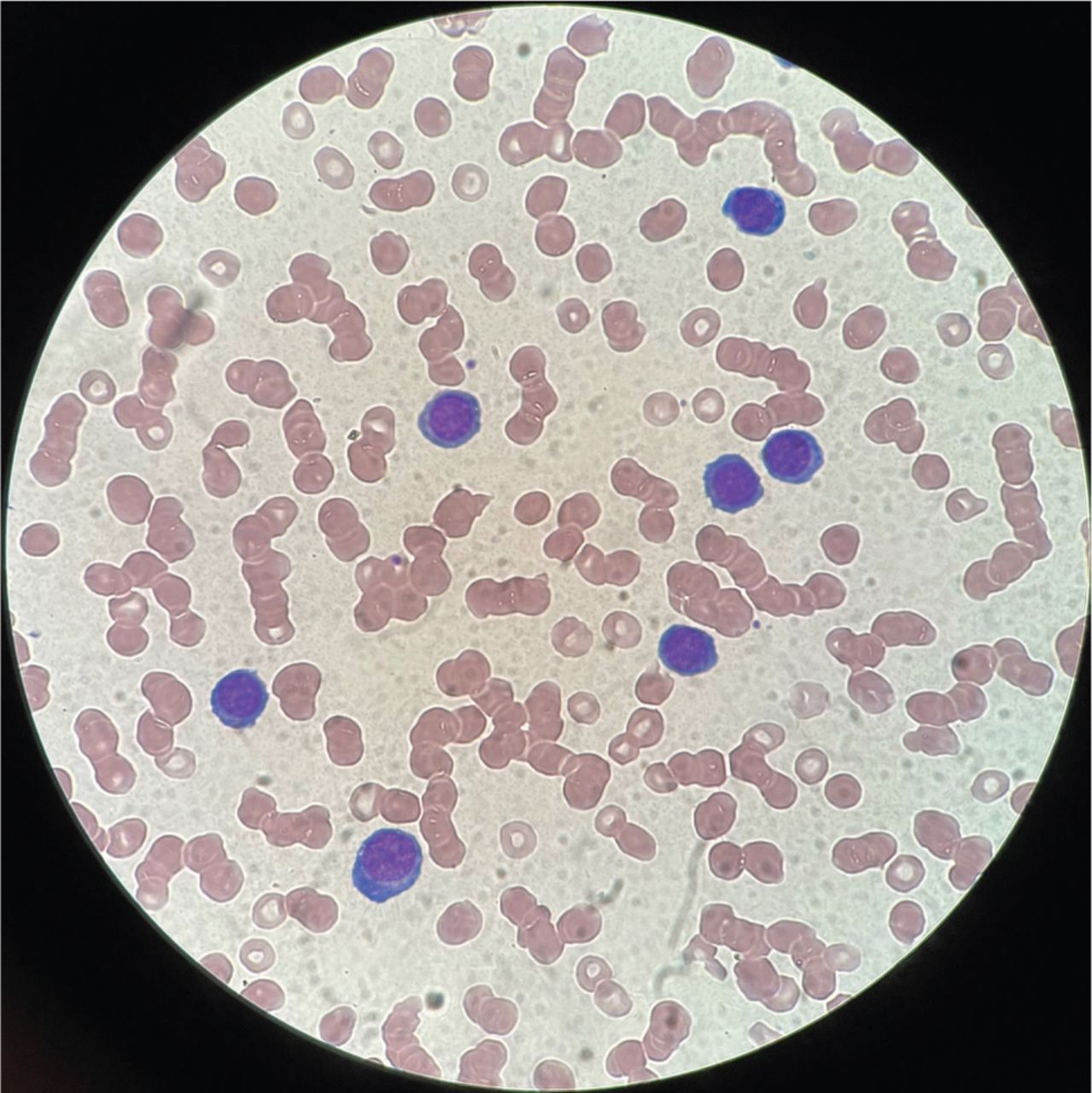
The immunoglobulin molecule consists of two heavy chains bound to two light chains by disulphide bonds (Fig 1). The five types of immunoglobulin (Ig) are IgG, IgA, IgM, IgE and IgD, with the light chain component restricted to either kappa or lambda. The most common type of paraprotein seen in myeloma is IgG kappa in which the myeloma cells produce two heavy IgG chains bound to two kappa light chains. IgA myeloma tends to carry a worse prognosis than IgG myeloma, while other Ig subtypes occur very rarely, as does ‘non-secretory myeloma’. In 20% of patients, the plasma cells secrete only the light chain portion of the immunoglobulin molecule, known as ‘light chain’ myeloma. These free light chains can be detected in the serum using the light chain assay, which has largely superseded urinary quantification of Bence Jones protein.
