
ABSTRACT
Regular chronic kidney disease (CKD) screening can facilitate earlier diagnosis of CKD and preventative action to reduce the risk of CKD progression. People with type 2 diabetes are at a higher risk of developing CKD; hence, it is recommended that they undergo annual screening. However, resources may be limited, particularly in lower-to-middle income countries, and those at the highest risk of having an abnormal CKD screening result should be prioritised for screening. We have developed models to determine which patients are at a high risk of renal impairment. We have shown that, for people with type 2 diabetes and no previous diagnosis of CKD stage 3–5, it is possible to use age, gender, body mass index, duration of type 2 diabetes and blood pressure information to detect those at a higher risk of a reduced glomerular filtration rate. When blood measurements are available, triglyceride and cholesterol measurements can be used to improve the estimate of the risk. Even though risk factors were associated with an increased urine albumin:creatinine ratio, we found no clinical benefit of using the model over a screen-all approach.
Introduction
Chronic kidney disease (CKD) is a recognised global health problem, with a prevalence of more than 9%, associated with cardiovascular complications and mortality.1 Diabetes is a well-known risk factor for CKD and acts as a catalyst for CKD progression and it is the leading cause of kidney failure.1–5 Early detection of CKD is, therefore, particularly important in people with diabetes to initiate preventative interventions that slow progression.6 However, with the expected increase of people with diabetes, this imposes a monumental demand on screening practices.7
CKD screening often involves the measurement of estimated glomerular filtration rate (eGFR) and urine albumin:creatinine ratio (uACR). The National Institute for Health and Care Excellence and the American Diabetes Association promote annual screening of CKD among patients with type 2 diabetes mellitus (T2DM).8,9 However, in practice, not all patients complete these checks; the UK national diabetes audit 2019/2020 reported that only 61.1% had a measurement of urine albumin and 94.4% had a measurement of serum creatinine, which has more recently decreased to 52.7% and 85.7%, respectively, with the onset of the COVID-19 pandemic.10
In addition, availability of healthcare resources vary globally. In lower-to-middle income countries, resources are limited and annual screening is not commonplace. Consequently, patients tend to receive reactive care rather than proactive prevention.11 Due to the asymptomatic nature of CKD in its early stages, patients can go undiagnosed or are diagnosed late.12 This can result in overall worsening health that may be irreversible. Therefore, there is a need for a tool to identify those who should be prioritised for screening to facilitate earlier diagnosis and earlier treatment, when resources are limited.
Methods
Design, data source and ethics
We carried out a retrospective, observational study, utilising data provided by 22 UK primary care centres that agreed to share pseudonymised patient-level data. A data sharing agreement was in place with each of the practices for all people with T2DM that did not choose to opt-out via the national data opt-out service. This was approved by the Health Research Authority, and Health and Care Research Wales.
Primary outcomes
Our primary outcomes measured on or after 01 January 2020 consisted of:
eGFR <60 mL/min/1.73m2 (via an eGFR entry or derived from a serum creatinine entry, described in the supplementary material S1)
uACR ≥30 mg/g.
Population
Our study population consisted of patients that were 18 years old and above with a diagnosis of type 2 diabetes and no diagnosis of CKD stage 3–5, prior to the eGFR/uACR measurement.
Candidate predictors
Diabetes-related care measures and patient information were selected as candidate predictors: age, gender, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure (DBP), duration of type 2 diabetes, total cholesterol, ratio of high-density lipid (HDL) to total cholesterol, glycated haemoglobin (HbA1c), triglycerides and ethnicity. Two versions of the model were considered: one using all the variables (termed the full model) and one using a subset (termed a minimal-resource model) excluding ethnicity and the measurements that require laboratory testing (ie including only age, gender, BMI, SBP, DBP and duration of type 2 diabetes).
Given that the data available were routinely collected, we expected that the measurements of predictors would likely be taken on a different day to the outcome measurement. The process for selecting or interpolating a value, where appropriate, is described in the supplementary material S1.
Missing data
For continuous variables, predictive mean matching within multiple imputation chained equations was performed for missingness below 60% using 20 iterations. Categorical variables were imputed with the mode.