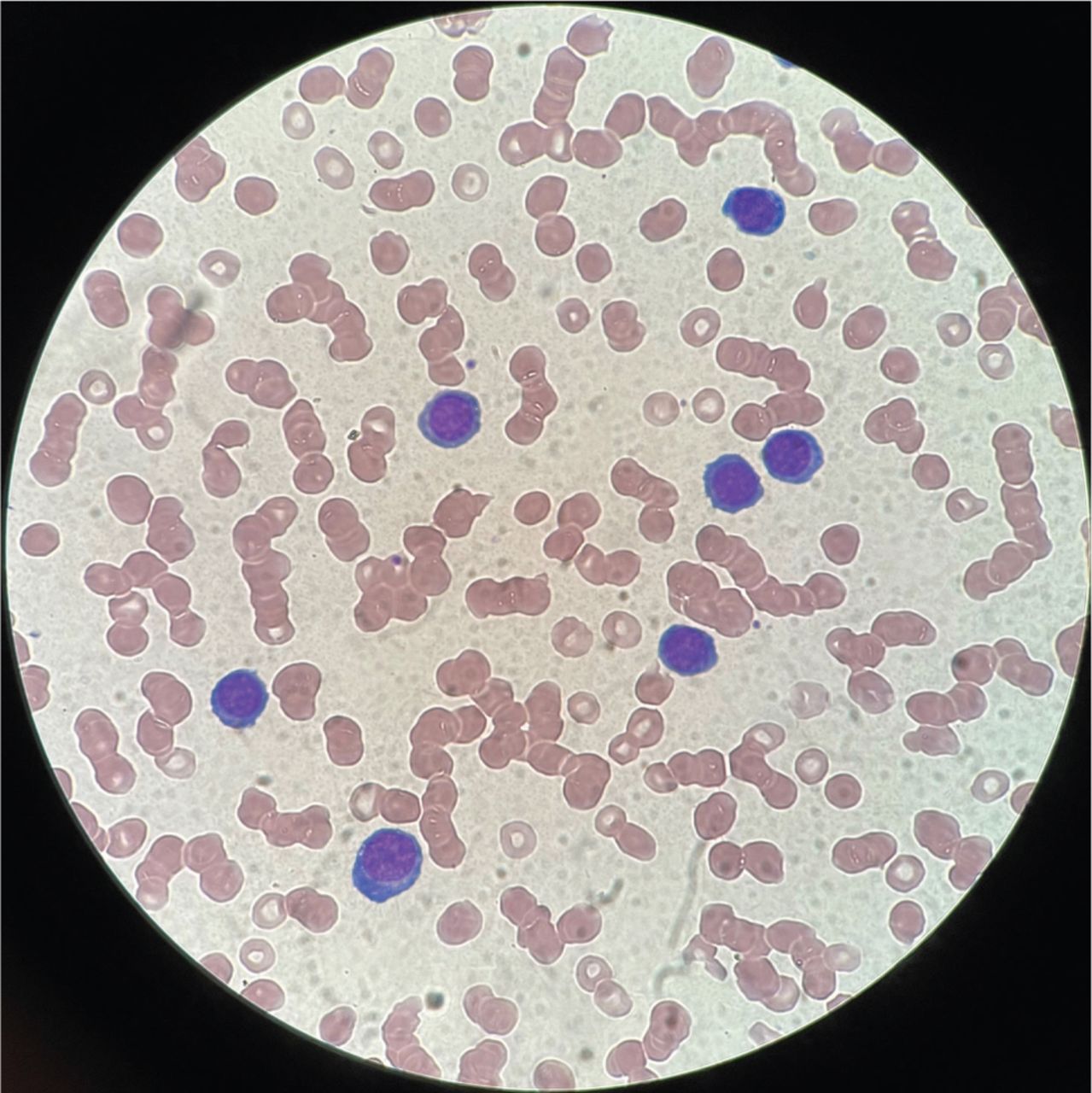
Blood film from patient with relapsed myeloma showing rouleaux formation of red cells and circulating plasma cells indicative of plasma cell leukaemia.
How does multiple myeloma present?