Statistical methods
The baseline characteristics of the patients at the time of outcome measurement were analysed. Continuous variables were evaluated using the mean and standard deviation or median and interquartile range for normal and non-normal distributions, respectively. Chi-squared testing was applied to test for differences in proportions, where appropriate. Logistic regression was applied to the data where the functional forms of the variables were selected a priori according to clinical expertise. Sample sizes were sufficient for model development according to post hoc calculations.13 Internal bootstrap validation using 200 iterations was applied to estimate the optimism of the model performance metrics. We present the optimism-adjusted positive predictive value (PPV) and sensitivity, and their bootstrap 95% confidence intervals (CIs). The aim of the model was to improve the PPV without reducing the sensitivity below 80%. Therefore, a threshold was selected where the lower bound of the optimism-adjusted sensitivity 95% CI was above 80%.
Results
Summary statistics
A total of 13,127 patients with type 2 diabetes were identified, of whom, 1,402 (10.7%) had a diagnosis of CKD stage 3–5 before 01 January 2020. After removing measurements that occurred before the first recording of type 2 diabetes or after a diagnosis of CKD stage 3–5, 9,423 patients had at least one valid uACR or eGFR (uACR n=6,090; eGFR n=9,297; supplementary material S1, Fig S1). Table 1 describes the demographic data of patients, grouped by measurement. There were 1,521 (25.0%) patients with a uACR ≥30 mg/g (1,312 with uACR of 30–300 mg/g and 209 with uACR of >300 mg/g) and 1,405 (15.1%) had an eGFR <60 mL/min/1.73m2.
Baseline patient demographics at the time of estimated glomerular filtration rate and urine albumin:creatinine ratio measurement
Of those with a selected eGFR measurement, 3,333 (35.9%) did not have a selected uACR measurement, of whom, 2,551 (27.4%) did not have any evidence of urine microalbumin testing. The proportion of patients without evidence of urine microalbumin testing with an eGFR <60 mL/min/1.73m2 was not significantly different from those with evidence of urine microalbumin testing (412 (16.1%) with no test vs 993 (14.7%) with a test; p=0.09). In patients with both an eGFR and uACR (n=5,964), positive results were correlated; the proportion of patients with a reduced eGFR was greater in those with a raised uACR (10.5% with uACR of <30 mg/g vs 25.7% with uACR ≥30 mg/g; p<0.001; supplementary material S1, Table S1).
Model performance
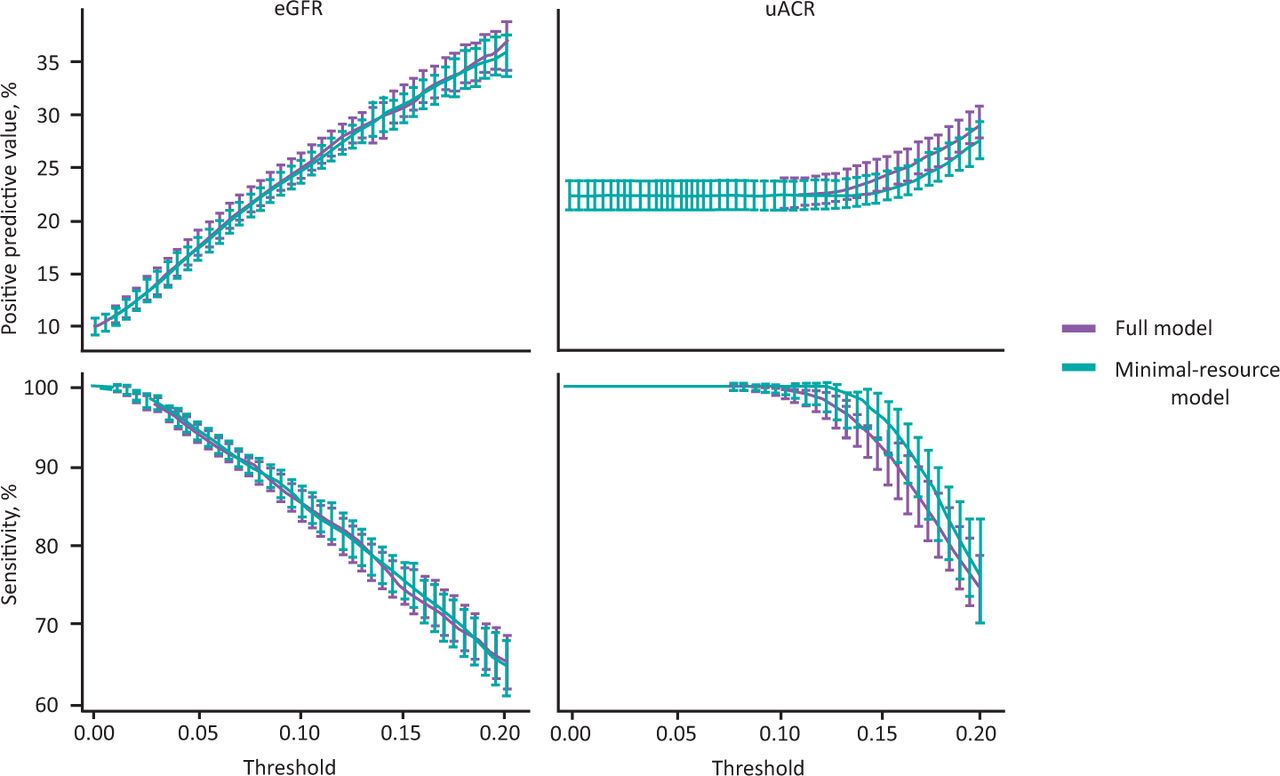
For the uACR models, the PPV increased from 0.250 (95% CI 0.239–0.260) to 0.271 (95%CI 0.261–0.285) using the minimal-resource model and to 0.279 (95% CI 0.269–0.293) with the addition of blood measurements and ethnicity (Fig 1). These correspond to relative improvements of 8.5% and 11.7%, respectively. Patients that were older, had a longer duration of T2DM, had higher blood pressure measurements and had a higher BMI were associated with an increased risk of a raised uACR within the minimal-resource model. A higher HbA1c was also associated with an increased risk of a raised uACR, but no other blood measurements within the full model were found to be statistically significant. Ethnicity and gender were not found to be statistically significant in the models. While BMI was statistically significant in the minimal-resource model, this was not the case in the full model.

Optimism-adjusted positive predictive value and sensitivity of models to predict the probability of an estimated glomerular filtration rate <60 mL/min/1.73m2 or a urine albumin:creatinine ratio ≥30 mg/g. eGFR = estimated glomerular filtration rate; uACR = urine albumin:creatinine ratio.
For the eGFR models, the PPV increased from 0.151 (95% CI 0.144–0.157) to 0.282 (95% CI 0.271–0.294) using the minimal-resource model and to 0.286 (95% CI 0.276–0.298) with the addition of the blood measurements and ethnicity (Fig 1). These correspond to an 86.3% and 90% relative improvement, respectively. In the full model, being a woman, being Asian or Asian British, being Black or Black British, being older, having a longer duration of diabetes, having a higher BMI and having more triglycerides were each associated with an increased risk of a reduced eGFR. Increased total cholesterol and ratio of HDL to total cholesterol were associated with a reduced risk of a reduced eGFR. However, in the minimal-resource model, being a woman was no longer associated with a reduced eGFR.
Discussion
Our study has demonstrated that it is possible to identify a significantly smaller target population for eGFR priority screening using a small number of non-invasive risk factors. We found that there was little additional benefit of including invasive clinical parameters (ie blood measurements) compared with these minimal-resource models. The improvement in PPV demonstrated by the minimal-resource eGFR model is promising for screening practices where resources are limited: the 86.3% improvement corresponds to reducing the screening population by 46.3%. Given that a reduced eGFR is indicative of deterioration, it could be argued that these patients are most in need of review and should be prioritised.