The manifestations of disease in multiple myeloma arise due to infiltration of the bone marrow with malignant plasma cells, as well as extraosseous deposits termed plasmacytomas, and to more widespread effects of the paraprotein on multiple organ systems. The presentation of end organ failure is often referred to by the mnemonic ‘CRAB’.3
C: Hypercalcaemia (serum calcium >2.75 mmol/L or >0.25 mmol/L higher than upper limit of normal) occurs when there is increased osteoclast activity causing osteolytic lesions. Signs include thirst, tiredness, confusion, arrhythmias or muscle spasms. Treatment may involve intravenous hydration and bisphosphonate therapy. Bisphosphonate therapy inhibits osteoclast activity and is preventative against pathological fractures and pain, but the effect on overall survival is undetermined.4 There is an increased risk of osteonecrosis of the jaw with bisphosphonate therapy and regular dental reviews are advised.
R: Renal impairment (serum creatinine >177 μmol/L or creatinine clearance <40 mL/min) results from both the precipitation of light chain casts in the distal tubule causing obstruction, and the direct toxic effect on proximal renal tubules.5 The non-specialist can facilitate recovery of renal dysfunction with hydration, and treatment of hypercalcaemia and hyperuricaemia. Poor recovery of renal dysfunction is associated with initial severe renal impairment and proteinuria.5
A: Anaemia (haemoglobin (Hb) <100 g/L or 20 g/L below lower limit of normal) and pancytopenia may occur secondary to heavy bone marrow infiltration by malignant plasma cells causing reduced production of red cells. Blood product support is often required and erythropoietin injections may be considered if there is also renal impairment.
B: Bone disease (>1 lytic bone lesion of >5 mm on X-ray, computed tomography (CT) or magnetic resonance imaging (MRI)). Pathological fractures may be localised to areas where bone marrow is most active in adults, namely the skull, spine, pelvis, rib cage and the long bones. A patient will often present with new bony pains or pathological fractures. In more severe cases, MM can present with spinal cord compression secondary to vertebral collapse or extraosseous plasmacytoma. Therefore, physicians should review for red flags of spinal cord compression and have a low threshold for urgent spinal imaging and neurosurgical review for potential decompressive options. Clinical oncology review should also be sought for consideration of radiotherapy. The National Institute for Health and Care Excellence (NICE) has published extensive guidance on red flags suggesting spinal cord or cauda equina compression including profound sensory or motor weakness; recent onset faecal incontinence (due to loss sensation of rectal fullness); recent onset urinary incontinence (loss of sensation of bladder fullness); and perianal anaesthesia.6
The risk of infection is also increased due to immune paresis and treatment, and MM patients should be reviewed urgently for signs of sepsis and may benefit from granulocyte colony stimulatory factor (GCSF) for neutropenia. Patients who already have a diagnosis of MM may be on prophylactic antibiotics, and anti-viral and anti-fungal agents, typically levofloxacin, aciclovir and fluconazole, respectively. Indeed, the recent TEAAM trial has demonstrated clear benefit for prophylactic levofloxacin in reducing early mortality in myeloma.7
Seven per cent of patients show signs of hyperviscosity at presentation with symptoms such as visual disturbance, cognitive impairment, and mucosal bleeding. If present, plasma viscosity or erythrocyte sedimentation rate (ESR) should be checked. Less than 5% of patients have clinical hepatomegaly or splenomegaly.8
Investigations and diagnostic criteria: what investigations should the non-specialist request?
Following the description of typical signs and symptoms, the non-specialist should be aware of which investigations to request for a suspected new diagnosis of MM. The following list is adapted from the recent summary of preliminary investigations recommended by the British Society of Haematology in the 2021 ‘Guidelines on the diagnosis, investigation and initial treatment of myeloma’.3
Screening tests: full blood count (anaemia/pancytopenia), urea and creatinine (renal dysfunction), calcium, and immunoglobulins (serum protein electrophoresis (to determine subtype, eg IgG myeloma) and serum free light chain assay (kappa and lambda)). Of note, the presence of a high paraprotein (>30 g/L), often with immune paresis, and/or skewed imbalance of the kappa/lambda ratio is highly suggestive of a diagnosis of myeloma.
Peripheral blood film may show rouleaux and occasionally circulating myeloma cells indicative of ‘plasma cell leukaemia’ (Fig 1). B2-microglobulin can also be requested to determine tumour burden. Virology screening (including HIV antigen, hepatitis serology, cytomegalovirus PCR and Epstein–Barr virus antibodies) should also be performed.
The traditional ‘skeletal survey’ has been superseded by cross-body imaging, such as CT, positron emission tomography – CT or MRI whole body. Focal imaging (such as MRI of the spine or pelvis) or plain films of long bones can be used to look at areas of concern in more detail.
Bone marrow aspirate and trephine biopsy should be performed to confirm diagnosis and risk stratify the patient based on the percentage of infiltration of plasma cells, flow cytometry to determine plasma cell phenotype, and fluorescence in situ hybridisation (FISH) analysis for chromosomal translocations and copy number abnormalities.
MM exists on a spectrum of disease and requires evidence of end-organ failure or other myeloma defining events, including a heavy bone marrow infiltrate of malignant plasma cells (>60%), a very deranged light chain ratio (>100) or more than one bone lesion of >5 mm on MRI. If there are no CRAB or myeloma-defining features, then the diagnosis is one of smouldering multiple myeloma (SMM) if the plasma cell infiltration is above 10%, or monoclonal gammopathy of undetermined significance (MGUS) if this is below 10%. MGUS can progress to myeloma at a rate of 1% of patients per year, but otherwise neither this nor SMM require treatment although they do require surveillance. Table 1 has been adapted from the British Society of Haematology guidelines on diagnostic criteria for myeloma.3
Diagnostic criteria for multiple myeloma, smouldering myeloma and monoclonal gammopathy of undetermined significance, adapted from the 2021 British Society of Haematology / UK Myeloma Forum guidelines3
It is important to note that a paraproteinaemia is not specific for myeloma-related disease. Other important differentials include Waldenström's macroglobulinaemia, chronic lymphocytic leukaemia, cryoglobulinaemia, POEMS (polyneuropathy, organomegaly, endocrinopathy, myeloma protein and skin changes) syndrome and amyloid light-chain (AL) amyloidosis, with the latter often co-existing with myeloma and causing symptoms of nephrotic syndrome, heart failure, neuropathy and macroglossia.
Management options9
Every patient should be reviewed in a multidisciplinary team (MDT) meeting prior to starting treatment. The MDT includes haematologists, specialist nurses, microbiologists, radiologists, occupational therapists, physiotherapists, dietitians and psychologists. The patient's performance status and opinion should be incorporated into an appropriate treatment approach, as will their eligibility for stem cell transplant.
Myeloma is currently viewed as a treatable but incurable condition and newly diagnosed myeloma patients should receive regular monitoring throughout their treatment with input from a clinical nurse specialist. The goal is to obtain biochemical and clinical remission from the disease. Those with smouldering myeloma should be reviewed every 3 months by a haematologist for the first 5 years following diagnosis, depending on disease stability. MGUS monitoring can take place in primary care, with the frequency of testing determined following an initial haematology review. In patients monitored in primary care, re-referral criteria to the haematology service should be determined to ensure possible progression is acted on accordingly.
First-line therapy in patients with confirmed myeloma usually involves proteasome inhibitors (such as bortezomib) or immunomodulatory drugs (such as thalidomide).3 Side effects of both medications may include peripheral neuropathy. These medications are usually used in combination with high-dose corticosteroids (dexamethasone) with dose adjustments required based on the side effect profile exhibited by the patient, including gastro-intestinal irritation and psychosis. Immunomodulatory drugs (such as thalidomide) have an increased risk of venous thromboembolism, therefore, patients need to be on a suitable anti-coagulant, plus a pregnancy prevention programme. Monoclonal antibody therapies (such as the anti-CD38 monoclonal antibody daratumumab) are also now available but can also interfere with blood grouping; the need for supportive blood products should be anticipated to allow for delays in supply. In fit patients, usually below the age of 70 years, autologous stem cell transplantation is recommended to consolidate response to first-line treatment and is now followed by maintenance therapy with single agent lenalidomide, which has been recently approved by NICE.10
Primary care physicians can support MM patients by ensuring that infections are treated promptly with broad spectrum antibiotics, optimising analgesia, and identifying and referring urgently if new symptoms (such as bone pain or neurological compromise) are apparent. Patients should receive the annual vaccination against influenza, the one-off pneumococcal vaccination and the booster dose of the COVID-19 vaccination. Primary care may also be involved in supportive care alongside community palliative care.
- © Royal College of Physicians 2022. All rights reserved.








{kind=link}