The disparity between the uACR and eGFR model performances can be explained by several factors. Firstly, the clinical nature of these measures is known to be different. In the CKD trajectory, a patient's uACR will usually raise before they exhibit glomerular hypofiltration.14 Additionally, it is expected that, as patients age, their eGFR will naturally reduce but the corresponding pattern is not the case for uACR.15 Secondly, the practices around each of the tests differ. The uptake of uACR remains low compared with eGFR within UK primary care and, unlike for eGFR, an alternative urine protein test (eg a dipstick urine test) may be performed prior to uACR testing, potentially resulting in uACR data being available for only a subset of the population. However, we found no evidence that being tested for microalbuminuria was associated with a reduced eGFR, suggesting that the difference in uptake may not be correlated with expected CKD severity.
With primary care services being reduced or suspended during the COVID-19 pandemic, we have observed a reduction in adherence to annual screening. In particular, serum creatinine measurement reduced from 94.4% to 85.7% in patients with T2DM in England (2020/2021). While this is still a high overall performance, those that went untested were in excess of 660,000 people. Therefore, it may be sensible to prioritise those patients without any recent measurements who are predicted at high risk of an abnormal test result using our tool.
Common to the CKD prediction literature, our models were developed using a single measurement.16 However, the definition of CKD requires sustained kidney damage for at least 3 months. Therefore, we do not propose that our tool replaces diagnostic testing, but simply offers a solution to target screening resources towards those most in need. The tool should be considered as a pathway to access screening services where it is not feasible to screen everyone. For those that are screened and do not have an abnormal result, this information can be utilised in a more sophisticated model to predict the onset of CKD in the future, with the potential to trigger early prevention.17
Many models to predict CKD in people with T2DM already exist.18 However, the focus in the literature remains on prognostic modelling (ie predicting a future diagnosis of CKD), whereas we have modelled a patient's risk of currently experiencing renal impairment. Similar tools have been proposed for the general population but our models are specific to patients with diabetes and highlight that diabetes is likely to interact with risk factors.19,20 General population models have not accounted for this. In addition, we considered models for both uACR and eGFR, whereas the literature tends to focus on eGFR only. Taking this approach, we have found that few of the variables associated with a reduced eGFR are also associated with a raised uACR. This is an important result, especially given the interest to identify patients before they experience any reduction in their eGFR.
While the difference in performance between the full and minimal-resource models was modest, we would advise that where additional information is available, it is utilised. However, we expect that such information is unlikely to be well-captured within lower-to-middle income countries, hence, the minimal-resource model is likely to be most appropriate. Supporting a change in resource-limited healthcare settings could offer an opportunity to reduce the burden of CKD in diabetes patients via earlier detection and decrease health inequalities.
Limitations
The routinely collected data for the candidate predictors was rarely taken on the day of the outcome measurement. Therefore, it may be expected that the in-practice model performance differs to the performance we observed within our study. Further, confounders (such as comorbidities and pharmaceutical therapies) were not well captured in the model due to data limitations. Including these may help improve the accuracy and precision of the model estimates. Additionally, the data on which the models were developed is from UK primary care. Validation within international cohorts is required before applying them in global markets since the generalisability will be influenced by population health and standard care practices including, but not limited to, diabetes care. In settings where screening is routinely performed and clinical information is regularly recorded, a more appropriate model could be developed, utilising a patient's historical data.
Conclusion
It is feasible to use non-invasive measurements to identify patients with type 2 diabetes that are likely to be currently experiencing renal impairment. Our minimal-resource model to predict a reduced eGFR can be used to target patients that are a high priority for CKD screening. We expect that the tool could assist with prioritisation of screening resources, particularly in lower-to-middle income countries.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/fhj:
S1 – Data wrangling protocol, exclusion diagram and contingency table.
Acknowledgements
The authors would like to thank the general practices that agreed to share the data used in this study as well as the team at Wellbeing Software that have supported the data extraction. In particular, we would like to thank Dr Alison Heaton (Teams Medical Practice, Gateshead), Dale Carter (Clifton Medical Centre, Rotherham), Jane Roper (East Hertfordshire GP Cluster), Dr Jagjit Takhar (Parsonage Surgery, Bishop's Stortford), New Wokingham Road Surgery (Crowthorne), Dr Matt Hoghton (Clevedon Medical Centre, Clevedon) and Daniel James Murphy (Honiton Surgery, Honiton) for their support in providing data for this study.
- © Royal College of Physicians 2022. All rights reserved.
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.